










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.4 Porto Alegre Out./Dez. 2013
ORIGINAL / ORIGINAL
Knowledge of pregnant before and after of the application of an educational manual in oral health
Conhecimento de gestantes antes e depois da aplicação de um manual educativo em saúde bucal
Adriana Maria Fuzer Grael TINOSI; Sílvia Helena de Carvalho SALES-PERESI
I Universidade de São Paulo, Faculdade de Odontologia, Departamento de Odontopediatria, Ortodontia e Saúde Coletiva. Al. Octávio Pinheiro Brisolla, 9-75, 17012-901, Bauru, SP, Brasil.
ABSTRACT
Objective
To evaluate the knowledge degree about oral health in a group of pregnant of the municipal district of Dois Córregos, São Paulo, before and after the application of an educational manual.
Methods
In the first stage, 60 pregnant users of the Only System of Health, chosen by chance, answered to a questionnaire where themes were approached as oral health in the gestation, feeding, breast-feeding, oral hygiene and fluoride. In the second stage, they received an educational manual with those same themes and they participated of a lecture with the intention of to discuss him referred manual and to heal eventual doubts that could appear during the reading of the same. After the lecture, a second questionnaire was applied to evaluate the acquired knowledge.
Results
Some knowledge was observed with relationship to the transmission of the mother's cariogenics bacteria for the baby, because, in the beginning 56.7% they affirmed that it can happen, increasing for 69.7% at the concluded of the study. It was also verified, the interest of the pregnant for the subject, since everybody agreed to be important to receive referring information to the oral health during the gestation.
Conclusion
The pregnant present some knowledge about oral health that can be improved by means of educational, preventive and healing programs. This group exert big it influences in the family ambit, could act as agents multipliers and avoiding the child's precocious contamination.
Indexing terms: Oral health. Pregnancy. Pregnant women. Primary prevention.
RESUMO
Objetivo
Avaliar o grau de conhecimento sobre saúde bucal em um grupo de gestantes do município de Dois Córregos, São Paulo, antes e depois da aplicação de um manual educativo.
Métodos
Na primeira etapa, 60 gestantes usuárias do Sistema Único de Saúde, escolhidas aleatoriamente, responderam a um questionário onde foram abordados temas como saúde bucal na gestação, alimentação, amamentação, higiene bucal e flúor. Na segunda etapa, receberam um manual educativo com esses mesmos temas e participaram de uma palestra no intuito de se discutir o referido manual e sanar eventuais dúvidas que pudessem surgir durante a leitura do mesmo. Ao final da palestra, foi aplicado um segundo questionário para avaliar o conhecimento adquirido.
Resultados
Observou-se algum conhecimento com relação à transmissão de bactérias cariogênicas da mãe para o bebê, visto que, no início, 56,7% afirmaram que isto pode ocorrer, aumentando para 69,7% ao final do estudo. Constatou-se também, o interesse das gestantes pelo assunto, já que todas concordaram ser importante receber informações referentes à sua saúde bucal durante a gestação.
Conclusão
As gestantes apresentam algum conhecimento sobre saúde bucal, que pode ser melhorado por meio de programas educativos, preventivos e curativos. O grupo de gestantes exerce grande influencia em âmbito familiar, podendo atuar como agentes multiplicadores e evitando a contaminação precoce da criança, em relação às doenças bucais.
Termos de indexação: Saúde bucal. Gestação. Gestantes. Prevenção primária.
INTRODUCTION
The mother plays an important role in the family, establishing most of the time, their habits and customs1. Taking into account that in the case of health, it is common women receive the influence of mothers, grandmothers, aunts and neighbours in building their knowledge, often empirically based, and that certain lifestyle habits can lead to risk factors for several diseases2, the access of these mothers to correct health information, may represent an important tool for the promotion of health within the family. Therefore, it is important to make an early approach in this populational group under educational and preventive aspects, aiming not only prevent diseases, but also to limit the damage caused by them , when already settled2-4.
Pregnancy, for being a unique period in a woman's life, when health care should be bigger, is the ideal time to acquire new knowledge that enable the adoption of new habits and behaviours. The preoccupation with the welfare of the future baby makes the mother more receptive, which facilitates the educational process by favouring the incorporation and development of healthy habits5-7.
Maternal and child care has been prioritized by the Brazilian public health, especially with regard to prenatal care, which has led to a reduction in the rates of infant morbidity and mortality2,6. However, in relation to oral health, Andrade et al.9 found that preventive and educational programs in the dental field for pregnant women and babies have not been properly exploited and disseminated by public health system. According to Moura et al.6, the participation of mothers in these programs promotes a positive impact in relation to health practices adopted by them, allowing all family members to be benefited5.
The Dental Prenatal, as it is called the dental care of pregnant women, which should be further introduced in early pregnancy, consists in educate , guide and inform the pregnant woman on oral hygiene, healthy eating habits , breastfeeding, in addition to the care with the oral health of the baby. It also includes the performing of clinical procedures in order to recover and/or maintain their oral health10-15. Regarding dental caries, it is important to emphasize that the mother can transmit it to their children, not only through improper habits. Different studies have proven the occurrence of vertical transmission of pathogenic microorganisms, especially the Streptococcus mutans, from mother to baby mainly between the 19 and 31 months old child, a period called "window of infectivity". Hence the need of maternal oral microbiota be compatible with health1,14,16-20.
However, the presence of myths and beliefs about dental care during pregnancy, limits the access to this important population portion to dental care, and the fear that the treatment could harm the baby, constitutes the main cause of evasion of service. On the other hand, it is still common the refusal by the dentist in performing clinical procedures in these patients, often because of the lack of technical and scientific knowledge, leading pregnant women to seek solutions to their oral problems based on empiricism, which could bring harm to maternal health. It is also observed little educational approach by these professionals, a factor that contributes to the demotivation of pregnant women in caring for their oral health5,7,21. It is the duty of the dentist to learn about the importance of dental activity during pregnancy, as well as actively participate in the prenatal team, demystifying the idea that being pregnant, the woman should postpone the dental treatment, when in fact it is in that stage she most needs the attention of the dentist10,14,22-24. Thus, the objective of this study was to assess the knowledge of oral health of pregnant women before and after implementation of an educational manual, in order to contribute to the development and implementation of educational and preventive programs, so important for the health of binomial mother- child.
METHODS
The research was conducted in the city of Dois Córregos (SP), in the period between March and August in 2008.
With regard to health, that municipality, which has a population of approximately 24,400 inhabitants, currently has 1 hospital, 1 emergency room (ER), 1 Health Community Agents Program (PACS ), 2 Basic Health Units (UBS ) and 3 Family Health Programs (PSF), the latter two being, the locations where the data of the 1st phase of this survey were collected. To conduct this study, in a quantitative nature, we used a sample of 60 user pregnant women in the National Health System, which were randomly chosen.
The pregnant women were approached while waiting for prenatal consultation, after signing a free and enlightened consent term. A questionnaire with objective questions, in which were explored topics such as oral health during pregnancy, feeding, breastfeeding, oral hygiene and fluoride was applied. Then, the pregnant women received an educational manual focusing on the subjects questioned. In a second stage of labour, a lecture was performed in order to discuss the manual and remedy any questions that might arise during the reading of it. At the end of the lecture, was administered a questionnaire covering the same topics, with the aim of assessing the knowledge gained.
The present study was initiated after approval by the Research Ethics Committee of the Faculty of Dentistry in Bauru, University of São Paulo (process number 004/2008). The women signed a Free and Enlightened Consent Term, according to Resolution 196/96 of the National Health Council, which regulates the guidelines and standards for research involving humans. The analysis of the results was descriptive, by means of absolute and relative frequencies, presented in tables and graphs.
RESULTS
Initially, 60 patients were included in the study who answered the questionnaire, but at the end of the study there were only 33 participants.
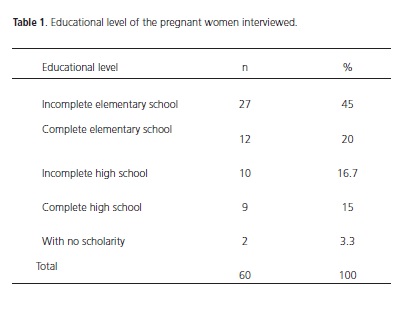
The age of the pregnant women interviewed ranged from 15 to 41 years old, 38.3% were aged 15- 20 years old, 35% between 21-29 years old and 26.7% over 30 years old. As the level of education, the majority (45%) had incomplete primary education , 20% complete primary, 16.7% incomplete high school, 15% complete high school and 3.3% reported being illiterate (Table 1). 80% of participants in this research have reported taking care of the household chores.
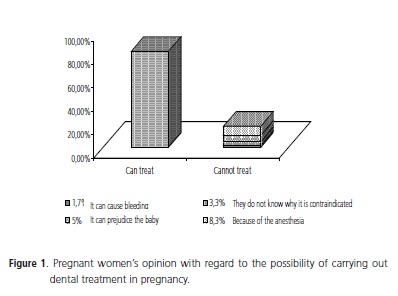
When asked to pregnant women in the initial phase of the study, if they had received guidance from their obstetric doctor to look for a dental service, only one (1.7%) gave an affirmative answer, because she had complained about tooth sensitivity. During the first phase, with respect to the fact that pregnant women can perform dental treatment, 81.7% said there was no problem in treating the teeth, while 8.3% said they could not because of the anaesthesia, 5% believe that this treatment can harm the baby, 1.7% mentioned the possibility of treatment cause bleeding and 3.3% did not know why the treatment is contraindicated. These results are shown in Figure 1.
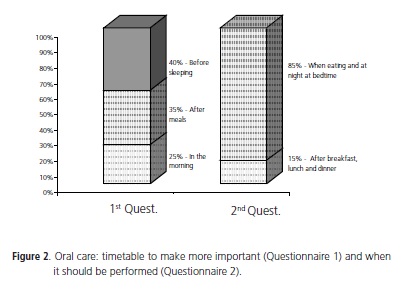
When they were questioned, in both phases of the study, if pregnancy increases the chances of oral diseases appear, initially, 75% answered yes, decreasing to 51.5% in the second questionnaire. In the first phase, 68.3% believed that pregnant women lose calcium from the teeth to form the structures of the baby, and in the second phase, 93.9% answered that the source of calcium for the baby is in the feeding of the pregnant woman. At the beginning of the study, 50% of respondents agreed that the feeding of pregnant women can influence the feeding preference of the future baby, increasing to 60.6% at the end of the study. With regard to oral hygiene, in the first phase was asked what the most important time to perform it, 40% answered before bedtime, 35% after meals and 25% said it was in the morning. In the second phase, when questioned about what moment the oral hygiene should be performed, 85% said always after eating and at bedtime, and 15% after breakfast, lunch and dinner (Figure 2).
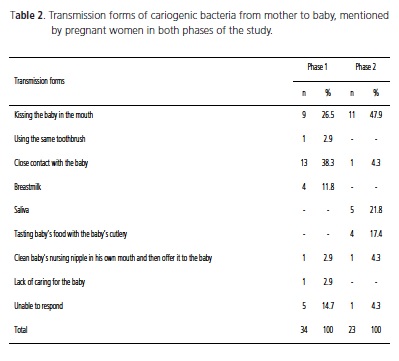
In relation to fluoride, initially 86.7% answered that it increases the tooth resistance. At the end of the study, all agreed that fluoride helps prevent tooth decay. When questioned, in the second phase, if the ingestion of toothpaste with fluoride by the child can cause problems, 69.7% answered yes. In the first questionnaire, 56.7% believed in the transmission of bacteria that cause tooth decay from mother to baby, increasing to 69.7% in the final questionnaire. Table 2 shows the forms of infection mentioned by the respondents. At the beginning of the study, 93.3% of the pregnant women believed in the influence of breastfeeding in a better development of the baby face and all agreed that it is important to receive guidance on oral health in pregnancy.
DISCUSSION
The participation of the individual in their own process of health/disease is crucial for the establishment of health promotion. Within this perspective professionals should develop educational strategies in health11.
For planning and evaluation of health actions, it is first necessary to diagnose the level of knowledge of the population, so that we can adopt the fundamental strategies in the process of transmission of information which influences the formation of behaviours that promote health8.
The non-attendance of all respondents at the lecture, can be justified by the difficulty of mobility of some pregnant women who lived distant from the site of the lecture, because some could not be located, due to moving, preventing them from being reported on the realization of the lecture, also others have already had their babies and reported being devoting most of their time in caring for them.
Although the questionnaires of both phases approach identical issues, some questions in the first questionnaire were not repeated in the second, and others were presented only in the second questionnaire. The most relevant questions were reapplied in the second stage, and in some of them, the same subject was asked differently. The educational level of the mother is an important factor to be considered, since it directly influences the construction of her health habits, moreover, the higher the level of knowledge, the better the health practices of these mothers. It was possible to observe in this study that the majority of pregnant women develop their chores at home, which makes them closer to their children, facilitating the transmission of habits and customs from mother to child.
The multidisciplinary approaching to the pregnant patient constitutes a fundamental practice for the success of maternal and child care programs, which aim to put the pregnant woman and the unborn baby in the philosophy of health promotion in an integral way. With regard to dental care during pregnancy, the involvement of the obstetric doctor, so important since he/she is considered the first professional to establish contact with the pregnant patients and whom they deposit all trust, it is not effective according to the present study, having as the most likely cause, the lack of access of these professionals to the information related to oral health. Feldens et al.23 observed that some actions adopted by physicians are devoid of scientific reasoning , such as prescribing fluoride supplements in prenatal care, which still occurs frequently, not bringing any benefit for teething children. Konishi & Abreu-e-Lima14 suggest greater disclosure by the dentists, of issues related to dentistry directed to the medical field and it can be performed through leaflets, articles, personal contact, thus facilitating the establishment of a link among these professionals.
Batistella et al.25 evaluated the oral health knowledge of 200 pregnant women through a questionnaire, of which 100 were users of the SUS (Unified Health System), and the other 100 patients from private clinics and found that 75% and 85% respectively, thought being good to perform dental treatment during pregnancy . A similar result was found during this work. Considering the importance and necessity in performing these treatments, Morandini & Vidotti26 warned regarding some particularities of this kind of service, since it is a special patient, undergoing physical, physiological and psychological changes, requiring a differentiated service, with the achievement of short consultations, judicious use of drugs and anaesthetics, exposure to x -rays only if necessary and always with proper protection as well as the achievement of a specific and complete anamnesis. Contact with the patient's physician is also crucial for the adoption of correct conduct by the dentist.
The belief that pregnancy "weakens" the teeth could be observed in this study, since most of the women responded pregnancy is responsible for the increase of oral diseases during this period. According to Oliveira4, behavioural changes, characteristics of this phase such as the increase in the frequency of food intake, increasing sleep and difficulty in performing effective oral hygiene because of dizziness and nausea common in pregnancy, can lead to increased rates of dental caries, also contributing to the occurrence of gum diseases, which can be exacerbated during this period because of the hormonal changes and increased blood circulation, quirky in pregnancy. It is also common, the association by pregnant women, between "weak teeth" in pregnancy and loss of calcium from mother teeth to form the calcified structures of the baby , which could be seen in the first phase of this study. Abdalla et al.22 stated that this calcium in the teeth of the pregnant woman is in a stable crystalline form, which prevents it from being available in the bloodstream, contrary to the myth that in pregnancy teeth become "weak" by the removal of calcium for the supply of foetal needs. According to Jorge & Raggio13, calcium used in the formation of the baby comes from the mother's feeding and in case of insufficient intake, reserves of calcium present in bone structures of the mother are used. It is important to guide the pregnant woman about the benefits of a balanced diet, rich in nutrients, which will directly influence the health of the unborn baby, as well as the losses resulting from the excessive consumption of sweets during pregnancy for both the teeth of pregnant women, as for the oral health of her unborn child. The possible influence of maternal diet on the feeding preference of the future baby should be considered, because from the 4th month of pregnancy, the early development of the palate baby occurs, causing it to begin to notice the taste of the food ingested by the mother food, allowing believe that high consumption of sweets by pregnant women may increase the susceptibility of child in preference for this type of food. According to Sales-Peres et al.15, it is possible to prevent tooth decay in the unborn baby by controlling the maternal diet during pregnancy, implementing new eating habits with low sucrose (sugar). In this study, most respondents agree that the feeding of pregnant women can influence the type of food that their child will prefer; this outcome is similar to that found by Alves10, where 61.7% thought that way.
Positive results regarding oral hygiene and the role of fluoride in preventing tooth decay could also be observed in this study. Taking into account the decrease in salivary flow during sleep, nocturnal oral hygiene constitutes an essential practice in the maintenance of oral health. Moreover, clarify that brushing should be done not only after the main meals, but also after the consumption of other foods throughout the day is also essential, especially in pregnancy, when there is an increase in the frequency of food intake.
The rational use of fluoride has emerged during the last decades, as an important method of combating dental caries, both in the preventive and therapeutic context. Despite the relevance of its use, Alves10 in his work, found that there are still many questions regarding the use of fluoride, whereas 51.7% of his respondents answered do not know its purpose, 28.3% believe that it acts as a protective factor for teeth and 18.3% associated the fluoride to teeth cleaning, which differs from the results obtained in this study. That author also noted the lack of knowledge by pregnant women with regard to the occurrence of dental fluorosis, since 51.7% believed that ingestion of fluoridated toothpaste by children would not cause problems. In the present study, this number was 30.3%, suggesting that, although most agree with the fact that children ingest fluoride toothpaste can cause losses, there is a need for greater dissemination on the subject.
During this study, we observed some knowledge on the part of pregnant women regarding the transmission of microorganisms from the mother to the baby and the possible forms of contagion. According to Navarro & Côrtes20, contamination of the child occurs through saliva by kissing on the mouth, blowing on food to be offered to the child, as well as the use of cutlery, glasses and metallic/ plastic utensils in common, because these objects allow about 1/3 of cariogenic microorganisms remain viable for up to seven hours after use by adults. It is important to clarify that this contagion can occur not only for the mother but also for any person who will have close contact with the child.
Encouraging breastfeeding arguably constitutes an important strategy for health promotion. According Tollara et al.27 it is the role of the dental professional guide and encourage the future mothers to breastfeed their children, taking into account the muscle work done by the baby during the act of breastfeeding. In their works, Araújo et al.11 and Antunes et al.28 stated there are numerous benefits provided by breastfeeding for both the mother and the baby, in the case of the woman who breastfeeds, the benefits range from increased affective mother-child bond to the prevention of various cancers. Regarding the baby, beyond the obvious nutritional and psychological value, there is the immune factor conferring protection against infections and allergies, and this is the main quality of breast milk. From dental and phonological point of view, breastfeeding promotes the correct development of dent facial because during sucking of the breast, the children establish the correct pattern of nasal breathing and swallowing, thus preventing the chronic oral breathing, and contributes in obtaining a normal occlusion, leading eventually to a proper mastication. Another advantage of breastfeeding is that the child meets the physiological need of suction, which does not occur with artificial feeding (bottle), in which the nutritional satisfaction is achieved in just a few minutes, since the flow of food is much higher, leading the children to adopt non-nutritive sucking habits (nursing nipple, finger) to satisfy their natural need for suction.
The increase in the interest of pregnant women in information and new knowledge, reported in the literature comes from meeting with the result obtained in this study, where all mothers said that they find important to receive information on oral health during pregnancy, similar to that found by Batistella et al.25, considering that 97.5% of their respondents answered that they wish to receive more information.
The fact that the pregnant woman be more receptive to new knowledge makes pregnancy an excellent time to conduct educational and preventive actions, which will promote the adoption of best health practices by these patients, enabling act as health promoters in their homes.
CONCLUSION
Based on these, we conclude that despite pregnant women having some knowledge about oral health it is necessary to develop and implement programs aimed at caring for these patients in an integral manner. The participation of physicians, as well as the inclusion of the dentist on the team of prenatal care, is critical to the success of these programs, making it possible to demystify the beliefs involving dental care during pregnancy.
Collaborators
AMFG TINÓS worked in theoretical conception, performed the data collection, organized the database, participated in the analysis of the results and wrote the article. SHC SALES-PERES worked on the theoretical framework of the methodology, to guide the discussion and the writing of the article.
REFERENCES
1. Fakhouri AP, Bastos JR, Bastos JRM, Peres AS, Aquilante AG, Castro RFM, Pagani MM. Educação e prevenção em saúde bucal para gestantes. Odontol Soc. 2002;4(1):44. [ Links ]
2. Knupp RRS, Medeiros UV, Mello PBM, Ferreira DC, Rendeiro MMP, Lopes MGM. Análise de conhecimentos e práticas de mães sobre saúde bucal [text in Internet]. In: 6º Seminário do Projeto Integralidade Gestão em redes - Racionalidades e práticas novas de avaliação, formação e participação na saúde; 2006; Rio de Janeiro. Anais eletrônicos. Rio de Janeiro: CEPESC: ABRASCO, 2006 [2007 Oct 23]. Available in: <http://www.lappis.org.br/ site/o-que-fazemos/publicacoes/235-resumos-ampliados-do-viseminario- do-projeto-integralidade.html>.
3. Miller MC. The pregnant dental patient. J Calif Dent Assoc. 1995;23(8):63-70.
4. Oliveira AM. Pré-natal odontológico: mitos e dúvidas mais comuns das gestantes. Rev AONP. 2003;13:24-5.
5. Codato LAB, Nakama L, Melchior R. Percepções de gestantes sobre atenção odontológica durante a gravidez. Ciênc. Saúde Coletiva. 2008;13(3):1075-80. doi: 10.1590/S1413- 81232008000300030.
6. Moura LFAD, Moura MS, Toledo OA. Conhecimentos e práticas em saúde bucal de mães que freqüentaram um programa odontológico de atenção materno-infantil. Ciênc Saúde Coletiva. 2007;12(4):1079-86. doi: 10.1590/S1413- 81232007000400029.
7. Silva SRC, Rosell FL, Valsecki Junior A. Percepção das condições de saúde bucal por gestantes atendidas em uma unidade de saúde no município de Araraquara, São Paulo, Brasil. Rev Bras Saúde Matern Infant. 2006;6(4):405-10.
8. Pinto LF, Malafaia MF, JA, Baccaro A, Soranz DR. Perfil social das gestantes em Unidades de Saúde da Família do município de Teresópolis. Ciênc Saúde Coletiva. 2005;10(1):205-13. doi: 10.1590/S1413-81232005000100027.
9. Andrade FP. Assistência a gestantes e bebês no serviço público de saúde. Odontol Soc. 2002;4(1):79.
10. Alves VP. Análise do grau de conhecimento e aprendizado em saúde bucal de gestantes residentes em Pederneiras - SP [monograph]. Bauru: University of São Paulo; 2003.
11. Araújo JJ, Pereira AFF, Bassi AK, Zampronio AK, Caldana ML, Bastos JRM. Promoção de saúde materno-infantil. In: Bastos JRM, Sales-Peres SHC, Caldana ML. Educação em saúde: com enfoque em odontologia e fonoaudiologia. Bauru: Santos; 2007. p. 35-42.
12. Flório FM, Pereira AC. Alicerce para a promoção de saúde bucal: o início precoce. In: Pereira AC. Odontologia em saúde coletiva: planejando ações e promovendo saúde. Porto Alegre: Editora Artmed; 2003. p. 413-25.
13. Jorge LC, Raggio DP. Odontologia X Gestação. Jornal do Site [Internet periodic]. 2004 [access 2007 Oct 23];6(87):[about of 2p.]. Available in: <http://www.jornaldosite.com.br/arquivo/ anteriores/liliane/artliliane87.htm>.
14. Konishi F, Abreu-e-Lima F. Odontologia intra-uterina. Rev Bras Odontol. 2002;59(5):294-5.
15. Peres SHCS, Cardoso MTV, Garcez RMV, Peres AS, Bastos JRM. Tratamento alternativo de controle da cárie dentária no período materno-infantil. Rev Assoc Paul Cir Dent. 2001;55(5):346-50.
16. Alaluusua S. Transmission of mutans streptococci. Proc Finn Dent Soc. 1991;87(4):443-7.
17. Brambilla E, Felloni A, Gagliani M, Malerba A, García-Godoy F, Strohmenger L. Caries prevention during pregnancy: results of a 30 month study. J Am Dent Assoc. 1998;129(7):871-7.
18. Caufield PW, Cutter GR, Dasanayake AP. Initial acquisition of mutans streptococci by infants: evidence for a discret window of infectivity. J Dent Res. 1993;72(1):37-45. doi: 10.1177/00220345930720010501.
19. Köhler B, Andreén I. Influence of caries-preventive measures in mothers on cariogenic bacteria and caries experience in their children. Archs Oral Biol. 1994;39(10):907-11. doi: 10.1016/0003-9969(94)90023-X.
20. Navarro MFL, Côrtes DF. Avaliação e tratamento do paciente com relação ao risco de cárie. Maxi-Odonto: Dentística. 1995;1(4):1- 38.
21. Narvai PC. Saúde bucal da gestante. RGO - Rev Gaúcha Odontol. 1984;32(3):243-9.
22. Abdalla AE. Cuidados com a gestante. J Am Dent Assoc Brasil. 1999;2(4):78-80. 23. Feldens EG, Feldens CA, Kramer PF, Claas BM, Marcon CC. A percepção dos médicos obstetras a respeito da saúde bucal da gestante. Pesq Bras Odontoped Clin Integr. 2005;5(1):41-6.
24. Gaffield ML, Gilbert BJC, Malvitz, DM, Romaguera R. Oral health during pregnancy. J Am Dent Assoc. 2001;132(17):1009-16.
25. Batistella FID, Imparato JCP, Raggio DP, Carvalho AS. Conhecimentos da gestante sobre saúde bucal. RGO - Rev Gaúcha Odontol. 2006;54(1):67-73.
26. Morandini AC, Vidotti BA. Odontologia para gestantes sem mitos. Pet Informa. 2004;17(1/2):61.
27. Tollara MN, Corrêa MSNP, Bõnecker MJS, Carvalho GD. Aleitamento natural. In: Corrêa MSNP. Odontologia na 1ª infância. São Paulo: Editora Santos; 1998. p.71-86.
28. Antunes LS, Antunes LAA, Corvino MPF, Maia LC. Amamentação natural como fonte de prevenção em saúde. Ciênc Saúde Coletiva. 2008;13(1):103-9. doi: 10.1590/S1413- 81232008000100015.
 Endereço para correspondência:
Endereço para correspondência:
SHC SALES-PERES
e-mail: shcperes@usp.br
Received on: 31/8/2009
Final version resubmitted on: 31/8/2009
Approved on: 7/5/2010
