










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.62 no.2 Porto Alegre Abr. 2014
ORIGINAL / ORIGINAL
Relative area measurement of maxillary sinus by computed tomography
Mensuração da área relativa do seio maxilar por meio da tomografia computadorizada
Ronaldo Andrade Figueiredo de OLIVEIRAI; Maria Cristina PEDRAZINII; Thomaz WASSALLI
I Faculdade São Leopoldo Mandic, Curso de Odontologia, Programa de Pós-Graduação em Implantodontia
ABSTRACT
Objective
To evaluate the relative area of the maxillary sinus in edentulous posterior maxilla with regard to linear area, bone septa and sinus pathologies..
Methods
A retrospective longitudinal study was conducted of tomographic exams in 60 individuals between 35 and 75 years of age, with the inclusion criteria being the uni- or bilateral edentulous posterior maxilla. Measurements were taken by the program in 101 maxillary sinuses. The horizontal and vertical measurements of each sinus were multiplied and resulted in a linear area in mm2.
Results
Of the 101 maxillary sinuses evaluated, 14 presented sinus pathologies (13.86%) and 22 (21.78%) with bone septa. The mean mesio distal distance was 38.4 mm (p ≤ 0.05), mean height 34. 5 mm (p ≤ 0.05) and mean linear area of 1335.88 mm² (p = 0.05). The Student's-t and analysis of variance (ANOVA) tests were applied for statistical analysis There were no statistically significant difference in the height and width of the edentulous maxillary sinuses between genders, but there was a variation in the linear area and the finding of the presence of bone septa and sinus pathologies.
Conclusion
The conclusion of this study corroborates those of previous study about the need for imaging exams with the purpose of obtaining information about the dimensions of the maxillary sinus, as guidance with regard to the quantity of graft material, choice of donor region, and presence of septa. These data serve as guidance in the sinus lift technique and the presence of sinus pathologies, which involve treatment before bone graft surgeries.
Indexing terms: Maxillary sinus. Sinusitis. Tomography, X-ray computed.
RESUMO
Objetivo
Avaliar a área relativa do seio maxilar em maxila desdentada posterior quanto à área linear, presença de septos ósseos e sinusopatias.
Métodos
Foi realizado um estudo longitudinal retrospectivo de exames tomográficos em 60 indivíduos entre 35 e 75 anos e como critério de inclusão, a maxila posterior desdentada uni ou bilateralmente. As medições foram realizadas pelo programa em 101 seios maxilares. As medidas horizontais e verticais de cada seio foram multiplicadas e resultaram em área linear em mm².
Resultados
Dos 101 seios maxilares avaliados, 14 apresentaram sinusopatias (13,86%) e 22 (21,78%) com septos ósseos. A média mesio distal foi de 38,4 mm (p ≤ 0,05), a altura média de 34, 5 mm (p ≤ 0,05) e área linear média de 1335,88 mm² (p = 0,05). Foi aplicado o teste t de Student e análise de variância (ANOVA) para análise estatística. Não houve diferenças estatísticas significantes na altura e largura dos seios maxilares desdentados entre os gêneros, mas houve uma variação da área linear bem como a constatação da presença de septos ósseos e sinusopatias.
Conclusão
A conclusão deste trabalho corrobora com estudos anteriores sobre a necessidade dos exames por imagem com a finalidade de obter informações quanto as dimensões do seio maxilar norteando a quantidade de material de enxertia bem como a escolha da região doadora, a presença de septos orientando a técnica de levantamento de seio e a presença de sinusopatias que implica em tratamento prévio à cirurgia de enxertos.
Termos de indexação: Seio maxilar. Sinusite. Tomografia computadorizada por raios X.
INTRODUCTION
The rehabilitation of completely or partially edentulous individuals by means of dental Implants has proved to be a promising resource in Dentistry. However, success depends on a minimum quantity of bone tissue being available for the placement of osseointegratable implants. This minimum bone condition is frequently absent, due to the rapid and continuous process of edentulous alveolar bone resorption, leading to different levels of atrophy. In these cases, reconstruction of the area to be rehabilitated becomes mandatory1-2.
Bone reconstruction of the maxillae must be preceded by planning of the case, with information about the medical history of the individual, clinical evaluation of the oral cavity, requisition of imaging exams for analysis of the maxillary sinus volume, presence of septa and/ or sinus infections. This set of information will guide the decision about when and how to perform the surgical reconstruction procedure3-4.
Pneumatization of the maxillary sinus with change in volume occurs due to the loss of teeth, and is an indication for performing bone reconstruction by means of bone graft. Depending on this volume, the donor area is selected, and the decision is made about whether or not to use biomaterials associated with autogenous bone5-6.
Bone graft in the maxillary sinus was developed from modification of the Caldwell-Luc technique, with full elevation of the whole sinus membrane, in a procedure known as "sinus lift"7-9. The procedure is simple, however, it must be carefully performed, in order to avoid complications such as perforation of the sinus membrane, or post-surgical infections. Internal configurations of the maxillary sinus, such as the presence of bone septa may cause problems limiting osteotomy of the access window through the lateral wall, and facilitate perforation of the sinus membrane10-11.
Considering that sinus septa are present in 39% of maxillary sinuses, and that this fact may cause problems during opening of the lateral window in grafts, the surgeon must always request a computed tomograph before surgery; this is now a consensus12-15.
The anatomy of the maxillary sinus may be investigated with the use of panoramic radiographs and/or computed tomographs. Depending on the findings as regards septa, the design of the lateral window must be modified16, in order to prevent intercurrences in the procedure.
With regard to sinus pathologies, chronic sinusitis or cysts are factors that must be controlled before the procedure in order to avoid later infection with loss of the graft and/or osseointegration of the implant not occurring17-19.
The maxillary sinuses may be affected by pathologies of traumatic origin, neoplasias and particularly by infections arising in the nasal or oral cavities with dental structures and their periodontium. When infection is present in the sinus cavity, it is denominated sinusitis, and this process may obstruct the sinus ostium, making it difficult for the seromucous secretion to leave the sinus cavity. Sinus infections may be of odontogenic origin when they are triggered by bucco sinus fistulas, endodontic or periodontal infections, by the presence of dental cysts or tumors. Non odontogenic sinus infections may arise from anatomic obstructive nasal conditions, such as deviation of the nasal septum and alterations in the position and size of the sinus ostium, concha bullosaand/or hypertrophic bulbous projection, due to allergic conditions, which may also cause hypertrophy of the adenoids and nasal mucosa20.
In view of the problem studied, the aim of this study was to perform an analysis of the area relative to the maxillary sinuses; that is, the height and width of the sinus cavity, by means of Computed Tomography NewTom 3G® (Mod. QR-DVT9000-QRSRL™, Verona, Italy) with volumetric acquisition and 3D reconstruction specifically of three aspects: difference in linear measurements between genders; presence of bone septa, and diagnosis of sinus pathologies, in order to equate the possible obstacles existent to performing the bone graft techniques, such as anatomical, pathological and linear variations.
METHODS
Ethical Aspects
The research was approved by the Research Ethics Committee of the School of Dentistry, São Leopoldo Mandic, Protocol No. 07/148 and the retrospective longitudinal study was conducted by means of a survey of the documents in the archives of the Dental Radiology Institute - IRO (Instituto Radiológico Odontológico - IRO) in Campinas (SP), Brazil.
An evaluation was made of 60 pre-operative computed tomographs to record the linear measurements and extension of pneumatization of the maxillary sinus, presence or absence of sinus pathologies and bone septa in individuals of the male and female genders between 35 and 75 years of age. The inclusion criteria were: completely, uni- or bilaterally edentulous posterior maxillae, and in conditions to be submitted to bone graft surgery with maxillary sinus lift and later rehabilitation with dental implants.
The computed tomographs were performed with the Cone Beam Computed Tomograph - NewTom 3G® (Mod. QR-DVT9000-QRSRL™, Verona, Italy) with low exposure to radiation and high resolution results. The operating parameters were 110KVp and variable MAs (calculated by the size of the individual), 1 mm thick cuts, acquisition time 36 seconds and cone beam opening of 9 inches (removal of image).
To obtain the computed tomographs, the individual was placed lying on his/her back, and the image of the maxilla was obtained with the individual's head placed in the Reid's Base Line position (Orbital-Meatal line) perpendicular to the work table and median sagittal plane parallel to it.
From the computed tomography images with the panoramic cut chosen in the most central region of the arch, the quantitative linear evaluation of the maxillary sinus was obtained by two lines: one vertical (V) and the other horizontal (H). The vertical line was dimensioned from the lowest point of the sinus floor to its highest point, at the margin of the orbital floor and the horizontal line demarcated at the largest mesio distal extension of the sinus cavity; that is, from the medial limit wall with the nasal cavity up to the distal wall next to the tuberosity of the maxilla (Figure 1).
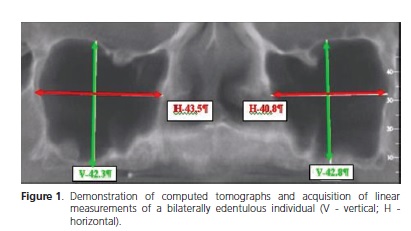
The vertical and horizontal measurements were taken with the software program of the tomograph itself (QRNNT version 2.02) and were multiplied to obtain an area in square millimeters denominated S1 or S2 (area/ mm²) = V (mm) x H (mm), with S1 being - area of the right or left maxillary sinus (unilaterally edentulous) or of the right maxillary sinus (bilaterally edentulous) and S2 - area of the left maxillary sinus (bilaterally edentulous).
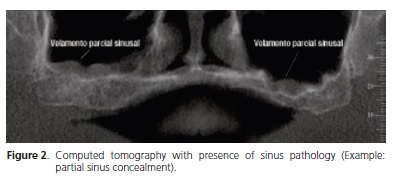
The presence of sinus pathologies such as thickening of the mucosa, retention cysts and opacification or radiolucency of the sinus cavity were evaluated by a single examiner using one single negatoscope apparatus (Figure 2).
With regard to bone septa, these were scored by evaluating their presence in the maxillary sinus floor by panoramic reconstruction of the computed tomographs, and confirmed in longitudinal cuts (Figure 3). 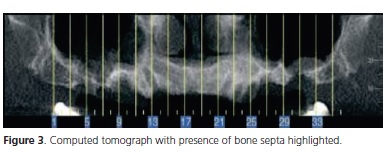
Analysis of Variance (ANOVA) and Student's-t tests were applied to the evaluations of the linear measurements and areas of the sinuses using the SAS statistical software program with a 5% level of significance.
The differences in height, width and areas obtained in the measurements of the sinuses were compared by dividing the groups by gender, and by the unilateral or bilateral presence of edentulous area.
RESULTS
Of the 24 individuals of the male gender, 8 were unilaterally and 16 bilaterally edentulous, totaling 40 maxillary sinuses. Eight presented sinus pathologies and 15 bone septa. Of the 36 individuals of the female gender, 11 were unilaterally and 25 bilaterally edentulous, totaling 61 maxillary sinuses. Six presented sinus pathologies and 7 bone septa.
Of the total of 101 maxillary sinuses analyzed, 14 (13.86%) sinuses presented sinus pathologies and 22 (21.78%) bone septa.
As regards sinus height and width, the mean value between genders was 38.4 mm in width and 34.52 mm in height. As regards the relative area of the sinuses, the mean observed in the male gender was 1367.53 mm2 and in the female gender it was 1315.13 mm2. The total mean relative area of the edentulous maxillary sinuses was 1335.88 mm2.
Mean height and width values of each gender considering the location of the edentulous sinus were submitted to
Analysis of Variance (ANOVA) and were shown to differ between them by p ≤ 0.05. Analysis of Variance of the areas (S1) did not differ between them with p > 0.05. The areas (S2) submitted to the Student's-t test considering gender and the edentulous maxillary sinus, did not differ between them with p> 0.05.
DISCUSSION
As success in Implant Dentistry may only be achieved if a meticulous study has been performed, all the alternatives diagnosed must be used in order to know the areas that will be operated, or submitted to graft procedures, or only to the placement of implants. Evaluation of the bone margins may be performed, in addition to clinical exam, by means of intraoral radiographs, panoramic radiographs, computed tomography and magnetic resonance (MR), with the use of computed tomography being a reliable and safe alternative for this type of evaluation.
Cone Beam technology, in addition to providing quality images, provides data about the quantity of remaining bone, anatomic structures involved and the characteristics of possible donor regions21. It minimizes the time of patient exposure during the procedure, diminishes artifacts that make it difficult to interpret the images, and enables the capture of 30 or more cuts with a thickness of 0.5 and 1 mm. Furthermore, tomography is the only means of observing the bone thicknesses available during the selection of the size and type of implant22-23.
In view of these affirmations, the use of computed tomography is recommendable both in complex and routine cases, due to its capacity to reconstruct a complete tridimensional model of the maxilla and mandible, with precise definition of the structure of the maxilla and anatomic location of critical structures24.
In view of this diagnostic alternative, there is no justification for an intervention in the maxillary sinus performed "in the dark". Detailed knowledge about the morphology of this maxillary region is clinically relevant in order to reduce complications when sinus lift surgery is performed25-26.
The sinus cavity is complex, and may be divided by bone septa which are cortical bone folds invaginated into the sinus. These septa may be complete (1 to 10%) or incomplete, and this condition may be visualized in imaging exams.
Septa are present in 13 to 35.3% of maxillary sinuses27, numbers that are in agreement with those found in this study, in which 22% of sinuses with the presence of septa were observed.
The size of the septum may range from 2.5 to 23.7 mm in mean length, and there are reports of a higher prevalence of septa in atrophic than in non atrophic edentulous areas. Maxillary sinus lift in the presence of a septum requires a modification in the design of the lateral window, in order to prevent intercurrences in the procedure16, and the success rate of sinus floor lift is clearly related to the presence of bone septa15.
Another fact that must be observed in maxillary sinuses is the presence of absence of infectious pathologies that generate serious complications. These pathologies, denominated sinusitis, may be acute or chronic and must be diagnosed from the individual's history and clinical and radiographic exams. The symptoms are not specific and resemble those of a common cold or allergic rhinitis. The cause of sinusitis is bacterial inhalation associated with edema of the mucosa lining the sinus, which makes it difficult for drainage of the secretion to occur, and facilitates bacterial colonization. The individual's history associated with acute sinusitis includes unilateral headache and pain in the area of the maxilla. The teeth, even when they are vital, may be painful and sensitive. Chronic sinusitis presents headache, edema of the face and thick purulent hypersecretion, generally with a yellowish or greenish color.
The maxillary sinuses may be affected by pathologies of traumatic, neoplastic and infectious origin. The infectious types are more frequent due to the proximity of the nasal cavity and dental and periodontal structures of the maxilla. Because of this proximity, these infections may be classified as being of odontogenic origin (10% of cases with minimal clinical symptoms) and non odontogenic, such as acute or chronic sinusitis. Sinus infections may be of odontogenic origin are generally unilateral, and are triggered by buco sinus fistulas, endodontic or periodontal infections, and also by the presence of dental cysts or tumors. The non odontogenic type may be uni- or bilateral and arise from obstructive nasal conditions, such as deviation of the nasal septum, concha bullosa and/or hypertrophic concha, hypertrophy of the adenoids and nasal mucosa, alteration in the position and size of the sinus ostium, and allergic diseases such as sinusitis may cause obstruction of the ostium. Traumatisms resulting from the Caldwell-Luc techniques sometimes obstruct the main ostium, leading to an accumulation of secretion inside the cavity and its consequent expansion, accompanied by expansion of the adjacent bone tissue. This phenomenon denominated mucocele is more common in the paranasal and frontal sinuses, and rare in the maxillary and sphenoid sinuses. Non secretory or pseudocysts originate from the accumulation of inflammatory exudates below the periosteum, resulting from sinus infections; whereas retention or secretory cysts originate from obstruction of the duct of a seromucous gland; that is to say, because of the non drainage of the secretion, the duct and gland dilate giving rise to a cystic structure20.
Irrespective of the cause of the sinus pathology, which in this study presented in 14% of the sinuses investigated, it should be diagnosed and treated before any invasive procedure is performed.
With regard to sinus topography - very important in the study of the surgical technique to be used and calculation of the bone volume to be grafted - researchers1,27 have analyzed the topographical anatomy during surgeries as well as radiographically, and found mean heights of 3.5 cm, widths of 2.5 cm and depths of 3.0 cm in sinuses, which corroborate the results with reference to height and mesio distal extension found in the present study. The dimensions of the maxillary sinuses are variable and depend on factors such as age, gender, ethnicity, and individual conditions, quite often varying when one side is compared with the other in the same individual. In adults, the size remains stationary in normal condition, however, after permanent tooth extractions, the size of maxillary sinuses increases by the occupation of root spaces. This pneumatization may be greater after extraction of all the maxillary teeth, or when partial a extractions occur in the first decades of life.
With this increase in sinus volume, tomographic exams help to define the quantity of bone graft to be requested for sinus lift and later implant placement. A12 mm increase in height requires 1.7 ± 0.9 cc; and for 17 mm the volume required is 3.6 ± 1.5 cc, therefore, this knowledge of the receptor area is essential for making decisions on the choice of donor area; extension of the surgical intervention, and even deciding about the type of graft material to be used, because depending on the extension of the receptor area, it may be necessary to complement the graft with the use of biomaterials6.
CONCLUSION
The study about the relative analysis of the maxillary sinus allowed one to conclude that detailed preoperative evaluation of the maxillary sinus is important and there is consensus in the literature about this affirmation.
With the use of computed tomography it is possible to calculate the quantity of material to be grafted in the sinus, thereby diminishing the morbidity of the patient operated, with regard to donor areas. Finding the presence of septa and/or sinus pathologies guides the dental surgeon with regard to the best procedure to adopt for the prevention of problems, so that the intervention, and the best time for the surgery may be planned.
REFERENCES
1. Ayala JP, Gutierrez GA. Tratamento da maloclusão de Classe II. In: Interlandi S. Ortodontia bases para a iniciação. 4ª ed. São Paulo: Artes Médicas; 1999. p. 329-76. [ Links ]
2. Rey SC, Fazzi R, Birman EG. Principais alterações craniofaciais em portadores da Síndrome de Down. Rev Fac Odontol FZL. 1991;3(1):59-64.
3. Benatti AM, Campos MTGR, Zangilorami TR, Oliveira MCS, Casarin S. Diagnóstico pré-natal: anomalias cromossômicas: Síndrome de Down. In: Manual Projeto Down. São Paulo: Centro de informações e Pesquisa da Síndrome de Down; 1994.
4. Mustacchi Z, Peres S. Genética baseada em evidencias: síndromes e heranças. São Paulo: CID; 2000.
5. Desai SS, Fayetteville BDS. Down syndrome: a review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol. 1997;84(3):279-85. doi: 10.1016/S1079-2104(97)90343-7.
6. Coelho CRZ, Loevy HT. Aspectos odontológicos da Síndrome de Down. Ars Curandi Odontol. 1982;8(3):9-16.
7. Mustacchi Z, Rozone G. Síndrome de down: aspectos clínicos e odontológicos. São Paulo: CID; 1990.
8. Vaden JL. Orthodontic magic. Am J Orthod Dentofacial Orthop. 2000;117(5):584-5.
9. Sweard AF, Roche F, Sunderland S. The lateral cranial silhouette in mongolism. Aschs Oral Biol. 1961;85(4):653-8.
10. Suri S, Tompson BD, Cornfoot L. Cranial base, maxillary and mandibular morphology in Down syndrome. Angle Orthod. 2010;80(5):861-9. doi: 10.2319/111709-650.1.
11. Hsu BS. Comparisons of the five analytic reference lines of the horizontal lip position: their consistency and sensitivity. Am J Orthod Dentofac Orthop. 1993;104(4):355-60.
12. Epker BH, Stella JP, Fish LC. Dentofacial deformities. St. Louis: Mosby; 1995.
13. Frota - Pessoa O. Genética clínica. Rio de Janeiro: Francisco Alves; 1984.
14. Scavone Junior R, Zahn-Silva W, Vale-Corotti KM, Nahás ACR. Soft tissue profile in White Brazilian adults with normal occlusions and well-balanced faces. Angle Orthod. 2006;78(1):58-63. doi: 10.2319/103006-447.1.
15. Cohen MM, Winer R. Dental and facial characteristics in Down's Syndrome (Mongolism). J Dent Res. 1965;44(1):197-208.
16. Thompson CDA. The palate in down's syndrome. The Dental Assistant. 1976;45(10):6-20. doi: 10.1056/ NEJM196706292762603.
17. Fink GB, Madaus WK, Walker JF. A quantitative study of the face in Down's syndrome. Am J Orthod. 1975;67(5):540-53.
18. Shapiro S. Periodontal disease and Blood Citrate level in patients with trisomy 21. J Dent Res.1969;48():1231-3. doi: 10.1177/00220345690480062401.
19. Pozsonyi J, Gibson D, Zarfas DE. Skeletal maturation in mongolism. (Down's syndrome). J Pediatric. 1964;64(1):75-8. doi 10.1016/S0022-3476(64)80319-X.
20. Jesuino FA, Valladares-Neto J. Craniofacial morphological differences between Down syndrome and maxillary deficiency children. Eur J Orthod. 2013 Feb;35(1):124-30. doi: 10.1093/ ejo/cjr105.
21. Schlickmann ICA, Moro A, Dos Anjos A. Análise do perfil facial masculino adulto jovem, esteticamente agradável, em fotografias padronizadas: comparação da medição manual com a computadorizada. Dental Press Ortodon Ortop Facial. 2008; 13(6):98-107. doi: 10.1590/S1415-54192008000600012.
 Correspondence to:
Correspondence to:
RT BASTING
e-mail: rbasting@yahoo.com
Received on: 9/6/2010
Final version resubmitted on: 19/3/2012
Approved on: 2/4/2012
