










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.3 Porto Alegre Jul./Set. 2013
ORIGINAL / ORIGINAL
Pain control with dexamethasone, etoricoxib or ibuprofen associated with arginine in impacted third molar surgery
Analgesia pós-operatória em exodontias de terceiros molares mandibulares inclusos: estudo comparativo com dexametasona, etoricoxibe e ibuprofeno associado à arginina
Alessandro Hyczy LISBOAI; Gibson Luiz PILATTI
I Universidade Estadual de Ponta Grossa, Faculdade de Odontologia. Av. Gen. Carlos Cavalcanti, Uvaranas, 84030-900, Ponta Grossa, PR, Brasil.
ABSTRACT
Objective
The aim of this study was to perform a comparative evaluation of postoperative analgesia associated with ibuprofen arginine, etoricoxib and dexamethasone in bilateral extractions of mandibular third molars.
Methods
TFourty two volunteers (12 men and 30 women), took part in this randomized, blinded, parallel, clinical trial and were divided into 4 groups: group 1, who received 600mg of ibuprofen and 555mg of arginine, G2, treated with 90 mg etoricoxib, G3, receiving 8 mg dexamethasone and G4, treated with a placebo, administered orally 90 minutes prior to surgery. Pain intensity was assessed using a 101 point numerical scale (101P) and a 4-point verbal scale (VRS) after 2, 4, 6, 8, 12, 24, 36 and 48 hours. For the statistical analysis of the data,the Kruskal-Wallis test was employed (p≤0.05).
Results
The results showed that volunteers in G4 exhibitedmore pain than the other groups, at 4 and 12 hours. The G3 showed higher pain intensity than G2 at 2 hours via the VRS and at 6 hours with the 101P, and in comparison with G1 after 4 and 6 hours with the 101P. There was a statistical difference between G4 and G3 and between G4 and G2 when comparingthe consumption of pain relievers.
Conclusion
It was concluded that all the drugs evaluated promoted postoperative analgesia when compared to the placebo. The analgesic consumption is lower when employing etoricoxib or dexamethasone. This work filed inthe Clinical Trials Registerunder no.U1111-1129-1722.
Indexing terms: Anti-inflammatory agents. Molar third. Tooth extraction.
RESUMO
Objetivo
Avaliar, de forma comparativa, a analgesia pós-operatória com o ibuprofeno associado à arginina, etoricoxibe e dexametasona, em exodontias bilaterais de terceiros molares inferiores inclusos.
Métodos
Tomaram parte deste estudo clínico randomizado, paralelo e cego 42 voluntários (12 homens e 30 mulheres), que foram divididos em 4 grupos: grupo 1, que receberam 600mg de ibuprofeno e 555 mg de arginina; grupo 2, tratados com 90 mg de etoricoxibe; grupo 3, que receberam 8 mg de dexametasona e o grupo 4, tratados com placebo, administrados por via oral, 90 minutos antes da cirurgia. A intensidade da dor foi avaliada por meio de uma escala numérica de 101 pontos (101P) e de uma escala verbal de 4 pontos (VRS), após 2, 4, 6, 8, 12, 24, 36 e 48 horas. Na análise estatística dos dados foi empregado o teste de Kruskall-Wallis (p≤0,05).
Resultados
Os resultados mostraram que os voluntários do grupo 4 acusaram maior intensidade de dor do que os demais grupos, nos períodos de 4 e 12 horas. O grupo 3 apresentou maior intensidade de dor do que grupo 2 no tempo de 2 horas pela escala verbal de 4 pontos e após 6 horas pela escala numérica de 101 pontos, e em relação ao grupo 1 após 4 e 6 horas pela escala numérica de 101 pontos. Houve diferença estatística entre grupo 4 e grupo 3, e entre grupo 4 e grupo 2 na comparação do consumo de analgésicos de resgate.
Conclusão
Concluiu-se que todos os fármacos avaliados promoveram analgesia pós-operatória se comparados ao placebo. O consumo de analgésicos é menor quando se emprega o etoricoxibe ou a dexametasona. Registro de Ensaios Clínicos: U1111-1129-1722.
Termos de indexação: Anti-inflamatórios. Dente serotino. Extração dentária.
INTRODUCTION
Extractions of impacted mandibular third molars generally cause patients discomfort, making it difficult for them to cope with their normal routines. The postoperative phase is characterized by signs and symptoms such as pain, edema, restricted opening of the mouth and potential loss of function, due to the inflammatory response to the surgery1. This inflammatory response, however, is often excessive, more accentuated than is required for the tissue repair process.
Pain, edema and the control of anxiety in patients are probably the biggest concerns for the dental surgeon when planning the extraction of impacted mandibular third molars2. It is necessary, therefore, for the professional to establish a medication protocol to minimize these concerns3.
Preemptive analgesia is one concept that has aroused a lot of interest recently, and is the subject of research studies in the fields of medicine and dentistry. It is defined as an analgesic regimen which begins before the noxious stimulus, with the aim of preventing hyperalgesia,and the consequent stimulus which amplifies the pain. It differs from the regimen of preventive analgesia, when the analgesic medication is introduced after tissue trauma resulting from surgery, though prior to the commencement of the painful sensation, after the effects of the local anesthetic have worn off4.
In a randomized, double-blind, placebo-controlled study of 498 patients submitted to third molar surgery, the pure form of ibuprofen (200 mg or 400 mg) was compared to ibuprofen (200 mg or 400 mg) combined with arginine, and it was demonstrated that the ibuprofen/arginine combination provided a faster analgesic effect (28 minutes for 200 mg and 29 minutes for 400mg) when compared with ibuprofen by itself (52 minutes with 200mg and 44 minutes with 400mg)5.
In a separate clinical study, using the model of a bilateral extraction of impacted mandibular third molars, on 50 patients, it was concluded that an8mg dose of dexamethasone, administered 2 hours prior to the surgical procedure, significantly reduces postoperative pain and edema, when compared to the placebo group6.
Dexamethasone is quite widely used to minimize pain, and principally edema, after third molar extractions. Despite this, researchers have suggested further studies using Prostaglandin-endoperoxide synthase-2 (COX- 2) selective inhibitors for oral surgery7-8. A number authors have stated that corticosteroids should be used for extractions that require osteotomy or in procedures that cause considerable tissue trauma, as for the majority of patients, oral medication is convenient, economical and a safe way of administering this medication9.
Etoricoxib is a COX-2 selective inhibitor antiinflammatory drug which has been shown to be effective in treating pain, having a rapid response and prolonged effect. When comparing etoricoxib doses of 60mg, 120mg, 180mg and 240mg, the conclusion was reached that the lowest dose for obtaining maximum effectiveness in the control of post-extraction pain was 120mg10. Other authors compared the use of a pre-operative120 mg dose of etoricoxib prior to the extraction of mandibular third molars and a 4mg dose of dexamethasone. These authors found that both are effective in controlling postoperative pain and that there was no statistical difference between the two groups11.
Researchers have pointed out that in single-dose situations, the COX-2 selective inhibitors demonstrated a longer duration of analgesic action when compared to ibuprofen12.
In yet another trial which compared the effectiveness of celecoxib and dexamethasone in the prevention and control of postoperative pain in periodontal surgery, the authors recommend further studies on the subject, employing the model of the bilateral extraction of impacted mandibular thirdmolars13.
In the literature, different medication protocol scan be found for controlling pain and edema after the extraction of impacted mandibular third molars1,10-14-16, however there is still no consensus on the topic. So the present study proposed to test if anti-inflammatory drugs of different groups (one corticosteroid, one COX-2 selective non-steroidal anti-inflammatory drug and one nonselective combined with arginine), promote postoperative analgesia with this type of surgery.
METHODS
In this randomized, parallel and blind clinical study, a total of 42 volunteers was selected from both sexes (12 men and 30 women), aged between 18 and 43, who were cared for in the dental clinic at the integrated faculties of the Campos Gerais Higher Education Center (CESCAGE), referred for the removal of impacted mandibular third molars, after anamnesis, physical examination and X-ray. The stratification was carried out according to the position of the third molar using the Pell & Gregory17 and Winter18 classifications.
The exclusion criteria were as follows: chronic use of painkillers, anti-inflammatory, anticoagulant orantiplatelet drugs during the previous 6 months, pregnant or lactating women, or those who presented with an existing clinical condition of pericoronitis, diabetes mellitus, a history of gastritis orgastrointestinal ulcers, high blood pressure, renal alterations or allergy to any of the drugs used in the study.
The patients were divided into 4 groups (G): G1 (n=10) which received 600 mg of ibuprofen together with 555mg of arginine, G2 (n=9) which received 90 mg of etoricoxib, G3 (n=10) which received 8 mg of dexamethasone and G4 which received a placebo (n=13), all of which were administered orally 90 minutes before surgery. The intensity of postoperative pain was evaluated using a numeric scale of 101 points (101P) and a separate 4-point verbal scale (VRS), at 2, 4, 6, 8, 12, 24, 36 and 48 hours after the procedure.
The drugs were removed from their original commercial packaging and were packed in similar packages, but called: A, B, C and D. After selecting the volunteers, they received an identification number. In order to preserve anonymity, a second researcher delivered the packs to the research study subjects and monitored the correct use of the medication.
A solution of mepivacaine 2% with epinephrine 1:100.000 (mean = 3.53; standard deviation = +2.47) was used for the local anesthetic. After extraction, all patients received 750 mg tablets of the pain reliever paracetamol, to be taken every 6 hours in the event of pain, and the patient was to mark on the record card the times that it was necessary to use them.
A pain-scale card (VRS and 101P) was handed out to the volunteers on the day of the surgery and this was returned at the next checkup for the removal of sutures and preservation. For the 4-point verbal scale, the patient was instructed to mark a number between 0 and 100 to indicate how intense the pain was at that moment, 0 signifying no pain and 100 equating to intolerable pain. On the verbal scale, the patient noted how he was feeling at that point in time (no pain, slight pain, moderate pain or severe pain). The data were processed statistically using the Kruskall-Wallis and Mann Whitney tests was set at 5% (p<0.05).
This study was approved by the Ethics in Research Committee at the State University of Ponta Grossa (Record no. 16272/09).
RESULTS
The data obtained using the 101 point scale (Figure 1) show that the volunteers in all the groups reported some intensity of pain, at all the points in time evaluated. Four hours after extraction, there was a statistically significant difference in relation to the placebo group (G4=60.3) when compared to the other groups (G1=13; G2=18.8; G3=35). In the six-hour period there was a statistically significant difference between G2 (13.3) and G3 (36.5) and between G1 (8.0) and G3 (36.5). As far as the period of 12 hours was concerned, there was a statistically significant difference between G4 (24.2) and G2(3.3) and between G4 (24.2) and G1(9.2).
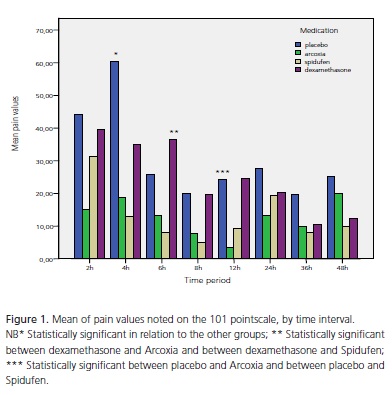
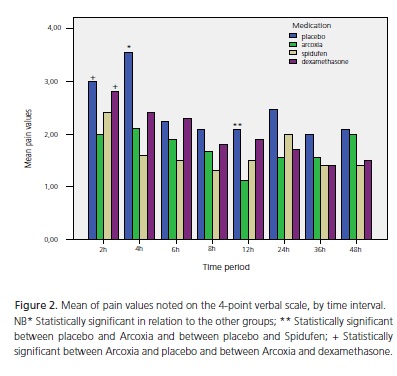
Figure 2 shows the mean value of the volunteers' pain when the 4-point verbal scale was used. Two hours after extraction, there was found to be a statistically significant difference between G2 (2.0) and G4 (3.0) and between G2 (2.0) and G3 (2.8). At 4 hours there was a statistically significant difference between G4 (3.5) in relation to the other groups (G1=1.6; G2=2.1; G3=2.4). At12 hours, a statistically significant difference was found between G4 (2.0) and G2(1.1) and between G4 (2.0) and G1(1.5).
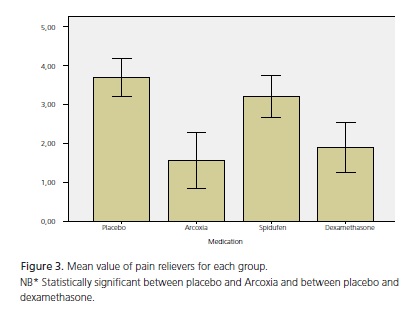
In Figure 3, the mean value of the pain relievers can be seen for each group, in which a statistically significant difference was observed between G4 (3.7) and G2(1.5) and between G4 (3.7) and G3(1.9).
DISCUSSION
The anti-inflammatory drug etoricoxib (Arcoxia) is a COX-2 selective inhibitor which is effective in the treatment of pain, having a fast response and a prolonged effect. It has already been demonstrated that the dose which provides maximum efficiency in controlling postoperative pain in oral surgery is 120mg10.
Ibuprofen with arginine is more effective as an analgesic when compared to ibuprofen by itself5. For this reason, and because ibuprofen is considered to be a safe drug, which serves as the gold standard when comparing with other anti-inflammatory drugs, including the COX-2 selective inhibitors5, it was decided, in the present study, to use ibuprofen combined with arginine.
Researchers have noted that the COX-2 selective inhibitors were clearly better than Ibuprofen, and in singledose situations, COX-2 selective inhibitors demonstrated a longer period of analgesic action when compared to ibuprofen12.
It should be stressed that none of the studies1-2,5-6,8-12 compared etoricoxib with ibuprofen. As etoricoxib does not alter bleeding time, it has the big advantage of being administered in just one daily dose and not causing gastrointestinal alterations, apart from the fact that it still has not been widely studied.
As for the present study, no statistical difference was found when comparing treatments with etoricoxib or ibuprofen. Therefore, these drugs had similar patterns in terms of the promotion of preemptive analgesia. So our results agree to another study19 conducted in 2011 where they compared etoricoxib, 90 mg and 120mg, with ibuprofen 600 mg; these authors concluded that there was no difference between these 3 groups, and that all are effective in controlling pain after the extraction of impacted third molars.
Many studies have already shown that preemptive analgesia with a placebo is lower than that observed when compared to anti-inflammatory drugs in controlling pain after extraction of mandibular third molars1,3,5,6,8,20. These studies are consistent with the results of the present study where the placebo also obtained results lower than the other protocols applied, with both scales and at the different points in time post-surgery.
Researchers concluded that the use of (two 6mg) doses of dexamethasone reduces post-surgical pain, spasm and edema in the third molars20. Other authors concluded that there was no statistically significant difference between a single 8mg dose of intramuscular dexamethasone and a single oral dose of 8mg dexamethasone21. In a another study22 conducted using similar methodology, there was found to be no difference between the groups that used different routes of administration (oral and intramuscular) for dexamethasone 8mg. It should be stressed that dexamethasone is a low-cost drug, thereby facilitating its use in the various social strata and has the advantage of having only a small mineral ocorticoid effect12.
Taking into consideration the abovementioned studies, the present study used dexamethasone orally due to ease of administration and to it being readily accepted by the patients. However, at 6 hours following extraction, using the 101 point numerical scale, the groups etoricoxib and ibuprofen combined with arginine had better pain control than the dexamethasone group. Two hours after extraction, when using the 4-pointverbalscale, it was found that etoricoxib presented better results than dexamethasone and the placebo. These results diverge from those obtained in another study11 where the researchers found no statistical differences between the group that was medicated with etoricoxib and the dexamethasone group.
Some authors20 have shown a reduced postoperative use of analgesics in patients who made preoperative use of dexamethasone in third molar surgery, when compared to the placebo. The present study confirms this study, since a statistically significant difference was found between G4 and G2 and between G4 and G3 with the consumption of pain relievers. Another study showed that patients subjected to the extraction of third molars who used dexamethasone co-administered with ibuprofen, used less pain relieving medication in comparison with individuals who used ibuprofen by itself or a placebo23.
The use of ibuprofen in preemptive analgesia was compared to the use of the same medication as a preventive analgesia. The results showed that there was no statistical difference between the two methods of administration of ibuprofen in controlling pain and edema after the extraction of mandibular thirdmolars24.
CONCLUSION
It may be concluded that the anti-inflammatory drugs tested promote greater analgesia in the first four hours after surgery, compared to the placebo, and the consumption of analgesics (pain relievers) is lower when using etoricoxib or dexamethasone.
Collaborators
AH LISBOA took part in the development of the study protocol, performed the collection and analysis of data, helped with the interpretation of results and the composition of the article. GL PILATTI took part in the development of the study protocol, conducted the statistical part of the study, helped with the interpretation of the results and the composition of the article.
REFERENCES
1. Klongnoi B, Kaewpradub P, Boonsiriseth K, Wongsirichat N. Effect of single dose intramuscular injection dexamethasone on preoperative lower impacted third molar surgery. Int J Oral Maxillofac Surg. 2012;41(3):376-9. doi: 10.1016/j. ijom.2011.12.014. [ Links ]
2. Girotto MA. Estudo comparativo de dois protocolos farmacológicos em exodontias de terceiros molares mandibulares inclusos [tese]. Piracicaba: Universidade Estadual de Campinas; 2003.
3. Moore RA, Straube S, Paine J, Derry S, McquayHJ. Minimum efficacy criteria for comparisons between treatments using individual patient meta-analysis of acute pain trials: examples of etoricoxib, paracetamol, ibuprofen, and ibuprofen/paracetamol combinations after third molar extraction. Pain. 2011;152(5):982- 89. doi: 10.1016/j.pain.2010.11.030.
4. Dionne R. Preemptive vs preventive analgesia: which approach improves clinical outcomes?. Compend Contin Educ Dent. 2000;21(1):48-56.
5. Black P, Max MB, Desjardins P, Norwood T, Ardia A, Pallotta T. A randomized, double-blind, placebo-controlled comparision of the analgesic efficacy, onset of action, and tolerability of Ibuprofen arginate and Ibuprofen in postoperative dental pain. Clin Ther. 2002;24(7):1072-9.
6. Baxendale BR, Vater M, Lavery KM. Dexamethasone reduces pain and swelling following extraction of third molar teeth. Anaesthesia. 1993;48(11):961-4.
7. Bodnar J. Corticosteroids and oral surgery. Anesth Prog. 2001;48(4):130-2.
8. Moore PA, Brar P, Smiga ER, Costello BJ. Preemptive rofecoxib and dexamethasone for prevention of pain and trismus following third molar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(2):1-7.
9. Kim K, Brar P, Jakubowski J. The use of corticosteroids and nonsteroidal xodontias matory medication for the management of pain and inflammation after third molar surgery: a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:630-40.
10. Malmstrom K, Sapre A, Couglin H, AgrawalNGB, Mazenko RS, Fricke JR. Etoricoxib in acute pain associated with dental surgery: a randomized, double-blind, placebo- and active comparatorcontrolled dose-ranging study. Clin Ther. 2004;26(5):667-79. doi: 10.1016/S0149-2918(04)90067-7.
11. Sotto-Maior BS, Senna PM, Assis NMSP. Corticosteroids or cyclooxygenase 2-selective inhibitor medication for the management of pain and swelling after third-molar surgery. J Craniofac Surg. 2011;22(5):758-62. doi: 10.1097/ SCS.0b013e318207f3fe.
12. Huber MA, Terezhalmy GT. The use of COX-2 inhibitors for acute dental pain: a second look. J Am Dent Assoc. 2006;137(4):480- 7.
13. Pilatti GL, Santos FA, Bianchi A, Cavassim R, Tozetto CW. The use of celecoxib and dexamethasone for the prevention and control of postoperative pain after periodontal surgery. J Periodontol. 2006;77(11):1809-14.
14. Alexander RE, Throndson RR. A review of preoperative corticosteroid use in dentoalveolar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(4):4-15. doi: 10.1067/ moe.2000.109778.
15. Fornasini G, Monti N, Brogin G, Gallina M, Eandi M, Persiani S, et al. Preliminary pharmacokinetic study of ibuprofen enantiomers after administration of a new oral formulation (ibuprofen arginine) to healthy male volunteers. Chirality. 1997;9(3):297- 302. doi: 10.1002/(SICI)1520-636X(1997)9:3<297::AIDCHIR16> 3.0.CO;2-I.
16. Ostenfeld T, Price J, Albanese M, Bullman J, Guillard F, Meyer I, et al. A Randomized, controlled study to investigate the analgesic efficacy of single doses of the cannabinoid receptor-2 agonist GW842166, ibuprofen or placebo in patients with acute pain following third molar tooth extraction. Clin J Pain. 2011;17(8):668-76. doi: 10.1097/AJP.0b013e318219799a.
17. Pell GJ, Gregory GT. Impacted third molars: classification and modified technique for removal. Dent Digest. 1933;39:330-8.
18. Winter GB. Principles of exodontias as applied to the impacted mandibular third molar; a complete treatise on the operative technic with clinical diagnoses and radiographic interpretations. St. Louis: American Medical Book Co.; 1926.
19. Daniels SE, Bandy DP, Christensen SE, Boice J, Losada MC, Liu H, et al. Evaluation of the dose range of etoricoxib in an acute pain setting using the postoperative dental pain model. Clin J Pain. 2011;27(1):1-8. doi: 10.1097/AJP.0b013e3181ed0639.
20 Schmelzeisen R, Frölich JC. Prevention of postoperative swelling and pain by dexamethasone after operative removal of impacted third molar teeth. Eur J Clin Pharmacol. 1993;44(3):275-7.
21. Boonsiriseth K, Klongnoi B, Sirintawat N, Saengsirinavin C, Wongsirichat N. Comparative study of the effect of dexamethasone injection and consumption in lower third molar surgery. Int J Oral Maxillofac Surg. 2011;41(2):244-7. doi: 10.1016/j.ijom.2011.12.011.
22. Antunes AA, Avelar RL, Martins Neto EC, Frota R, Dias E. Effect of two routes of administration of dexamethasone on pain, edema, and trismus in impacted lower third molar surgery. Oral Maxillofac Surg. 2011;15(4):217-23. doi: 10.1007/s10006-011- 0290-9.
23. Bauer HC, Duarte FL, Horliana AC, Tortamano IP, Perez FE, Simone JL, et al. Assessment of preemptive analgesia with ibuprofen coadministered or not with dexamethasone in third molar surgery: a randomized double-blind controlled clinical trial. Oral Maxillofac Surg. 2012;17(3):165-71. doi: 10.1007/ s10006-012-0360-7.
24. Aznar-Arasa L, Harutunian K, Figueiredo R, Valmaseda- Castello'n E, Gay-Escoda C. Effect of preoperative ibuprofen on pain and swelling after lower third molar removal: a randomized controlled trial. Int J Oral Maxillofac Surg. 41(8):1005-9. doi: 10.1016/j.ijom.2011.12.028.
 Endereço para correspondência:
Endereço para correspondência:
FRF ALVES
e-mail: alessandrolisboa@hotmail.com
Received on: 17/2/2012
Final version resubmitted on: 23/1/2013
Approved on: 25/4/2013
