










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.3 Porto Alegre Jul./Set. 2013
Multidisciplinary treatment of adult patients with Class III malocclusion
Tratamento multidisciplinar de paciente adulto com má oclusão de Classe III
Carla Corrêa MENDES-GOUVÊAI; Nicolas Zaragoza VELAZQUEZII; Alessandro SCHWERTNERIII; Eduardo César Almada SANTOSII
I Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia, Departamento de Odontologia Infantil e Social. Rua José Bonifácio, 1193, Vila Mendonça, 16015-050, Araçatuba, SP, Brasil.
II Universidade Estadual Paulista Júlio de Mesquita Filho, Faculdade de Odontologia, Departamento de Odontologia Infantil e Social. Araçatuba, SP, Brasil.
III Universidade do Norte do Paraná. Londrina, PR, Brasil.
ABSTRACT
This article describes the multidisciplinary treatment of an adult patient presenting with Angle Class III malocclusion, alteration of the mandibular position, vertical alveolar bone loss and absence of teeth in the lower posterior region. With advancing age the existence of occlusal interference due to loss of teeth or tooth structure is very common, resulting in periodontal problems due to occlusal trauma. The options for treatment of Class III malocclusion in adolescent and adult patients include compensatory orthodontic treatment in mild to moderate cases and orthognathic surgery for moderate to severe cases. The combination of various dental specialties enabled improvement in the social circumstances of the patient. This can be observed objectively by the final dental relationship and by the skeletal and tegumentary cephalometric comparison between the situation at the beginning and at the end of the treatment. The compensatory treatment performed permitted the successful correction of a Class III malocclusion in the clinical case presented.
Indexing terms: Malocclusion, Angle Class III. Orthodontics. Patient care planning. Therapy.
RESUMO
Este trabalho descreve o tratamento multidisciplinar de um paciente adulto com má oclusão de Classe III de Angle, alteração postural da mandíbula, perda óssea alveolar vertical e ausência dentária na região póstero-inferior. Com o avanço da idade é muito comum a existência de interferências oclusais devido à perda de dentes ou de estrutura dentária, resultando em problemas periodontais devidos ao trauma oclusal. As opções de tratamento da má oclusão de Classe III em adolescentes e pacientes adultos incluem tratamento ortodôntico compensatórios em casos suaves a moderados e cirurgia ortognática para casos moderados a severos. O resultado clínico da interação de diferentes especialidades odontológicas permitiu uma melhora do aspecto social da paciente, objetivamente pela relação dentária final e pela comparação cefalométrica esquelética e tegumentar entre o início e final de tratamento. O tratamento compensatório realizado possibilitou o sucesso na correção de uma má oclusão de Classe III do caso clínico apresentado.
Termos de indexação: Má oclusão de Angle Classe III. Ortodontia. Planejamento de assistência ao paciente. Terapia.
INTRODUCTION
The demands of adult patients in Orthodontic clinics are getting heavier and heavier due to the public's growing awareness of the esthetic and functional benefits1 of orthodontic treatment and the need for repeat treatment for malocclusions. With advancing age it is very common to find occlusal interference due to the loss of teeth or dental structure, resulting in periodontal problems on account of occlusal trauma2. Late intervention in the permanent dentition, albeit limited, is viable when a more posterior positioning of the lower jaw is prioritized with a subsequent increase in lower anterior facial height3.
Class III malocclusion in the adult population, for the most part, requires a multidisciplinary approach and the preparation of a conscious treatment plan that includes periodontal, prosthetic and endodontic therapy. Depending on the severity of the dysplasia of the upper and lower jaws, there may be a need for orthognathic surgery4-6. In the recent literature, there have been few articles that have included the longitudinal monitoring of a significantly large enough sample through to skeletal maturation, nevertheless it is worth performing a critique of what the authors consider to be longitudinal results.
The treatment options for adolescents and adult patients, however, include compensatory orthodontic treatment in mild to moderate cases and orthognathic surgery for moderate to severe cases7. It is preferable to perform compensations in patients whose craniofacial growth is complete, as growth changes are not necessarily predictable.
The aims of any orthodontic treatment are to eliminate the patient's complaint and establish physiological occlusion in areas where a pathological condition is causing damage to the periodontium or the teeth8. For patients with prosthetic and periodontal involvement, not submitted to orthognathic surgery, the aims of treatment should include the following: parallelism of the abutment teeth; redirecting the occlusal forces; adequate inter-proximal space and appropriate tooth positioning; improvement in the support and competence of the lip; improvement in the crown-to-root ratio; improvement in or correction of mucogingival and bone conditions; restoration and maintenance of periodontal health; functional and esthetic improvement to achieve the aims of orthodontic treatment6. In contrast to orthodontic therapy for adolescents, with adults it is generally the precursor of continuous treatment in order to facilitate prosthetic, surgical, restorative or periodontal therapy9. For this reason, the planning should be performed jointly with all the specialists involved6,10-11 and the treatment should follow the pre-established protocol10.
When treating adults, the patient's physiology must be respected, permitting functional conditions that maintain the integrity of the occlusion and the periodontal tissues, in ideal conditions and for a long time9. To this end, periodontal treatment should be carried out prior to the orthodontic treatment and the health of the periodontium should be controlled throughout the entire period of therapy9,12.
The following case illustrates the multidisciplinary treatment of an adult patient, encompassing periodontics, prosthesis, orthodontics and implantology.
CASE REPORT
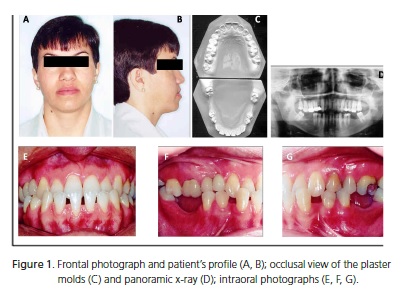
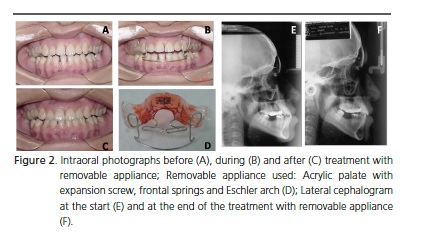
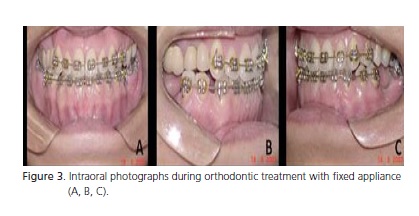
An adult Caucasian patient, aged 32, with Class III malocclusion, anterior crossbite, bone loss with anterior gingival recession of the lower jaw, counterclockwise rotation of the lower jaw and absence of lower posterior teeth. The patient was offered a treatment which combined orthodontic-surgical treatment and prosthetic rehabilitation. This option was spontaneously rejected by the patient as he did not wish to be subjected to orthognathic surgery. After the diagnosis and the confirmation of the involvement of the postural mandibular component, pronounced inclination of the lower incisors and diastemas, a second treatment plan was proposed in which he would initially undergo periodontal treatment and monitoring of the state of the periodontium during the orthodontic therapy (Figure 1). Then he would be treated with a removable appliance (Acrylic palate with expansion screw, frontal springs and Eschler arch, used daily for 10 months) to improve mandibular posture and to upright the lower incisors (Figure 2). Afterwards the complete orthodontic treatment was carried out for alignment/leveling and the recovery of the prosthetic spaces (Figure 3). The last step consisted of the prosthetic rehabilitation of any spaces to restore complete function (Figure 4).
It should be stressed that, prior to treatment, the patient in question signed a free and informed consent form, authorizing the publication of the case.

DISCUSSION
The interaction of the dental specialties, with the wider range of treatment prognosis, leads to a satisfactory situation, both in terms of the patient's occlusion at the conclusion of the treatment (Figure 4), and esthetically, promoting a consequent improvement in the patient's social circumstances. The results obtained permit us to assert the importance of multidisciplinary treatment in the adequate restoration of the inter-arch relationship, function and esthetics.
In the clinical case in question, the option for treatment using orthognathic surgery for the Class III skeletal correction was rejected by the patient. The second option offered, which was acceptable to the patient, was treatment with dentoalveolar compensation, which was clinically possible to perform, however the underlying skeletal deformity would persist. It should be stressed that dental compensation can be effective in the treatment of borderline cases13, carried out either with or without the extraction of teeth14.
The planning of the compensation of dental positioning, to permit functional occlusion on badly positioned bone bases15, was carried out satisfactorily. The patient was aware that the surgical approach could provide an even better occlusal and esthetic outcome16.
Nevertheless, with regard to patient satisfaction with the results of treatment and the resolution of his initial complaints15, the treatment that was performed addressed these aspects successfully.
Although the literature contains articles about Class III compensatory treatment on adult patients14-15,17, it is important right now to show cases where there has been multidisciplinary treatment and emphasize that the wishes and desires of the patient must be prioritized. Accordingly, one factor in considering treatment a success consists of patient satisfaction with the results achieved.
CONCLUSION
At the present time, mainly with adult patients, the integration and planning of the treatment of malocclusions permits us to attain feasible objectives and eliminate the patient's main complaint. In the presented case of the patient with Class III malocclusion, the multidisciplinary treatment resulted in sufficiently satisfactory and adequate esthetics, repeating that the success of the results obtained also entails the patient´s satisfaction with the outcome.
Collaborators
A SCHWERTNER performed the patient's orthodontic treatment and the initial composition of the article. CC MENDES-GOUVÊA and NZ VELAZQUEZ conducted a review of the literature, organization and final composition of the article. ECA SANTOS directed the research and took part in the composition of the article.
REFERENCES
1. Khan RS, Horrocks EN. A study of adult orthodontic patients and their treatment. Br J Orthod. 1991;18(3):183-94. [ Links ]
2. Nattrass C, Sandy JR. Adult orthodontics: a review. Br J Orthod. 1995;22(4):331-7.
3. Fränkel R, Fränkel CH. Ortopedia orofacial com regulador de função. São Paulo: Editora Santos; 1990.
4. Carastro J, Moshiri F. Adult orthodontics: an update. Am J Orthod Dentofacial Orthop. 1987;91(1):81-2.
5. Lindauer SJ, Rebellato J. Biomechanical considerations for orthodontic treatment of adults. Dent Clin North Am.1996;40(4):811-36.
6. Shroff B, Siegel SM, Feldman S, Siegel SC. Combined orthodontic and prosthetic therapy. Dent Clin North Am. 1996;40(4):911- 43.
7. Yavuz I, Hahcioglu K, Ceylan I. Face mask therapy effects in two skeletal maturation groups of female subjects with skeletal class iii malocclusions. Angle Orthod. 2009;79(5):842-8. doi: 10.2319/090308-462.1.
8. Capelozza Filho L, Braga AS, Cavassan AO, Ozawa TO. Tratamento ortodôntico em adultos: uma abordagem direcionada. Rev Dental Press Ortod Ortop Facial. 2001;6(5):63- 80.
8. Capelozza Filho L, Braga AS, Cavassan AO, Ozawa TO. Tratamento ortodôntico em adultos: uma abordagem direcionada. Rev Dental Press Ortod Ortop Facial. 2001;6(5):63- 80.
9. Petrelli E. Ortodontia contemporânea. São Paulo: Editora Sarvier; 1993.
10. Almeida RR, Bonfante G, Iague Neto G, Almeida MR. A interrelação Ortodontia e Prótese: apresentação de um caso clínico. Rev Dental Press Ortod Ortop Facial. 1997;2(4):13-20.
11. Penido SMMO, Sakima T, Gandini Júnior LG, Dinelli TCS. A interrelação da ortodontia e outras especialidades odontológicas: relato de caso clínico. Rev Ass Paul Especial Ortod Ortop Facial. 2003;1(2):63-74.
12. Koroluk LD, Konchak PA. Adjunctive orthodontic treatment for adult patients. J Can Dent Assoc. 1996;62(5):423-7.
16. Koroluk LD, Konchak PA. Adjunctive orthodontic treatment for adult patients. J Can Dent Assoc. 1996;62(5):423-7.
17. Koroluk LD, Konchak PA. Adjunctive orthodontic treatment for adult patients. J Can Dent Assoc. 1996;62(5):423-7.
13. Ferro A, Nucci LP, Ferro F, Gallo C. Long-term stability of skeletal Class III patients treated with splints, Class III elastics, and chincup. Am J Orthod Dentofacial Orthop. 2003;123(4):423-34. doi: 10.1067/mod.2003.70.
14. Lima CE, Lima MT. Directional force treatment for an adult with Class III malocclusion and open bite. Am J Orthod Dentofacial Orthop. 2006;129(6):817-24.
15. Souza RLS, Rocha EAM, Ribeiro AA, Caldas SGFR. Diagnóstico e tratamento de má oclusão de Classe III com mordida dupla em paciente adulto: relato de caso. Rev Clin Ortodon Dental Press. 2008;7(5):84-92.
16. Dwyer P. Orthodontic and orthognathic surgical correction of a severe Class III malocclusion. Am J Orthod Dentofacial Orthop. 1998;113(2):125-32.
17. Janson G, Souza JEP, Alves FA, Andrade JR P, Nakamura A, Freitas MR, et al. Extreme dentoalveolar compensation in the treatment of Class III malocclusion. Am J Orthod Dentofacial Orthop. 2005;128(6):787-94.
 Endereço para correspondência:
Endereço para correspondência:
CC MENDES-GOUVÊA
e-mail: carla_cmendes@ hotmail.com
Received on: 28/6/2010
Final version resubmitted on: 10/1/2011
Approved on: 27/1/2011
