










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.4 Porto Alegre Out./Dez. 2013
ORIGINAL / ORIGINAL
Analysis of the preparation obtained by three techniques of root canal instrumentation using computed tomography
Análise do preparo obtido por três técnicas de instrumentação do canal radicular através de tomografia computadorizada
Susy Cristina Gouvêa AMADEUI; Rodrigo Sanches CUNHAII; Carlos Eduardo da Silveira BUENOI; Flávia Casale ABEI; Alexandre Sigrist de MARTINI
I Faculdade São Leopoldo Mandic, Curso de Odontologia, Departamento de Endodontia. Rua José Rocha Junqueira, 13, Swift, 13045-755, Campinas, SP, Brasil.
II University of Manitoba, Department of Endodontics. Winnipeg, Canada.
ABSTRACT
Objective
Use computed tomography to compare three methods of root canal instrumentation.
Methods
Thirty mandibular molar mesiobuccal canals were divided in three groups according to instrumentation technique: Group 1 - hand instrumentation with balanced force technique; Group 2 - Protaper Universal rotary system following manufacturer's instructions; and Group 3 - Protaper Universal rotary system and Gates-Glidden drills. Teeth were evaluated by computed tomography before and after preparation at three axial cuts: 3mm, 5mm, and 7mm from the root apex. Data were subjected to statistical analysis using the F, Chi-Square, Likelihood Ratio Chi-Square, and Mantel-Haenszel Chi-Square tests.
Results
Group 3 showed significantly greater dentin removal with no tendency towards mesial or distal canal transportation, compared with Groups 1 and 2. Also, Group 3 required the least amount of time for instrumentation.
Conclusion
Association of rotary instrumentation and Gates-Glidden drills is a safe and effective technique for root canal preparation.
Indexing terms: Dental instruments. Dental pulp cavity. Endodontics. Tomography, X-Ray Computed.
RESUMO
Objetivo
Comparar o preparo de canais radiculares através de tomografia computadorizada.
Métodos
Trinta canais mésio-vestibulares de molares inferiores foram divididos em 3 grupos, de acordo com a técnica de instrumentação a ser utilizada: Grupo 1 - instrumentação manual, utilizando-se de movimentos de forças balanceadas; Grupo 2 - Sistema Protaper Universal de instrumentação rotatória, conforme protocolo do fabricante; Grupo 3 - Sistema Protaper Universal de instrumentação rotatória associada a brocas de Gates- Glidden para pré-alargamento cervical. Os dentes foram submetidos à tomografia computadorizada antes e após o preparo, e a análise das imagens foi feita através de cortes axiais a 3mm, 5mm e 7mm do ápice radicular. Os dados foram submetidos a análise estatística utilizando testes paramétricos (para as variáveis tempo e desgaste de dentina) e não-paramétricos (para a variável sentido do desvio).
Resultados
Os resultados mostraram uma tendência significativa do grupo 3 a desgastar mais dentina quando comparado aos grupos 1 e 2. O grupo 1 desgastou significantemente mais dentina para o sentido distal e o grupo 2 desgastou significantemente mais para o sentido mesial. O grupo 3 não apresentou tendência de sentido de desgaste. O tempo despendido foi menor no grupo 3, seguido pelo grupo 1 e 2.
Conclusão
Pôde-se concluir que a associação das brocas de Gates-Glidden ao Sistema Protaper Universal promoveu um preparo adequado de maneira segura e, a tomografia computadorizada foi um método adequado para a análise do preparo de canais radiculares.
Termos de indexação: Instrumentos odontológicos. Cavidade pulpar. Endodontia. Tomografia Computadorizada por Raios X.
INTRODUCTION
There are a large number of rotary instrumentation systems available for endodontic practice, and there are great differences in design and clinical performance among them. The advantages these systems have brought endodontists deserve to be pointed out, however, many advancements in instrument design have been made to improve canal shaping and diminish clinical time. An example of this is the Protaper System (Dentsply Maillefer, Ballaigues, Switzerland) that was produced with progressive tapers with the intention of creating an ideal formatting in the shortest clinical time.
Cervical pre-widening with the use of Gates- Glidden burs in decreasing sizes releases interferences in the cervical and middle thirds of the root canal and allows the files to reach the apical third more easily and safely1-4 in addition to reducing the rate of Protaper instrument fractures.
The complex dental internal anatomy sometimes makes it difficult to elaborate an appropriate cylindricalconical modeling, demonstrates its limitations, and leaves areas without undergoing the action of instruments, and others with excessive dentinal wear. Taking into consideration that the majority of canals have a flattened anatomic shape, no matter how thin or small the rotary instrument diameter may be, its action on these flattened areas is unlikely to occur, preventing them from being well cleaned and shaped3-6.
The literature has shown that the qualitative analysis of root canal instrumentation has been performed by some methodologies in canals simulated in resin blocks and in natural teeth. Analysis in natural teeth has been performed by means of radiographic assessments, system of muffles, moldings or by tomography. Compute tomography was recently suggested for this type of analysis, with good results, mainly because of being a nondestructive resource that allows evaluation of the quantity of dentin removed from the root canal walls5,7.
The aim of this study was to evaluate, by means of computed tomography, the direction of the root canal deviation, quantity of dentin removed in the mesiovestibular canal of mesial roots of mandibular molars after the use of three instrumentation techniques and the total time spent on each technique.
METHODS
Thirty extracted first or second permanent mandibular molars were selected for this study. The teeth had completely formed roots, were stored in physiological solution and the mesio-vestibular roots presented curvatures between 25 and 45 degrees. The use of the teeth for research purposes was approved by the Research Ethics Committee of São Leopoldo Mandic, under Protocol No.06/025.
After coronal opening, the mesial roots were separate from the distal roots at the furca level, using a diamond-coated disc (KG Sorensen, Brazil). Part of the tooth crowns was cut in order to standardize the working length to 19 mm. The roots were randomly divided into 3 equal groups, with the aim of providing the homogeneity of the samples. The roots were then positioned and fixed by the cervical portion in an acrylic resin base, five at a time, at all times with the vestibular surface, which was marked with a scratch, facing the external surface of the tomograph.
In order to obtain the pre-instrumentation images, in three cuts for analysis: 3, 5 and 7 mm from the root apex, the tomograph, 3DX Accuitomo (J. Morita®, Japan) was used.
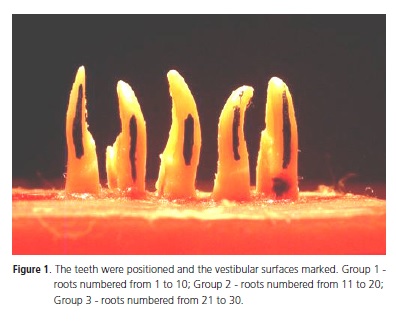
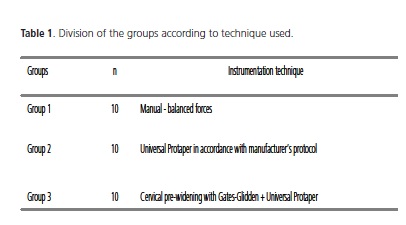
For each of the groups, a technical sequence of root canal preparation was formed, as shown in Table 1.
Detailed description of the techniques used considering the groups:
Group 1: Roots 1 to 10 - two-stage manual instrumentation technique using the Balanced Forces concept
Instrumentation performed by this technique was divided into two stages: Preparation of the cervical and middle thirds, and apical preparation.
Preparation of the cervical and middle thirds: a) initial catheterization with Kerr type file #10 up to the real working length (RWL); b) widening of the cervical and middle thirds (up to the beginning of the curvature) with K-flexofile type files using balanced force movements up to the diameter corresponding to KFlexofile type file #35; c) using Gates Glidden #3 and #2 burs, respectively with "brush-stroke" movements in the direction towards the "safety zone".
Preparation of the apical third: a) preparation of the apical third up to the diameter corresponding to file K-flexofile #25; b) step-back with programmed withdrawal of 1 mm at a time, up to the diameter corresponding to file K-flexofile #40.
Group 2: Roots 11 to 20 - Rotary instrumentation with Universal Protaper System - technique suggested by the manufacturer.
To perform the preparation of teeth in the Groups with the Universal Protaper rotary system, an X-Smart electric motor (Denstply-Maillefer) with a constant speed of 300 rpm and torque control suggested by the manufacturer was used in the following manner: a) Shaping files (Sx, S1 and S2) - torque 3Ncm; b) Finishing files (F1, F2) - torque 1Ncm and 2Ncm respectively.
Sequence used: a) initial catheterization with K-file #10 up to RWL;
b) the use of file S1, until small resistance was offered; c) file Sx, until small resistance was offered; d) file S1,up to RWL; e) file S2, up to RWL; f) file F1, up to RWL; g) file F2, up to RWL.
For each tooth a new rotary instrument was used.
Group 3 - Roots 21 to 30 - Rotary instrumentation with Universal Protaper System with pre-widening using Gates Glidden burs. a) initial catheterization with Kerr type file #10 and #15, up to RWL; b) use of file S1, until small resistance was offered; c) file Sx, until small resistance was offered; d) Gates-Glidden bur #3 at low speed, (10.000 rpm); e) Gates Glidden bur #2 at low speed, (10.000 rpm); f) pre-widening with K-flexofile type file # 15 and 20 up to RWL; g) file S1, if possible, up to RWL; h) file S2, if possible, up to RWL; i) file F1, up to RWL; j) pre-widening with K-flexofile type file #25; k) file F2, up to RWL.
In the same way as in Group 2, the manual files and Gates-Glidden burs were used twice and for each tooth a new rotary file was used.
For all the groups the same irrigation protocol was used; that is to say, 5ml of 2.5% sodium hypochlorite at each change of file, 5ml of 17% EDTA (ethylenodiamino tetraacetic acid) for 3 minutes and final irrigation with 2 ml of 2.5% sodium hypochlorite. For maintenance of foraminal patency a Kerr type file #10 was used at each change of file. The manual and rotary files, and Gates- Glidden burs were used only once. A new tomograph was taken after instrumentation, and cuts were made at 3, 5 and 7mm from the root apex.
To measure the areas of the canals, the software program ImageTool (ImageTool Software Development Kit Source Code Version 3.0) was used, and the area corresponding to the root canal before and after instrumentation was demarcated for 3, 5 and 7 mm. This procedure was performed by two evaluators at different times, to provide greater reliability of the measures, and a mean was calculated. Afterwards, the means of the measurements obtained of the area of each root post-instrumentation were subtracted from the preinstrumentation area, thus calculating the area of dentin removed.
For measurement of the direction of deviation, the differences in measurements between pre-and postinstrumentation were analyzed in a similar manner to that suggested by Gambill et al.6, however, the sign of that difference was not removed, because a negative difference would mean a deviation in the Distal (D) direction; a positive difference, deviation in the Mesial (M) direction and a null difference, centralized canal (C). The measurements were made with the aid of the program 3D Tomox (version 1.0.51), associated with the tomograph itself, which allowed the measurements to be calculated in millimeters, make cuts in the direction of X, Y and Z and visualize images in three dimensions. The time spent on the preparation of each root was calculated (in minutes).
To evaluate the time spent a stopwatch (Cronobio. CIAL, São Paulo, Brazil) was used.
The data were submitted to statistical analysis by means of parametric tests, such as the F test for the analysis of variance of the variables time and dentin wear, and non parametric tests, such as the Chi-Square, Likelihood Ratio Chi-Square and Mantel-Haenszel Chi-Square tests for the variable direction of deviation.
RESULTS
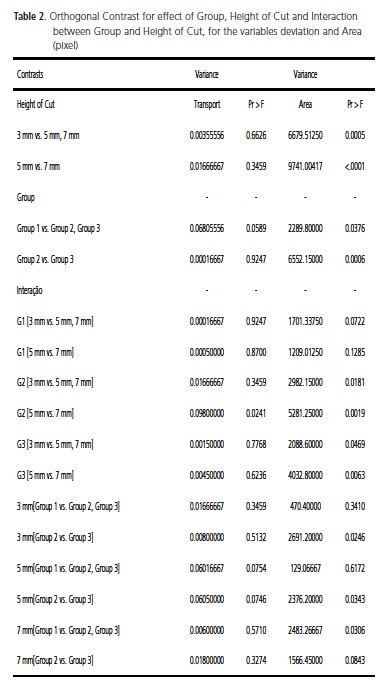
For the variable area there was statistical difference among the three groups, with the largest quantity of dentin being removed in Group 3, followed by Group 2 and 1, respectively. Whereas with regard to height of cuts, the results showed that in Groups 2 and 3, the conicity of the canals was maintained to a greater extent, and in Group 1 there was greater rectification of the canal, and there was no statistical difference for area as regards the heights of cuts before and after preparation. Moreover, at the height of cut at 7 mm only Group 1 presented significant difference among the other groups, with a lower value for dentin removal.
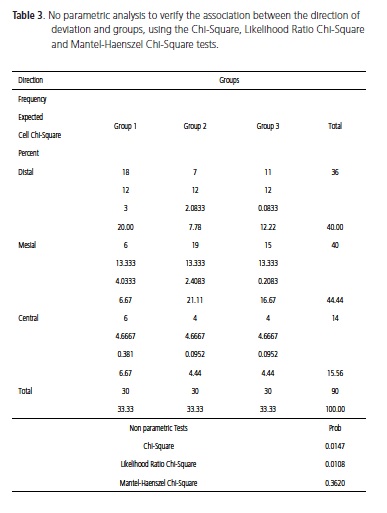
With the purpose of verifying the direction of deviation, categories were established for this variable according to the sign and magnitude observed, in the following manner: negative difference deviation in the Distal direction (D); positive difference deviation in the Mesial direction (M); and Null value observed, revealed the absence of deviation; that is to say, a centralized canal (C). This new variable was analyzed by non parametric statistics using the Chi-Square, Likelihood Ratio Chi-Square and Mantel-Haenszel Chi-Square tests.
For the association between groups (instrumentation procedures) and direction of deviation, a significant effect was observed, of Group 1 in deviating more towards the Distal direction, and Group 2, deviating more towards the Mesial direction. Group 3 presented no tendency between the different directions of deviation.
DISCUSSION
Various methodologies have been used to evaluate the action of instruments and techniques in root canal shaping, such as the radiographic method1,7-12, muffles13-15, artificial canals16-17 and computed tomography, which has been to be superior for this type of analysis4-6,18-25.
The mesio-vestibular roots of extracted mandibular molars were used, as they frequently present accentuated curvatures and accentuated concavity in the distal region, making them more susceptible to the risks of instrumentation21.
Taking into consideration that the majority of canals have a flattened anatomic shape, no matter how thin or small the rotary instrument diameter may be, its action on these flattened areas is unlikely to occur, preventing them from being well cleaned and shaped3-6. Thus, the hybridization of instruments may be an efficient combination both for practicality and for diminishing the time and weariness of the operator. Berutti et al.26 studied the influence of manual pre-widening and torque on the failure of the Protaper system, and concluded that prewidening is the main determinant facture in the reduction of failures in this system.
As regards dentin removal, Group 1 was the one in which the last removal was promoted, and even between the three levels of cut in this group, there was no statistical difference with reference to area. This may be explained by the low conicity of the manual instruments, which do not promote such a conical preparation as that provided by rotary instruments with increasing tapers. It was observed that although the pre-widening with Gates-Glidden burs had been performed, at the height of the cut at 7 mm, more dentin was not removed in this Group than in Group 2, instrumented only with the Protaper rotary system18. Probably the little conicity of these manual instruments, even in a crown-apex preparation, did not open sufficient space to enable the Gates-Glidden burs to work more freely and at greater depth, without being forced into the apical direction, as happened in Group 3. Results contrary to these were shown by Gluskin et al.5, Gambill et al.6 and Peru et al.20.
In the most apical cut (3 mm) there was statistical difference between Groups 2 and 3 with regard to dentin removal. In Group 3 the apical third was widened more than it was in the Group in which the Protaper system was used as recommended by the manufacturer, probably because the instrument may have come into greater contact with the apical region, free of interferences from the cervical and middle thirds. This allows us to say that the apical preparation with rotary instruments does not necessarily have a smaller diameter in comparison with manual preparations, and a hybrid technique would be a good solution to enable these instruments to work freely within the canal and promote a larger widening of the apical and middle thirds, because the same was also observed in the cut at 5 mm from the apex.
In the more cervical cat at 7 mm from the root apex, Group 1 differed statistically from the others. In Group 1 less removal of dentin was promoted at 7 mm followed by Group 2 and lastly, with the greatest wear, Group 3. These same results were found by Garip & Gunday18, and they contradict the report made by Gluskin et al.5.
There was no difference in the direction of deviation between the heights of cuts, but there was difference between the groups and direction of deviation. Group 1 had a greater tendency to transport towards the distal direction. This is due to the fact that the stainless steel files are rigid, and have difficulty in working in large curvatures, and thus tend to wear more towards the region inside the curvature, rectifying the canal. Group 2 had a greater tendency to transport towards the mesial direction. This is owing to the fact that the NiTi files have a tendency to return to the initial position because of their superelasiticity and in the curvature of mandibular molars, they wear more toward the mesial direction; that is to say, outside of the curvature.
Group 3 showed no tendency towards deviation, conserving the canal in a more centralized form, probably as a result of associating the use of Gates-Glidden burs.
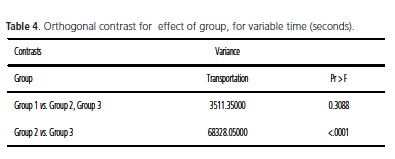
Group 3 was the one in which the preparation was performed in the fastest manner, followed by Group 1, without however, presenting statistical differences between them. Group 2 differed statistically from Group 3 as regards time, thus being the slowest group.
CONCLUSION
According to the methodology used, and based on the results obtained in the present study, it was possible to conclude that the Group in which there was the association of nickel-titanium rotary instruments with Gates-Glidden burs (pre-widening) the largest quantity of dentin removed and least deviation (transport) was promoted, and the procedure was the fastest.
Collaborators
SCG AMAEDEU was responsible for elaborating the project, conducting the research and writing the article. RS CUNHA was responsible for the statistical analysis, and writing the article. CES BUENO was responsible for preparing the samples, and writing the article. FC ABE was responsible for the bibliographic survey, and writing the article. AS MARTIN guided the research and participated in writing the article.
REFERENCES
1. Machado ME, Machado MLBBL, Antoniazzi JH. Eficácia da técnica seriada convencional e das técnicas escalonadas ápicocervical e cérvico-apical no preparo químico-cirúrgico de canais curvos. Rev Bras Odontol. 1998;55(2):55-62. [ Links ]
2. Roland DD, Andelin WE, Browning DF et al. The effect of preflaring on the rates of separation for 0.04 Taper nickel titanium rotary instruments. J Endod. 2002;28(7):543-5. doi: 10.1097/00004770-200207000-00015.
3. Peters OA, Schönenberger k, Laib A. Effects of four Ni–Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int Endod J. 2001;34(3):221-30. doi: 10.1046/j.1365-2591.2001.00373.x.
4. Paqué F, Balmer M, Attin T, Peters OA. Preparation of ovalshaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod. 2010;36(4):703-7. doi: 10.1016/j.joen.2009.12.020.
5. Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni–Ti rotary GT™ files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001;34(6):476-84. doi: 10.1046/j.1365- 2591.2001.00422.x.
6. Gambill JM, Alder M, Del Rio C. Comparison of nickel-titanium and stainless-steel hand-file instrumentation using computed tomography. J Endod. 1996;22(7):369-75. doi: 10.1016/S0099- 2399(96)80221-4.
7. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32(2):273-5. doi: 10.1016/0030-4220 (71) 90230-1.
8. Lee J. Canal orifice enlargement as related to biomechanical preparation. J Endod. 1983; 9(11): 463-70. doi: 10.1016/S0099- 2399(83)80160-5.
9. Heck AR, Garcia RB. Avaliação Radiográfica do Desvio Apical do Canal Radicular após a Instrumentação manual com Limas Flexofile, Flex-R e Onyx-R e o Sistema Mecânico Rotatório Profile. Rev Fac Odontol Bauru. 1999;7(1/2):35-40.
10. Schafer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: Protaper versus Race. Int Endod J. 2004;37(4):239-48. doi: 10.1111/j.0143-2885.2004.00783.x.
11. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38(10):743-52. doi: 10.1111/j.1365-2591.2005.01010.x.
12 Javaheri HH, Javaheri GH. A comparison of three Ni-Ti Rotary Instruments in Apical Transportation. J Endod. 2007;33(3):284- 6. doi: 10.1016/j.joen.2006.05.004.
13. Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod. 1987;13(5):243-5. doi: 10.1111/j.1365-2591.2005.01010.x.
14. Desplazes P, Peters O, Barbakow F. Comparing apical preparations of root canals shaped by nickel-titanium rotary instruments and nickel-titanium hand instruments. J Endod. 2001;27(3):196- 202. doi: 10.1097/00004770-200103000-00015.
15. Wu MK, van der Sluis WM, Wesselink PR. The risk of furcal perforation in mandibular molars using Gates-Glidden drills with anticurvature pressure. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99(3):378-82. doi: 10.1016/j. tripleo.2004.07.008.
16. Weine FS, Kelly RF, Lio PF. The effect of preparation procedures on original canal shape and on apical foramen shape. J Endod. 1975;1(8):255-62. doi: 10.1016/S0099-2399(75)80037-9.
17. Calberson FLG, Deroose CAJG, Hommez GMG et al. Shaping ability of GT rotary files in simulated resin root canals. Int Endod J. 2004;35(7):607-14. doi: 10.1046/j.1365-2591.2002.00540.x.
18. Garip Y, Günday M. The use of computed tomography when comparing nickel-titanium and stainless steel files during preparation of simulated canals. Int Endod J. 2001;34(6):476- 84.
19. Peters OA, Peters CI, Schönenberger K, Barbakow F. Protaper Rotary Root Canal Preparation: effects of canal anatomy on final shape analysed by micro CT. Int Endod J. 2003;36(2):86-92.
20. Peru M, Peru C, Mannocci F, Sherriff M, Buchanan LS, Pitt Ford TR. Hand and nickel-titanium root canal instrumentation performed by dental students: a micro-computed tomographic study. Eur J Dent Educ. 2006;10(1):52-9. doi: 10.1111/j.1600- 0579.2006.00395.x.
21. Taşdemir T, Aydemir H, Inan U, Unal O. Canal preparation with Hero 642 rotary Ni-Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J. 2005;38(6):402-8. doi: 10.1111/j.1365-2591.2005.00961.x.
22. Madarati AA, Qualtrough AJ, Watts DC. A Micro-computed tomography scanning study of root canal space:changes after ultrasonic removal of fractured files. J Endod. 2009; 35(1):125- 8. doi: .org/10.1016/j.joen.2008.10.005.
23. Paqué F, Peters OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molar with the self-adjusting file. J Endod. 2011;37(4):517-21. doi: 10.1016/j.joen.2010.12.011.
24. Paqué F, Ganahl D, Peters OA. Effects of root canal preparation on apical geometry assessed by micro-computed tomography. J Endod. 2009;35(7):1056-9. doi: 10.1016/j.joen.2009.04.020.
25. Yin X, Cheung GS, Zhang C, Masuda YM, Kimura Y, Matsumoto K. Micro-computed tomographic comparison of nickeltitanium rotary versus tradictional instruments in C-shaped root canal system. J Endod. 2010;36(4):708-12. doi: 10.1016/j. joen.2010.01.003.
26. Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of manual preflaring and torque on the failure rate of ProTaper rotary instruments. J Endod. 2004;30(4):228-30. doi: 10.1097/00004770-200404000-00011.
 Endereço para correspondência:
Endereço para correspondência:
AS MARTIN
e-mail: a-sigrist@uol.com.br
Received on: 6/12/2011
Final version resubmitted on: 20/6/2012
Approved on: 30/8/2012
