










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.61 no.4 Porto Alegre Out./Dez. 2013
CLÍNICO / CLINICAL
Risks and complications in surgically assisted rapid maxillary expansion
Riscos e intercorrências na expansão rápida de maxila cirurgicamente assistida
Kelly dos Anjos MELOI; Sarah Teixeira COSTAI; Raquel Simões Silva STEHLINGI; Eduardo Stehling URBANOI
I Universidade Federal de Juiz de Fora, Faculdade de Odontologia. Rua José Lourenço Kelmer, s/n., Campus Universitário, São Pedro, 36036-900, Juiz de Fora, MG, Brasil.
ABSTRACT
Rapid maxillary expansion is generally contra-indicated in patients with incomplete bone formation, and is only used as an alternative in those with advanced skeletal age. In young patients, Haas and Hyrax expanders are indicated and are chosen according to requirements. In adults, an application of orthodontic-surgical techniques allows correction of transversal and other deformities, offering very acceptable and predictable results while increasing the maxillary arch perimeter to correct the posterior crossbite. However, there have been reports of related complications, such as significant hemorrhage, gingival recession, root resorption, devitalization of teeth, sinus infection, oculomotor nerve paralysis, and orbital compartment syndrome. Maxillofacial surgeons should be aware of such possible complications and that patients are fully informed. This study reviews available literature and presents a case of surgical treatment, with the aim of reviewing complications occurring during the orthognathic surgery for opening the midpalatal suture.
Indexing terms: Complications. Orthognathic surgery. Palatal expansion technique.
RESUMO
A expansão rápida da maxila cirurgicamente assistida é contra-indicada, na maioria dos casos, em pacientes com maturidade óssea incompleta, sendo indicada apenas àqueles pacientes com idade óssea avançada. A cirurgia aumenta o perímetro do arco maxilar, corrigindo as mordidas cruzadas. Nos pacientes jovens, são usados aparelhos expansores do tipo Haas e Hyrax, escolhidos de acordo com as necessidades de cada paciente. Nos adultos, as aplicações das técnicas ortodôntico-cirúrgicas, possibilitam a correção de deformidades transversais, com uma previsibilidade bastante aceitável e, com poucos relatos de complicações. Complicações como hemorragia significativa , recessão gengival, reabsorção radicular, desvitalização de dentes, sinusite, paralisia do nervo oculomotor, e síndrome do compartimento orbital foram descritas. Cirurgiões maxilofaciais devem estar cientes de tais complicações e que os pacientes devem estar plenamente informados. Este estudo, revisa a literatura disponível e apresenta um caso de tratamento cirúrgico, com a finalidade de, expor as possíveis complicações da cirurgia ortognática.
Termos de indexação: Complicações. Cirurgia ortognática. Técnica de expansão palatina.
INTRODUCTION
Rapid maxillary expansion (RME) is often used to improve orthodontic results by increasing the maxillary transverse dimension in young patients1-6. The force exerted by expanders (Haas-type and Hyrax) opens the midpalatal suture5-6. Such appliances are most commonly used in children, but fail in teenagers and adults, thus RME is less effective in those ages2,4,6.
Some studies have reported the risks and effects of RME in periodontal, skeletal, dental, ducts, orbital and nasal changes in patients after this orthognathic surgery 1-2,4-8.
Surgically assisted rapid palatal expansion is an alternative to achieve effective maxillary expansion in skeletally mature patients1,3-4. However, some authors have reported that this technique has low morbidity1,3.
Surgical or orthodontic techniques increase maxillary arch perimeter to correct posterior crossbite to prove space for a crowded maxillary and others purposes1,4-5,7-8.
Pre-operative planning includes soft tissue evaluation, and the type of presenting maxillary transverse deficiency and buccal lingual inclination of the posterior teeth8. The patient´s age is considered as the fundamental basis for distinguishing either the use of rapid maxillary expansion or surgically assisted rapid palatal expansion4,8. This study aims to review available literature, and to present a case of rapid maxillary expansion (RME).
CASE REPORT
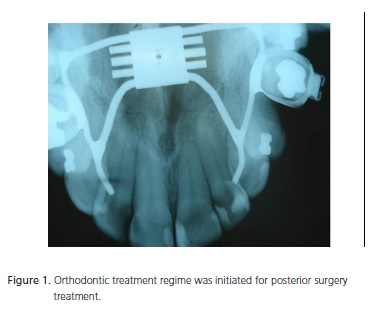
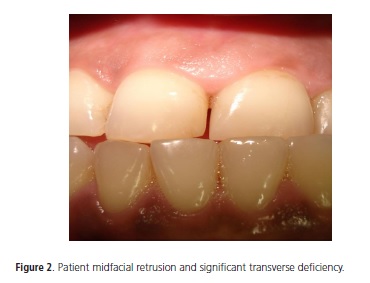
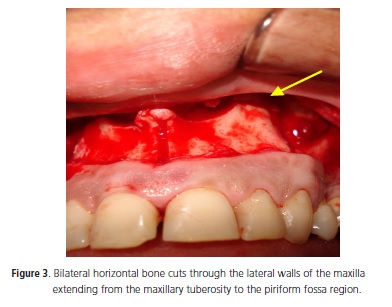
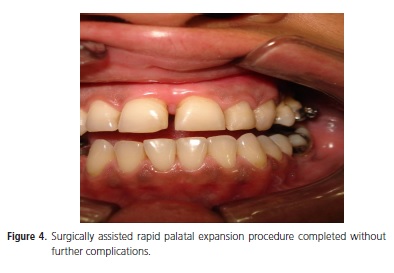
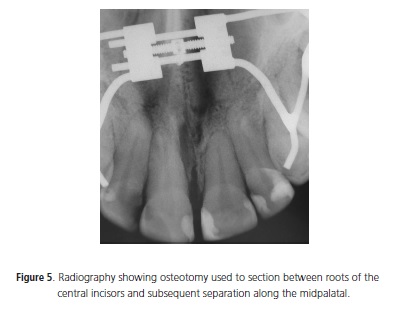
The patient is a 38-year-old female with midfacial retrusion and significant transverse deficiency (Figure 2). Lateral cephalometric analysis showed abnormal values. An orthodontic treatment regime was initiated for posterior surgery treatment (Figure 1). The patient was taken to the Hospital ater to undergo surgically assisted rapid palatal expansion under general anesthesia using naso-tracheal intubation. A saw was used in the initial procedure to make horizontal bone cuts in both sides through the lateral walls of the maxilla, from the maxillary tuberosity to the piriform fossa region. The medial wall of the maxillary sinus was not included in the cut, and a pterygomaxillary separation was not performed. A diamond disc was used to make a cut through the labial cortex directly between the roots of the maxillary central incisors. A fine osteotome was then used to section between the roots of the central incisors and this was continued along the midpalatal suture to the posterior end of the hard palate without perforating the palatal mucosa (Figure 5). An analysis of the orthodontic expansion required between the central incisors was made before and after the procedure. At this point the expander was activated by turning the expansion screw 10 one-quarter turns (2.5 mm). In this present case, bleeding occurred in the tuber of the maxilla, (due to the proximity of the pterygoid venous plexus), and the nasal cavity, controlled respectively by the use of a fibrin sponge and nasal packing. The surgically assisted rapid palatal expansion procedure continued without further complications (Figure 4).Homeostasis was ensured and sutures put in place.
This work was analyzed and approved by the Ethic Committee of Federal University of Juiz de Fora (protocol number 369/2008).
DISCUSSION
The objective of this study was to conduct a review ofa surgically assisted RME,describe a clinical case including the closure of sutures, and discuss complications associated with this technique.
The choice of using either RME or surgicallyassisted RMEis directly related to the closure of sutures and theage of the patient. Surgically-assisted rapid palatal expansion (RPE) is indicated in patients over 16 years old1,2,9,8 with an upper age limit of 25 years1-2,9-10. Some studies have specified the appropriate upper age limit to be 25 years in men, and 20 years for women1-2,11. This surgery is recommended after the second decade of life1-2,12. Research also suggests that orthognathic maxillary expansion is successful in patients younger than 12, and that corticotomies are essential in patients over 14 years1-2,13.
Many studies have reported the connection between the closure of sutures and the patient's age, and type of expansion14-17. For example, Latham & Burston14 state that, in general, after about 2 or 3 years of age the skull sutures function primarily as sites of bone union, although localized remodeling seems to be a continuing process. In agreement with this assumption, Sicher15 declares that the closure of sutures usually starts in the mid-30s at the posterior part of the median palatine suture. Person16 added that there is evidence of bony ossification at 17 years old. However, Latham & Burston9 report that there is no evidence of synostosis in the same suture by the age of 18 years, Baurind & Korn17 reposted that the maxillary sutures close at approximately 14-15 years of age in females and at approximately 15-16 years of age in males. These outcomes suggest that, in spite of the majority of facial sutures appearing to be open on the surface of old skulls, some degree of union may be present in the substance of the suture18.
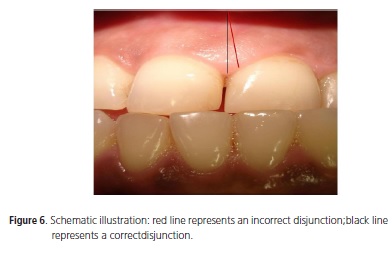
Although surgically assisted rapid palatal expansion procedures have been reported to have low morbidity, some complications have been described1-2. Several articles have described complications associated with maxillary expansion; for example, significant hemorrhaging and subsequent gingival recession1-2,19. Root resorption has also been reported1-2,13,20. Injuries to the branches of the maxillary nerve, infection, pain, devitalization of the teeth, and altered pulpal blood flow have also been reported1-2,13,20. However, if performed under the correct protocolpulpal blood flowis not affected20. Other complications such as periodontal breakdown1,6,21, sinus infection1,22, alar base flaring1,9,22, relapse, and unilateral expansion1,22 have also been reported. In the case of unilateral expansion it is necessary to wait for consolidation to re-evaluate anyesthetic defect and evaluate the possibility of further surgical intervention (Figure 6).
Breakage, stripping, or locking of the appliance screw1,22, and its loosening and impingement onto palatal soft tissue1,6,23 have also been related as possible complications. The incidence of frank aseptic tissue is about 1.8%, and at least 5% of the patients suffer some type of palatal ulceration6,24. Hemorrhage can also be life-threatening1-2,22 requiring blood transfusions and additional hospital stay1,11, or present as a minor posterior epistaxis1-2,7,22. Life threatening epistaxis caused by cerebrovascular accident, skull base fracture with reversible oculomotor nerve paralysis, and orbital compartment syndrome have been described previously6,25, and the latter has been described as a possible cause of permanent blindness4. Undesirable fractures of the maxillary articulation, and asymmetric fractures of the inderdental bone between the central incisors, are commonly seen1-2,21-22. Glassman et al.1-2,26 have also described extrusion of the teeth attached to the gadget. In the particular technique described by Glassman, and in other conservative techniques, the fracture of the alveolar process is recommended26.
It is possible to observe an increase in stress on the skull base, particularly on the optic foramen, if the procedure is performed without separation1,22,27. Other complications include bilateral lingual anesthesia1-2,22,28, nasopalatine canal cysts1,22,29, increasednasal volume and decreased nasal resistance29, a decreased craniocervical angle and increased cervical lordosis angle5,7, and a positive effect on the hearing levels in persons with conductive hearing loss5,7.
Some effects noted on the skull include a maxillary slight, an increase of anterior facial height30 and maxillary and nasal width1-2,5-6, buccal bone plate thickness reduction, increased lingual bone plate thickness (mostly in the posterior teeth)7, and a reduction as a whole of both buccal bone thickness and buccal marginal bone levels of the posterior teeth7-8,30. No significant effects have been seen in pharyngeal airway dimensions or the hyoid position in adults8,28-29.
CONCLUSION
Surgically assisted rapid palatal expansion is a widely used procedure for the correction of transverse maxillary deficiency in skeletally mature patients. However, no definitive way exists that combines successful outcomes from various surgical procedures, and that ensures adequate mobilization in combination with the most conservative procedure. Therefore, it is considered necessary that surgeons are fully informed of all possible complications, and that such information is transmitted to prospective patients.
Collaborators
ES URBANO, was responsible for the surgical procedure described in the item case report, as well as supervision and collection of references and writing up the paper. KA MELO was responsible for the of the monitoring of the case, collection of bibliographic references and also has participated in the preparation of the scientific article. ST Costa, was responsible for monitoring the case, collection of bibliographic references, and also has participated in the preparation of the scientific article. RSS STEHLING, responsible for the surgical procedure described in the item case report, as well as supervision and collection of references and writing up the paper.
REFERENCES
1. Suri L, Taneja P. Surgically assisted rapid palatal expansion: a literature review. Am J Orthod Dentofacial Orthop. 2008;133(2):290-302. doi: 10.1016/j.ajodo.2007.01.021. [ Links ]
2. Atac A, Karasu HA, Aytac D. Surgically assisted rapid maxillary expansion compared with orthopedic rapid maxillary expansion. Angle Orthod. 2006;76(3):353-9.
3. Lanigan DT, Mintz SM. Complications of surgically assisted rapid palatal expansion: review of the literature and report of a case. J Oral Maxillofac Surg. 2002;60(1):104-10. doi: 10.1053/ joms.2002.29087.
4. Babacan H, Sokucub O, Doruka C, Ay S. Rapid maxillary expansion and surgically assisted rapid maxillary expansin effects on nasal volume. Angle Orthod. 2006;76(1):66-71.
5. Taspinar F, Uçuncu H, Bishara SE. Rapid maxillary expansion and conductive hearing loss. Angle Orthod. 2003;73(6):409-14.
6. Chung CH, Font B. Skeletal and dental changes in the sagittal, vertical and transverse dimension after rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2004;126(5):569-75. doi: 10.1016/j.ajodo.2003.10.035.
7. Tecco S, Festa F, Tete S, Longhi V, D'Attilio M. Changes in head posture after rapid maxillary expansion in mouth-breathing girls:-a controlled study. Angle Orthod. 2005;175(2):171-6.
8. Garib DG, Henriques JFC, Janson G, Freitas MR, Fernandes Ay. Periodontal effects of rapid maxillary expansion with tooth-tissue-borne and tooth-borne expanders: a computed tomography evaluation. Am J Orthod Dentofacial Orthop. 2006;129(6):749-58. doi: 10.1016/j.ajodo.2006.02.021.
9. Epker BN, Wolford LM. Transverse maxillary deficiency dentofacial deformities: integrated orthodontic and surgical correction. St Louis: Mosby; 1980.
10. Timms DJ, Vero D. The relationship of rapid maxillary expansion to surgery with special reference to midpalatal synostosis. Br J Oral Surg. 1981;19(3):180-96.
11. Alpern MC, Yurosko JJ. Rapid palatal expansion in adults with and without surgery. Angle Orthod. 1987;57(3):245-63.
12. Mossaz CF, Byloff FK, Richter M. Unilateral and bilateral corticotomies for correction of maxillary transverse discrepancies. Eur J Orthod. 1992;14(2):110-6. doi: 10.1093/ejo/14.2.110.
13. Mommaerts MY. Transpalatal distraction as a method of maxillary expansion. Br J Oral Maxillofac Surg. 1999;37(4):268- 72. doi: 10.1054/bjom.1999.0127.
14. Latham RA, Burston WR. The postnatal pattern of growth at sutures of the human skull. Dent Pract. 1966;17(2):61-7.
15. Sicher H. Oral anatomy. 4th ed. St.Louis: Mosby Co.; 1965.
16. Persson M. Structure and growth of facial sutures. Odontol Rev. 1973;24(6):1-146.
17. Baumrind S, Korn EL. Transverse development of human jaws between the ages of 8.5 and 15.5 years, studied longitudinally with the use of implant. J Dent Res. 1990;69(6):1298-306. doi: 10.1177/00220345900690061501.
18. Scott JH. Dentofacial development and growth. Oxford: Pergamon Press; 1967.
19. Carmen M, Marcella P, Giuseppe C, Roberto A. Periodontal evaluation in patients undergoing maxillary expansion. J Craniofac Surg. 2000;11(5):491-4.
20. Harada K, Sato M, Omura K. Blood-flow change and recovery of sensibility in the maxillary dental pulp during and after maxillary distraction: a pilot study. Oral Surg Oral Med Oral Patho Oral Radiol Endod. 2004;98(5):528-32. doi: 10.1016/j. tripleo.2004.02.079
21. Mehra P, Cottrell DA, Caiazzo A, Lincoln R. Life-threatening, delayed epistaxis after surgically assisted rapid palatal expansion: a case report. J Oral Maxillofac Surg. 1999;57(2):201-4. doi: 10.1016/S0278-2391(99)90241-0.
22. Schimming R, Feller KU, Herzmann K, Eckelt U. Surgical and orthodontic rapid palatal expansion in adults using Glassman's technique: retrospective study. Br J Oral Maxillofac Surg. 2000;38(1):66-9. doi: 10.1054/bjom.1999.0274.
23. Lehman JA, Haas AJ. Surgical-orthodontic correction of transverse maxillary deficiency. Dent Clin North Am. 1990;34:385-95.
24. Bays RA, Greco JM. Surgically assisted rapid palatal expansion: An outpatient technique with long-term stability. J Oral Maxillofac Surg. 1992;50(2):110-3. doi: 10.1016/0278-2391(92)90352-Z.
25. Holberg C, Steinhäuser S, Rudzki I. Surgically assisted rapid maxillary expansion: midfacial and cranial stress distribution. Am J Orthod Dentofacial Orthop. 2007;132(6):776-82. doi: 10.1016/j.ajodo.2005.12.036.
26. Glassman AS, Nahigian SJ, Medway JM, Aronowitz HI. Conservative surgical orthodontic adult rapid palatal expansion:sixteen cases. Am J Orthod. 1984;86(3):207-13. doi: 10.1016/0002-9416(84)90372-5.
27. Palasia J, Ngan P, Martin C, Razmus T. Use of conventional tomography to evaluate changes in the nasal cavity with rapid palatal expansion. Am J Orthod Dentofacial Orthop. 2007;132(4):458-66. doi: 10.1016/j.ajodo.2005.10.025.
28. Rungcharassaeng K, Caruso JM, Kan JY, Kim J, Taylor G. Factors affecting buccal bone changes of maxillary posterior teeth after rapid maxillary expansion. Am J Orthod Dentofacial Orthop. 2007;132(4):428.e1-8. doi:
29. Malkoç S, Uşümez S, Işeri H. Long-term effects of symphyseal distraction and rapid maxillary expansion on pharyngeal airway dimensions, tongue, and hyoid position. Am J Orthod Dentofacial Orthop. 2007;132(6):769-75. doi: 10.1016/j. ajodo.2005.11.044.
30. Lai KP, Almeida MHC, Almeida RC, Ferrer KJN, Bianchini FLC. Disjunção rápida da maxila em mordida cruzada. RGO - Rev Gaúcha Odontol. 2003;51(4):285-8.
 Endereço para correspondência:
Endereço para correspondência:
KA MELO
e-mail: kellyanjosm@gmail.com
Received on: 17/9/2009
Final version resubmitted on: 2/8/2010
Approved on: 29/9/2010
