










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.4 Porto Alegre Out./Dez. 2013
ORIGINAL / ORIGINAL
Per capita cost of fluoridating the public water supply in a large municipality
Custo per capita da fluoretação da água de abastecimento público em um município de grande porte
Érica Helena Sgroi MARTINEZI; Antonio Carlos FRIASII; Haroldo José MENDESIII; Kelly Polido Kaneshiro OLYMPIOIV
I Serviço Autônomo de Água e Esgoto de Sorocaba. Av. Pereira da Silva, 1285, Jd. Santa Rosália, 18095-340 Sorocaba, SP, Brasil.
II Universidade de São Paulo, Faculdade de Odontologia, Departamento de Odontologia Social. São Paulo, SP, Brasil.
III Universidade Estadual do Sudoeste da Bahia, Departamento de Saúde, Colegiado de Odontologia. Jequié, BA, Brasil.
IV Universidade de São Paulo, Faculdade de Saúde Pública, Departamento de Saúde Ambiental. São Paulo, SP, Brasil.
ABSTRACT
Objective
To estimate the per capita cost of fluoridating the municipal water supply of Sorocaba in 2009 and describe the costs from 1989 to 2008.
Methods
Sorocaba's Autonomous Water and Wastewater Service disclosed the initial capital required for implementing the water fluoridation system and the costs associated with the purchase of chemicals, system operation, and control of fluoride concentration. These numbers were added and divided by the municipal population with piped water.
Results
In 2009 the per capita cost was R$ 1.43 (US$ 0.72), and from 1989 to 2008 the estimated per capita cost ranged from R$ 1.19 to R$ 1.43 (US$ 0.59 to 0.72).
Conclusion
The per capita cost of water fluoridation is low, and when the fluoride concentration is kept at the recommended levels, it is an efficient, simple, and safe public policy for preventing dental caries. Knowing its cost allows comparisons and encourages its implementation.
Indexing terms: Dental caries. Fluoridation. Water supply.
RESUMO
Objetivo
Estimar o custo per capita da fluoretação das águas de abastecimento público para o município de Sorocaba, em 2009 e descrever seus custos financeiros de 1989 a 2008.
Métodos
Foi realizada uma pesquisa junto ao Serviço Autônomo de Água e Esgoto de Sorocaba e os dados sobre custos do capital inicial de instalação, do produto químico, da operacionalização do sistema e do controle dos teores de fluoreto foram obtidos, calculados e divididos pelo número de habitantes abastecidos por água no município.
Resultados
a) O custo per capita foi de R$ 1, 43 (US$ 0,72) em 2009 e b) no período de 1989 a 2008, a estimativa do custo per capita variou de R$ 1,19 a R$ 1,43 (US$ 0,59 a 0,72).
Conclusão
O custo per capita da fluoretação da água é baixo, comprovando que, quando praticada com os níveis de fluoreto recomendados, torna-se uma medida de saúde pública eficiente, simples e segura para a prevenção da cárie dentária. Estimar seu custo é importante para efeito de comparação e incentivo a sua implementação para outros municípios.
Termos de indexação: Cárie dentária. Fluoretação. Abastecimento de água.
INTRODUCTION
Fluoridation of the public water supply is considered one of the top ten public health measures of the 20th century1, but its efficacy, effectiveness, toxicity, and cost are still questioned2. Its temporary or permanent discontinuation, or fluoride levels below the recommended levels prevents dental caries less effectively3.
According to the National Survey of Basic Sanitation4, 45% of the Brazilian municipalities fluoridated their water supply by the year 2000, and by 2008, this percentage had increased to 60.6%5. Despite this increase, water fluoridation does not yet benefit all Brazilians: those in rural and city outskirt areas are possibly left out. These are the areas that most require fluoridation because of the low socioeconomic level of their inhabitants, increasing inequalities6.
Given that dental caries is still the main oral health problem of the Brazilian population, water fluoridation is one of the most effective means of maintaining low levels of fluoride in the oral cavity. The anticariogenic action of fluoride is widely recognized. In terms of public health, the effects are greater when water is used as vehicle because of its widespread use and lower cost7.
According to water treatment plants, the factors that prevent water fluoridation include the high cost of installing the necessary equipment and the cost of the chemicals8. In 1974, water fluoridation became compulsory in all Brazilian municipalities with water treatment plants9. Therefore, analyzing the cost of implementing and maintaining water fluoridation may technically subsidize the municipalities that wish to implement and maintain it because it is an efficient, simple, inexpensive, and safe public health measure when the fluoride levels are correct10-12. The objectives of this case study were: a) to estimate the cost of water fluoridation per capita in 2009; b) to describe its costs from 1989 to 2008; and c) to analyze the dental caries indices since the implementation of water fluoridation in 1973.
METHODS
In 2009 Sorocaba had an estimated population of 584,313 inhabitants13, and by 2008, 99% of this population had piped water at home14.
In Sorocaba, water fluoridation is performed by the Autonomous Water and Wastewater Service (SAAE) of Sorocaba, an autonomous municipal water and wastewater treatment plant. There are two plants: ETA 1 (Cerrado) supplies water to 90% of the city, has been fluoridating water since October 1973, and treats 2000 liters of water per second15; and ETA 2 (Éden) has been fluoridating water since 1982 and treats as much as 200 liters of water per second15.
The two plants were studied. The data provided by SAAE were: cost reports for the equipment, chemicals, system operation, and control of fluoride concentration in the water supply. The companies that provided the equipment were also consulted. Calculation of the costs included10:
Initial capital (IC)
a) equipment: metering pump; storage tanks; fluoride concentration control and testing equipment; b) installation: represents 85% of equipment cost16-17; c) technical consultancy: represents 15% of the initial capital17-18.
The initial capital was stratified by twenty years, the equipment lifetime. This calculation included the initial capital plus technical consulting divided by twenty (number of years).
Cost of the chemicals (CC)
The fluoride added to reach the recommended concentration of 0.7 ppm took the fluoride present naturally in the water into account. The cost is given by ton of product.
System operating cost (SOC)
a) equipment depreciation and maintenance: these represent roughly 10% of the initial capital distributed according to equipment lifetime; b) electricity: percentage of the costs with electricity for the two ETA plants divided by the proportion of electricity cost for running the fluoridation pumps; c) human resources: mean annual cost of the salaries and labor costs of the water treatment plant operators (one operator per plant).
Cost of controlling fluoride concentration (CCFC)
a) metering and control equipment (fluorometer): fixed amount already added to the initial capital required for implementing water fluoridation; b) chemical products: reagents; c) ion-selective electrodes: lifetime of one year17.
The cost of water fluoridation per capita per year was given by the following formula10:
Fluoridation cost indicator: (IC + CC + SOC + CCFC) / city population
This estimate included the cost divided by the number of inhabitants of Sorocaba who received fluoridated water, estimating the cost of the system/year and the cost of the system/person/year in 2009.
The cost of operating the system from 1989 to 2008 included the operating costs and costs with chemicals. The initial capital was stratified for twenty years. However, SAAE only provided the cost of controlling the fluoride concentration for the year of 2009, so the estimated cost of controlling the fluoride concentration from 1989 to 2008 was given by multiplying it to the percentage of this cost in 2009 in relation to the total cost of the same year, that is, 1.47%. Therefore, the cost of controlling the fluoride concentration from 1989 to 2008 was given by multiplying the total cost of that period by 1.47%.
RESULTS
The chemical used today is fluosilicic acid (FSA), which is added at the end of the water treatment process.
In ETA Cerrado the water has a natural fluoride concentration of roughly 0.11 mg/L and fluoridation is done by a gravimetric rotameter. In ETA Éden the water has a natural fluoride concentration of 0.3 mg/L and fluoridation is done by a metering pump.
All costs provided by SAAE were expressed in reais, the current Brazilian currency.
Initial capital (IC)
Table 1 shows how the initial capital (IC) was calculated. The equipment cost was added to the installation cost (85% of the equipment cost) and to the technical consultancy cost (15% of the initial capital). The total cost was R$ 295,423.05, which divided by 20 years gives R$ 16,697.82. 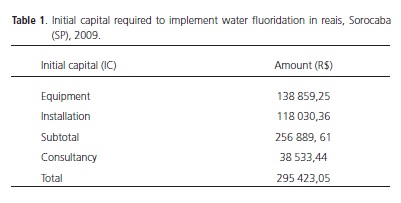
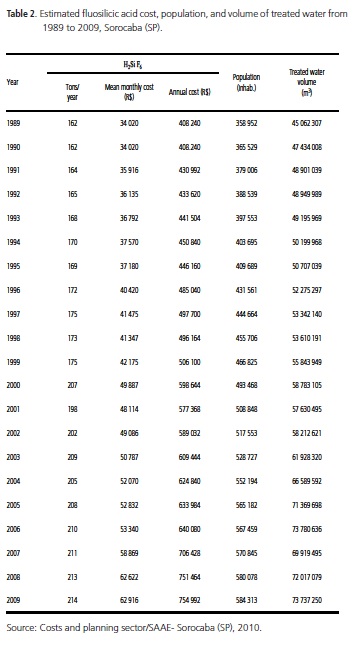
Cost of the chemicals (CC)
Table 2 shows the total amount of fluosilicic acid (H2SiF6) used per year in tons, mean monthly and annual costs of purchasing the chemicals in reais, number of Sorocaba, , and volume of treated water in liters from 1989 to 2009 in Sorocaba (SP).
System operating cost (SOC)
a) equipment depreciation and maintenance (10% of the IC); b) electricity: amount consumed by the pumps of the two plants, which corresponded to 0.025% of the total electricity used by ETA Cerrado and to 0.053% of the total electricity used by ETA Éden (SAAE); c) human resources.
Table 3 shows the cost of operating the system from 1989 to 2009 in reais. 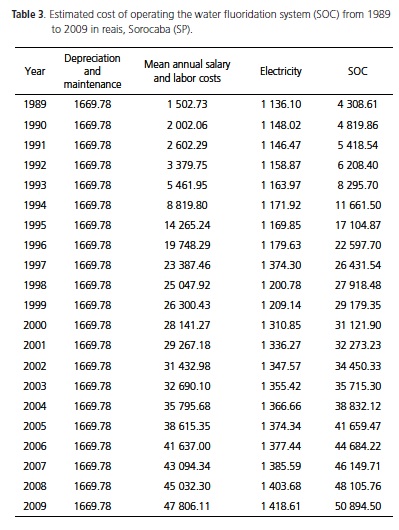
Cost of controlling fluoride concentration (CCFC)
The fluoride concentration at ETA Cerrado is controlled by an ion-selective electrode, with ten analyses being performed per day, and three electrodes being bought per year, and by the SPADNS method (twelve analyses per day). ETA Éden uses only the SPADNS method. The costs include laboratory glassware and the reagents required for both methods (TISAB II, standard fluoride solution, SPADNS reagent). The costs of the necessary equipment, namely spectrophotometers and potentiometers, have already been included in the initial capital.
The cost of controlling fluoride concentration from 1989 to 2008 was given by multiplying the percentage of this cost by the total cost of the initial capital and of operating the system and purchasing reagents in 2009, that is, by 1.47%.
Dividing the cost indicator formula (represented by adding the costs of the initial capital, chemicals, system operation, and fluoride concentration control) by the estimated population of Sorocaba (SP) in 2009 we get:

Hence, the cost of fluoridating water in Sorocaba (SP) in 2009 was R$ 1.43 reais/person/year (0.72 USD/ person/year). Reais was converted into dollars by multiplying the amount in reais by the average selling rate practiced by banks in 2009, which was of R$ 1.99 per dollar.
Table 4 shows the final composition of the estimated cost in reais/person/year of fluoridating the public water supply of Sorocaba, SP, from 1989 to 2009. The total cost includes the initial capital for implementing the system, the chemicals, and the cost of operating the system, which were provided by SAAE, and the cost of controlling the fluoride concentration in the water (given by multiplying the total cost of the system from 1989 to 2008 by 1.47%, as described previously).
Studies done in 1974, twelve months after the implementation of water fluoridation in the municipality of Sorocaba16, and in 198519 investigated the prevalence of caries in schoolchildren aged 7 to 12 years using the same indices.
Other epidemiological oral health studies done in 1999, 2002, and 2006 included schoolchildren aged 7 to 12 years attending public schools. Table 5 shows their decayed-missing-filled (DMF) index. The listed studies used different study designs and sampling methods20.


DISCUSSION
Manau et al.21 compared the costs of water fluoridation with semimonthly gargling with a 0.02% sodium fluoride (NaF) solution at school and supervised tooth brushing with fluoride toothpaste, also at school. The estimated cost of water fluoridation (installation, equipment, chemicals, maintenance) was US$ 0.39, and those of semimonthly gargling and supervised tooth brushing were US$ 2.24 and US$ 8.80, respectively. Water fluoridation is not only cheaper, but also more widespread, benefitting the entire population and making the measure highly efficient.
O'Connell et al.22 estimated that water fluoridation in Colorado, United States of America (USA), resulted in savings of 148.9 million dollars in 2003, or approximately US$ 60.78 per person.
For the American Dental Association (ADA)23, water fluoridation is profitable. In most American communities, each dollar spent on water fluoridation saves 38 dollars of dental treatment.
According to the Center for Studies in Public Health (NESP)24, the cost of water fluoridation in Brazil, considering initial capital, chemicals, and system operation, is estimated to be R$ 0.13 per person per year.
According to the Guide to community-preventive services25, the estimated mean water fluoridation cost of 2002 varied from US$ 2.70 per person in towns with up to 5,000 inhabitants to US$ 0.40 per person in towns with more than 20,000 inhabitants.
Frias et al.10 estimated the mean annual cost of water fluoridation in São Paulo, SP, from 1985 to 2003 to be R$ 0.08 (US$ 0.03) per person; this estimate included the initial capital required for implementing the system, chemicals, cost of operating the system, and cost of controlling fluoride concentration. The accumulated cost in 18 years was R$ 1.44 (US$ 0.97) per person. According to the author, the results should be interpreted with caution because of the economic characteristics of each country, state, and city, population, and the data collection criteria and methods.
In Sorocaba, water fluoridation in 2009 cost R$ 1.43 (US$ 0.72) per person and the estimated cost for the period from 1989 to 2009 varied from R$ 1.19 to R$ 1.43. These costs are much higher than those estimated by Frias et al.10, probably because of the municipal demographic profile.
The present study found that the most expensive item associated with water fluoridation is the cost of the chemicals, representing more than 90% of the total cost, which varied insignificantly over the 20-year study period.
An epidemiological study conducted in 197418 in Sorocaba, 12 months after the implementation of water fluoridation, found DMF indices of 2.77; 3.62; 4.87; 6.11; 8.06, and 9.78 for children aged 7, 8, 9, 10, 11, and 12 years, respectively.
A study conducted by the Pontifical Catholic University of Campinas in 1985 covering the period from 1973 to 198519 found DMF indices of 1.85, 2.88, 4.26, 5.65, 7.68, and 9.35 for children aged 7, 8, 9, 10, 11, and 12 years, respectively. The caries prevalences in children aged 7, 8, 9, 10, 11, and 12 years decreased by 33.22%, 20.45%, 12.53%, 7.53%, 4.72%, and 4.40%, respectively. The study concluded that the reduction in the prevalence of dental caries between 1974 and 1985 did not reach the mean found by similar studies conducted in other municipalities that fluoridated their waters during the same period, such as Campinas. In Campinas, ten years after the implementation of water fluoridation, the prevalences of dental caries in children aged 7, 8, 9, 10, 11, and 12 decreased by 70.76%, 55.84%, 50.92%, 55.21%, 45.20%, and 50.68%, respectively. The low reduction in the prevalence of caries observed during the period may be due to irregular water fluoridation. The SAAE may not have maintained the appropriate fluoride concentrations in the first 12 months of water fluoridation because of interruptions or inadequate fluoride addition to the water, and only maintained the appropriate fluoride concentrations during 3 or 4 years. Effective control of water fluoridation began in 1995, when the Paulista Association of Dental Surgeons - Sorocaba Division (APCD) and University of Campinas' (Unicamp) biochemistry laboratory began to test the water fluoride concentration quarterly, and found optimal fluoride concentrations for caries prevention, a procedure that continues to this day (APCD, 1990 - 0.76 ppm; 1995 - 0.76 ppm; 1996 - 0.74 ppm; 1997 - 0.72 ppm; 1998 - 0.72 ppm; 2005 - 0.70 ppm; 2006 - 0.73 ppm; 2007- 0.67 ppm; 2008 - 0.69 ppm; 0.69 ppm; 2009 - 0.66 ppm)26. This shows the need of maintaining the optimal fluoride concentration effectively to obtain the desired results.
Comparison of the DMFTs of 1985 to 1999 shows that the caries prevalence in children aged 12 years dropped 75.4%; the prevalence of 1985 is classified as very high by the World Health Organization (WHO), but that of 1999 is classified as low. In 2002, the DMFT was 40% lower than the previous finding. Subsequent studies have shown that caries prevalence continues to decrease, proving that water fluoridation and its monitoring, greater availability of fluoride toothpastes, and other health care measures are effective. As a matter of fact, the DMFT of 12-year-olds was 1.04 in 2006, 24.65% lower than the previous finding and classified as very low by the WHO20.
The Oral Health Conditions in the State of São Paulo in 200227 found a DMFT of 2.5 for children aged 12 years, 6.4 for children aged 15 to 19 years, 20.3 for adults, and 28.2 for the elderly. A national study conducted in 1986 found a DMFT of 6.0 for children aged 12 years from the Brazilian Southeast. This number decreased significantly in the state of São Paulo, reaching 3.7 in 1998 and 2.5 in 2002. The DMFT of 12-year-olds from municipalities that fluoridate their water is 2.3, while for those from municipalities that do not, it is 3.5. Thus, dental caries is 34.3% more prevalent in locations without water fluoridation. Although not as expressive, the same is observed in 5-year-olds: the mean dmft in municipalities with and without fluoridated water is 2.2 and 3.1, respectively, a difference of 29%.
In 2003 Cypriano et al.28 reported the prevalence and severity of caries in preschoolers aged 5 to 6 years and schoolers aged 7 to 12 years from seven municipalities representative of the region of Sorocaba, SP, exposed or not to fluoridated water. The 5-year-olds had a dmft of 3.1, and 37.6% were caries-free (dfmt=0). The 12-yearolds had a DMFT of 2.6, and 32.3% were caries free. The caries prevalence in the region is considered low. Children of all ages presented better oral health conditions in municipalities with fluoridated water; the proportion of caries-free 12-year-olds was higher (p=0.019), and the dmft was lower (p=0.001). The oral health goal of the WHO/International Dental Foundation (IDF) for 2000 for 12-year-olds was achieved, but 30.1% of the children had a DMFT higher than 3.0. The goal for 5-year-olds was not achieved given that only 37.3% of the children were caries free. These groups require special care to meet their needs.
Today the population in greatest need of dental care is that with the highest DMFT. Thus, this is one more argument in favor of water fluoridation. Frazão et al.29 confirm this statement in a study about early tooth loss in adults aged 35 to 44 years, reporting that, in a context of high caries prevalence, water fluoridation, age, and socioeconomic status help to prevent tooth loss in this age group.
The study results show that water fluoridation continues to benefit oral health considerably, which is essential in communities with high proportions of low-income children or people in general. Moreover, water fluoridation has a very good benefit-cost ratio for preventing dental caries, even in locations where the incidence of dental caries has decreased in the last years. In Brazil, water fluoridation is very beneficial and should be always maintained at the optimal fluoride concentration30.
CONCLUSION
In Sorocaba the per capita cost of water fluoridation was low during the study period. The present study corroborates others showing that when the recommended fluoride concentrations are observed, water fluoridation is an effective, simple, and safe public health measure for preventing dental caries. Estimating its cost allows comparisons between studies and encourages its implementation by municipalities that have not yet adhered to the practice.
Although the epidemiological studies of dental caries mentioned herein use different methods, secondary data analysis showed a significant decrease in the prevalence of dental caries. A DMFT of 1.04 is considered very low by the WHO.
Collaborators
ÉHS MARTINEZ designed the study, analyzed and interpreted the data, and wrote the article. AC FRIAS analyzed and interpreted the data, and wrote and critically reviewed the article. HJ MENDES conceived and designed the study, analyzed and interpreted the results, and wrote and critically reviewed the article. KPK OLYMPIO designed the study, analyzed and interpreted the data, and wrote and critically reviewed the article.
REFERENCES
1. Centers for Disease Control and Prevention. Populations receiving optimally fluoridated public drinking water- United States, 1992- 2006. MMWR Morb Mortal Wkly Rep. 2008;57(27):737-41. [ Links ]
2. Narvai PC. Cárie dentária e flúor: uma relação do século XX. Cienc Saude Coletiva. 2000;5(2):381-92. doi: 10.1590/S1413- 81232000000200011.
3. Burt BA, Fejerskov O. Water fluoridation. In: Fejerskov O, Ekstrand J, Burt BA eds. Fluoride in dentistry. 2 ed. Copenhagen; Munksgaaard; 1996. p. 275-90.
4. Instituto Brasileiro de Geografia e Estatística (IBGE). Ministério do Planejamento, Orçamento e Gestão. Pesquisa Nacional de Saneamento Básico 2000. Rio de Janeiro: 2002. [cited 2010 mar 8]. Available from: <http://www.ibge.gov.br/home/ estatistica/populacao/condicaodevida/pnsb/pnsb.pdf>.
5. Instituto Brasileiro de Geografia e Estatística (IBGE). Ministério do Planejamento, Orçamento e Gestão. Pesquisa Nacional de Saneamento Básico 2008. Rio de Janeiro: 2010. [cited 2010 ago 24]. Available from: <http://www.ibge.gov.br/home/estatistica/ populacao/condicaodevida/pnsb2008/PNSB_2008.pdf>.
6. Antunes JLF, Narvai PC. Políticas de saúde bucal no Brasil e seu impacto sobre as desigualdades em saúde. Rev Saude Publica. 2010;44(2):1-6. doi: 10.1590/S0034-89102010005000002.
7. Murray JJ. O uso correto de fluoretos em Saúde Pública. São Paulo: OMS/Santos; 1992.
8. Pinto VG. Saúde bucal coletiva. São Paulo; Santos; 2000. p.353- 401.
9. Brasil. Ministério da Saúde. Lei n. 6050, de 24 de maio de 1974. Dispõe sobre a fluoretação da água em sistemas de abastecimento quando existir estação de tratamento [texto na Internet]. Diário Oficial da União, Brasília (DF); 1974 Maio 27 [citado 2010 Ago 24]. Disponível em: < http://presrepublica. jusbrasil.com.br/legislacao/128460/lei-6050-74>.
10. Frias AC, Narvai PC, Araujo ME, Zilbovicius C, Antunes JLF. Custo da fluoretação das águas de abastecimento público, estudo de caso: município de São Paulo, Brasil, período de 1985-2003. Cad Saude Publica. 2006;22(6):1237-46. doi: 10.1590/S0102- 311X2006000600013.
11. Rugg-Gunn A, Villa AE, Buzalaf MAR. Contemporary biological markers of exposure to fluoride. In: Buzalaf MAR. Fluoride and the oral environment. Basel: Karger; 2011. p 37-51.
12. Frazão P, Peres MA, Cury JA. Qualidade da água para consumo humano e concentração de fluoreto. Rev Saude Publica. 2011; 45(8):964-73. doi: 10.1590/S0034-89102011005000046.
13. Instituto Brasileiro de Geografia e Estatística. IBGE-Cidades [citado 2010 Mar 8]. Disponível em: <http://www.ibge.gov.br/ cidadesat/topwindow.htm?1>.
14. Brasil. Ministério das Cidades. Secretaria Nacional de Saneamento ambiental. SNIS. Sistema Nacional de Informações sobre saneamento [citado 2010 Mar 30]. Disponível em: <http:// www.snis.gov.br/>.
15. Serviço Autônomo de Água e Esgoto. SAAE. [citado 2010 Mar 30]. Disponível em: <www.saaesorocaba.sp.gov.br>. 16. São Paulo (Estado). Secretaria de Estado da Saúde. Divisão Regional de Saúde de Sorocaba DRS4. Inspetoria de Odontologia Sanitária. Prevalência da cárie dental em escolares da rede de ensino estadual da cidade de Sorocaba. Sorocaba: Secretaria de Estado da Saúde; 1974.
17. Centers for Disease Control and Prevention, Public Health Service, US Departament of Health and Human Services. Water fluoridation: a manual for engineers and technicians. Washington: Centers for Disease Control and Prevention; 1991.
18. Centers for Disease Control and Prevention. Engineering and administrative recommendation for water fluoridation. MMWR Recomm Rep. 1995;44(RR-13):1-40.
19. São Paulo (Estado). Secretaria de Estado da Saúde. Análise dos dados de prevalência de cárie dentária na cidade de Sorocaba/ SP/Brasil, depois de implantado o sistema de fluoração das águas de abastecimento público. Período 1973/1985. Sorocaba: Secretaria de Estado da Saúde; 1985.
20. Sorocaba. Prefeitura Municipal de Sorocaba. Secretaria da Saúde. Levantamento epidemiológico em saúde bucal nos escolares de 5 a 14 anos da rede pública de Sorocaba. Sorocaba. Prefeitura Municipal de Sorocaba; 2006.
21. Manau C, Cuenca E, Martinez-Carretero J, Saleras L. Economic evalution of community programs for the prevention of dental caries in Catalonia,Spain. Community Dent Oral Epidemiol. 1987;15(6):292-300. doi: 10.1111/j.1600-0528.1987. tb01738.x.
22. O'Connell JM, Bruson D, Anselmo T, Sullivan PW. Costs and Savings Associated With Community Water Fluoridation Programs in Colorado. Prev Chronic Dis. 2005;2(special issue):1-13.
23. American Dental Association. After 60 years of success in fighting dental decay: water fluoridation still lacking in many communities [cited 2009 set 21]. Available from: <www.ada. org>.
24. Núcleo de Estudos de Saúde Pública. Universidade de Brasília. A fluoretação das águas de abastecimento público [texto na Internet]. [citado 2009 Set 21] Available from: <www.nesp.unb. br/saudebucalaids/fluoretacaodeaguas.pdf>.
25. Community Guide Branch. National Center for Health Marketing (NCHM). Centers for Disease Control and Prevention. Guide to community preventive services 2002. Preventing dental caries: community water fluoridation [text Internet]. [cited 2010 Mar 30]. Available from: <http://www.thecommunityguide.org/oral/ fluoridation.html>.
26. Associação Paulista de Cirurgiões-Dentistas Regional Sorocaba. Relatórios do Programa de monitorização do flúor na água de abastecimento de Sorocaba. Sorocaba: Associação Paulista de Cirurgiões-Dentistas; 1990, 1995 a 1998, 2005 a 2009.
27. São Paulo (Estado). Secretaria de Estado da Saúde. Faculdade de Saúde Pública da Universidade de São Paulo. Condições de saúde bucal no estado de São Paulo em 2002. São Paulo: 2002. [citado 2010 Mar 30].<http://www.saude.sp.gov.br/resources/gestor/ destaques/saude_bucal/condicoes_de_sau de_bucal,2002.pdf>.
28. Cipriano S, Pecharki GD, Sousa MLR, Wada RS. A saúde bucal de escolares residentes em locais com ou sem fluoretação nas águas de abastecimento público na região de Sorocaba, São Paulo, Brasil. Cad Saude Publica. 2003;19(4):1063-71. doi: 10.1590/S0102-311X2003000400028.
29 Frazão P, Antunes JLF, Narvai PC. Perda dentária precoce em adultos de 35 a 44 anos de idade: Estado de São Paulo, Brasil, 1998. Rev Bras Epidemiol. 2003;6(1):49-57. doi: 10.1590/ S1415-790X2003000100007.
30. Thylstrup A. Clinical evidence of the role of pre-eruptive fluoride in caries prevention. J Dent Res. 1990;69(special issue):742-50.
 Endereço para correspondência:
Endereço para correspondência:
EHS MARTINEZ
e-mail: ericasgroi@hotmail.com
Received on: 29/6/2012
Final version resubmitted on: 28/9/2012
Approved on: 9/10/2012
