










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.2 Porto Alegre Abr./Jun. 2013
CLÍNICO / CLINICAL
Non-nutritive sucking associated with self-mutilating behavior
Hábito de sucção não-nutritiva associada à automutilação
Renata Cristiane da SILVAI; Fabiano JEREMIASII; Lourdes SANTOS-PINTOII; Angela Cristina Cilense ZUANONII
I Universidade Camilo Castelo Branco, Câmara Especial de Pós-Graduação e Pesquisa. São Paulo, SP, Brasil.
II Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia, Departamento de Clínica Infantil. Rua Humaitá, 1680, Araraquara, SP 14801-930, Brasil.
ABSTRACT
Although sucking activity has been considered an essential behavior of early childhood to satisfy nutritive and non-nutritive needs, digit and pacifier sucking are deleterious oral habits that may interfere with child development. Furthermore, this clinical picture may be compounded by other concerning habits, such as self-mutilating behavior. This article reports 4-year follow-up of a child in whom non-nutritive sucking was associated with an unusual self-mutilating behavior; namely, the child would pull out her own hair after wrapping it around her finger every time she sucked on the pacifier. This occurred specially at bedtime, while she was watching TV, or when she was somewhat anxious, and remitted and recurred throughout the follow-up period. In an attempt to address this behavior, pacifier use was discontinued and the child's head was shaved. Ultimately, the case was only solved through combined efforts involving the child, her family, and health professionals. Based on the parents' reports and clinical examination and follow-up findings, we emphasize the importance of investigating the origin of the problem and considering emotional aspects and its association with other habits in such cases.
Indexing terms: Child. Pacifiers. Self mutilation.
RESUMO
Apesar de a atividade de sucção ser considerada um comportamento essencial da primeira infância por satisfazer as necessidades nutritivas e não-nutritivas, a sucção do dedo e chupeta são hábitos deletérios ao desenvolvimento da criança. Além disso, esse quadro clínico pode ser ainda mais preocupante se houver associação com outros hábitos, como o da automutilação. Neste contexto, no presente artigo são relatados 4 anos de acompanhamento de uma criança que costumava arrancar seus cabelos depois de enrolá-los nos dedos enquanto estava com a chupeta na boca, sem demonstrar sinal algum de sintomatologia dolorosa. Tal fato ocorria especialmente próximo a períodos de sono, ansiedade ou quando assistia à televisão, havendo períodos de remissão e exacerbação. Na tentativa de solucionar o caso foi proposta, além da interrupção do uso da chupeta, a raspagem de todo o cabelo da criança. Contudo, a solução definitiva só foi possível quando houve o envolvimento coletivo, abrangendo criança, família e profissionais da saúde. Baseando-se no relato dos pais, no exame clínico e no acompanhamento do caso, enfatiza-se a importância de se investigar a origem do problema, considerando os aspectos emocionais e sua associação com outros hábitos.
Termos de indexação: Criança. Chupetas. Automutilação.
INTRODUCTION
Sucking activity in the first years of life is considered an essential behavior of early childhood to meet nutritive and non-nutritive needs1. However, habitual digit and pacifier sucking are considered extremely deleterious to normal child development2.
Prolonged or chronic digit or pacifier sucking may predispose to dental conditions such as dental caries2 and malocclusion3-5, and is associated with acute otitis media6 and with some psychological disorders, including depression, as well as colic7-9. Pacifier use has been associated with development of latex allergy in infants10, and pacifiers may serve as fomites for dissemination of microorganisms among children, leading to bacterial and fungal infections and reinfections8, as in previous reports of increased Candida albicans colonization associated with pacifier use9. According to Kramer et al.11, pacifier use discourages breastfeeding and contributes to early weaning. Furthermore, infants who are weaned early are more likely to use pacifiers than those who are breastfed for longer.
In view of the foregoing, digit and pacifier sucking are habits to be avoided. When complete avoidance is not possible, they should be kept to a minimum; neither habit should be encouraged beyond the first year of life. This article seeks to report the 4-year follow-up of a child who exhibited self-mutilating behavior (infant trichotillomania) associated with pacifier use.
CASE REPORT
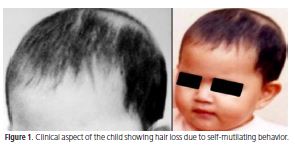
A female infant was referred with a complaint of trichotillomania associated with pacifier use. While sucking her pacifier, the child would wrap her head hair around her fingers and pull it out without displaying any outward sign of pain (Figure 1). Both parents worked outside the home and the child had been in daycare since age 40 days.
The child had no medical conditions and no past medical history or family history of note. As soon as they noticed the child's hair loss, the parents sought the advice of their pediatrician, who attributed this behavior to pacifier use.
After a comprehensive assessment, the parents were informed of the risks and consequences of this selfmutilating habit and of the importance of terminating it as soon as possible. The pediatrician also recommended that the child's head be shaved completely. The child's parents followed all recommendations, but only head-shaving was successful, and temporarily so, as the child reverted to her previous behavior as soon as her hair had grown long enough to pull.
At age 18 months, the child was taken out of daycare because her mother had stopped working outside the home. Interestingly, as the child was able to spend more time with her mother, her hair-pulling behavior ceased completely and her pacifier use was rapidly and substantially reduced, until it was limited to bedtime.
At age 4 years, the child was sent to preschool as her mother had to return to work. Subsequently, the child reverted to occasional hair-pulling during pacifier use. The behavior was particularly pronounced at bedtime, while watching TV, or when the child was somewhat anxious, and was quickly curtailed by the mother, who warned the child and told her why she should not pull out her hair. Nevertheless, slight hair loss on the forehead and back of the neck was noticed.
In view of the persistence of this behavior and its manifest consequences, the parents sought advice from a pediatric dentistry specialist, who helped them along the encouragement process to assist the child in discontinuing pacifier use definitively. Within 1 year, both behaviors (pacifier use and hair-pulling) had ceased completely. The child's understanding and cooperation were determining factors in the success of this intervention.
Throughout the follow-up period, the child exhibited recurring episodes of severe otitis media. Furthermore, due to her pacifier use, she had maxillary constriction and a mild acquired deformity of the hard palate. Orthodontic treatment was planned to address these conditions.
The authors stress that all procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki (2000) and with current Brazilian legislation. The child's legal guardians provided written informed consent for the publication of this report.
DISCUSSION
Sucking is an important reflex in the first weeks of life. Breastfeeding confers benefits both in terms of its nutritive aspect and by satisfying the child's sucking instinct12. The World Health Organization13 recommends exclusive breastfeeding in the first 6 months of life and mixed feeding (supplemented by other foods) thereafter until age 2. Children who are not breastfed, for a variety of reasons, usually meet their sucking needs by using a dummy or pacifier. There is strong evidence that pacifier use reduced motivation for breastfeeding and contributes to early weaning and other non-nutritive sucking habits1,3,11 . According to Juberg et al.1, pacifier use is among the most common oral habits in the first 36 months of life. This is because the decision to use a pacifier rests entirely with the child's parents or guardians, who provide it. Pacifiers are a common item in layette sets, and their use is often widely encouraged by family members.
The most serious hazards of this non-nutritive sucking habit are interference with breastfeeding, dental deformities, and the risk of accidents. Latex allergy, tooth loss, oral ulcers, and sleep disorders are also associated with pacifier use14, which also increases fungal colonization and proliferation in the oral cavity10. Furthermore, this habit has been associated with acute otitis media; the incidence and severity of infection were found to decrease after a reduction in daily pacifier use, which suggests that pacifier sucking is a risk factor for ear infection6. The child described in this report also had recurrent episodes of otitis media, which led to several doctor's appointments and courses of pharmacological therapy. The child's ear infections only improved after her pacifier sucking habit was reduced.
With continuous pacifier sucking, the child developed dental–skeletal alterations over time, including anterior open bite and posterior crossbite. These changes are commonly observed in children with a pacifier sucking habit, and depend on the frequency, duration, and intensity of pacifier use, as well as on the position of the teeth, on heredity, and on the child's age and overall health12,15-17. Likewise, spontaneous correction after cessation of the habit depends on the aforementioned variables and on the severity of malocclusion. Therefore, it is imperative that parents be informed and instructed as to the consequences of pacifier use so they can intervene at the proper age. Parental intervention notwithstanding, the child's cooperation is essential to the success of any therapy.
Juberg et al.1 stress that sucking habits decrease with advancing age, following the pattern of normal child development. Indeed, this child's pacifier use decreased over time, to the point where it was eventually restricted to bedtime or to times of particular anxiety. According to several authors11-12,15,18-21, some children engage in pacifier sucking more intensely than others. This fact may be explained by emotional aspects, as well as by social, domestic, cultural, and economic influences. Pacifier use is known to temporarily curtail crying or fussing in certain situations, but when used regularly, it may encourage or induce deleterious behaviors instead11.
During the course of follow-up, we observed that the child's most severe pacifier sucking and hair-pulling behaviors coincided with the hours she spent in daycare. Therefore, her behaviors were probably an attempt to secure attention, particularly parental attention, with pacifier use serving as something of a self-comforting habit. We believe that development of this habit was directly related to early weaning of the child and to the absence of her parents, both of whom worked outside the home. The child appeared somewhat emotionally needy. Nevertheless, no psychological care or counseling was provided, despite our recommendations.
The literature stresses that the essential purpose of breastfeeding is to ensure frequent physical contact the mother and child. The reciprocal psychological and physiological benefits of breastfeeding to the mother–child pair in this symbiotic relationship play a vital role in normal child development. Touch is a basic behavioral need, just as breathing is a basic physical necessity; infants are destined to grow and develop socially by means of contact with others, and this need for contact will persist throughout the life course. If children are to develop properly, they must be touched, held, carried, caressed, embraced, and lovingly spoken to, even when breastfeeding is lacking. The emphasis is on the care and embracement provided by touch from the hands, arms, and lap; it appears that, even in the absence of many other stimuli, these are essential calming experiences that infants require to survive with at least some health. Humans are able to survive extreme deprivation of other senses, including deprivation of visual and auditory stimuli, as long as the sensory experience of skin contact is provided22.
Within this context, we stress the importance of multidisciplinary guidance and monitoring of child development in these cases. As far as the role of the dental practitioner is concerned, it is recommended that children first see a pediatric dentist between the ages of 4 and 6 months19. This is a crucial age in which the professional can provide guidance and help prevent certain habits. Pacifiers can be a helpful childcare tool in some situations, but they should not be used as a source of emotional support.
CONCLUSION
We conclude that parental unavailability (particularly on the part of the mother) and early weaning played a key role in the development of deleterious habits (pacifier use and self-mutilating behavior) in this child. The child's emotional habits and lifestyle were modified in an attempt to induce cessation of these habits. This strategy was ultimately successful, but a multidisciplinary approach was required.
Collaborators
RC SILVA, F JEREMIAS, L SANTOS-PINTO, and ACC ZUANON all contributed to the drafting of the manuscript.
REFERENCES
1. Juberg DR, Alfano K, Coughlin RJ, Thompson KM. An observational study of object mouthing behavior by young children. Pediatrics. 2001;107(1):135-142. doi: 10.1542/ peds.107.1.135. [ Links ]
2. Ollila P, Niemelä M, Uhari M, Larmas M. Prolonged pacifier sucking and use of a nursing bottle at night: possible risk factors for dental caries in children. Acta Odontol Scand. 1998;56(4):233-7.
3. Karjalainen S, Ronning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediat Dent. 1999;9(3):169-73. doi: 10.1046/j.1365-263x.1999.00133.x.
4. Farsi NMA, Salama FS. Sucking habits in Saudi children: prevalence contributing factors and effects on the primary dentition. Pediatr Dent. 1997;19(1):28-33.
5. Fukuta O, Braham RL, Yokoi K, Kurosu K. Damage to the primary dentition resulting from thumb and finger (digit) sucking. J Dent Child. 1996;63(6):403-7.
6. Niemalä M, Pihakari O, Pokka T, Uhari M, Uhari M. Pacifier as a risk factor for acute otitis media: a randomized, controlled trial of parental counseling. Pediatrics. 2000;106(3):483-8. doi: 10.1542/peds.106.3.483.
7. Stone KN, Fleming P, Golding J. Socio demographic associations with digit and pacifier sucking at 15 months of age and possible associations with infant infection. Early Human Development 2000;60(2):137-48. doi: 10.1016/S0378-3782(00)00113-4.
8. Brook I, Gober AE. Bacterial colonization of pacifiers of infants with acute otitis media. J Laryngol Otol. 1997;111(7):614-5. doi: 10.1017/S0022215100138113.
9. Freishtat RJ, Goepp JG. Episodic stridor with latex nipple use in a 2-month-old infant. Annals Emerg Med. 2002;39(4):441-3. doi: 10.1067/mem.2002.122771.
10. Mattos-Graner RO, Moraes AB, Rontani RMP, Birman EG. Relation of oral yeast infection in Brazilian infants and use of a pacifier. ASDC J Dent Child. 2001;68(1):33-6.
11. Kramer MS, Barr RG, Dagenais S, Yang H, Jones P, Ciofani L, et al. Pacifier use, early weaning and cry/fuss behavior. A randomized controlled trial. JAMA. 2001;286(3):322-6. doi: 10.1001/jama.286.3.322.
12. Vieira AR, Modesto A. Pacifier-sucking associated with a bizarre habit: a case report. J Clin Pediatr Dent. 2000;24(3):187-9.
13. World Health Organization. Expert Consultation on Optimal Duration of Exclusive Breastfeeding. Geneva: World Health Organization; 2001.
14. Cinar DN. The advantages and disadvantages of pacifier use. Contemp Nurse. 2004;17(1-2):109-12.
15. Queluz DP, Aidar JM. Dummy: a pernicious habit? J Bras Odontopediatr Odontol Bebe. 1999;2(8):321-7.
16. Duncan K, McNamara C, Ireland AJ, Sandy JR. Sucking habits in childhood and the effects on the primary dentition: findings of the Avon Longitudinal Study of Pregnancy and Childhood. Int J Paediatr Dent. 2008;18(3):178-88. doi: 10.1111/j.1365- 263X.2007.00905.x.
17. Peres KG, Barros AJD, Peres MA, Victora CG. Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saúde Pública. 2007;41(3):343-50. doi: 10.1590/S0034-89102007000300004.
18. Mascarenhas CF. Sucção de chupeta: qual a razão da utilização da chupeta no recém-nascido? Rev Fono Atual. 1999;10:25-8.
19. Zuanon ACC, Zuanon JAS, Giro EMA, Hebling J. Analyses of oral interactions presents in children with ages varying from 0 to 3. J Dent Res. 1998;77:1183-322.
20. Levy SM, Slager SL, Warren JJ, Levy BT, Nowak AJ. Associations of pacifier use, digit sucking, and child care attendance with cessation of breastfeeding. J Fam Pract. 2002;51(5):465.
21. Warren JJ, Bishara SE. Duration of nutritive and nonnutritive sucking behaviors and their effects on the dental arches in the primary dentition. Am J Orthod Dentofacial Orthop. 2002;121(4):347-56. doi: 10.1067/mod.2002.121445.
22. Montagu A. Tocar. O significado humano da pele. 10th ed. São Paulo: Summus; 1998.
 Endereço para correspondência:
Endereço para correspondência:
ACC ZUANON
e-mail: aczuanon@foar.unesp.br
Received on: 8/10/2009
Final version resubmitted on: 12/1/2011
Approved on: 7/4/2011
