










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.62 no.3 Porto Alegre Out./Dez. 2014
ORIGINAL / ORIGINAL
Bilateral mandibular dentigerous cysts: a case report
Cisto dentígero bilateral em mandíbula: relato de caso
Hécio Henrique Araújo de MORAISI; Tasiana Guedes de Souza DIASII; Ricardo José de Holanda VASCONCELLOSIII; Belmiro Cavalcanti do Egito VASCONCELOSIII; Auremir Rocha MELOIII; David Alencar GONDIMIII; Ricardo Wathson Feitosa de CARVALHOIII
I Universidade do Estado do Rio grande do Norte, Faculdade de Odontologia. Rua André Sales, 667, Paulo XI, 59300-000, Caicó, RN, Brasil
II Universidade do Estado do Rio Grande do Norte, Curso de Odontologia. Mossoró, RN, Brasil
III Universidade de Pernambuco, Faculdade de Odontologia. Camaragibe, PE, Brasil
ABSTRACT
Dentigerous cysts are frequently found in the maxilla. After radicular cysts, dentigerous cysts are those most commonly diagnosed, accounting for 20% of all jaw cysts. They are often asymptomatic and diagnosed incidentally during routine examinations. Clinical complications such as dental displacement, ectopic eruption, dental impaction, adjacent tooth root resorption, cortical expansion with facial asymmetry, paresthesia, pathological fracture, and even malignant transformation may occur. Despite these classical features, definitive diagnosis must always be based on histological examination. Most dentigerous cysts are solitary. The aim of this article is to report a case of bilateral mandibular dentigerous cysts in a non-syndromic patient and, through a literature review, present the available treatment modalities used successfully in this case.
Indexing terms: Dentigerous cyst. Mandible. Odontogenic cyst.
RESUMO
Os cistos são frequentemente encontrados nos maxilares. Depois dos cistos radiculares, os cistos dentígeros são os mais comumente diagnosticados, constituindo cerca de 20% de todos os cistos maxilo-mandibulares. Frequentemente apresentam-se de indolores, sendo achados em exames de rotina. Complicações clínicas como deslocamentos de dentes, erupções ectópicas, impacções dentárias, reabsorção das raízes dos dentes adjacentes, expansão da cortical gerando assimetria facial, parestesia e fratura patológica podem ocorrer advinda à presença dessa afecção. Apesar das características clássicas, o diagnóstico definitivo deve sempre ser baseado através do exame histopatológico. A maioria dos cistos dentígeros apresenta-se de forma solitária; múltiplos cistos são raros e geralmente são encontrados em pacientes sindrômicos. Este trabalho tem como objetivo relatar um caso de cistos dentígeros bilaterais em mandíbula no qual a descompressão teve fundamental importância para o sucesso do caso.
Termos de indexação: Cisto dentígero. Mandíbula. Cisto odontogênico.
INTRODUCTION
Dentigerous cysts are common lesions of the maxillomandibular complex. They are defined as pathologic epithelium-lined cavities that surround the crown of an unerupted tooth at the level of the cementoenamel junction. Although dentigerous cysts are highly prevalent, bilateral occurrence is rare and usually associated with syndromes or systemic diseases1, such as Maroteaux-Lamy syndrome2, cleidocranial dysplasia, and mucopolysaccharidosis1.
Dentigerous cysts are usually associated with an impacted tooth, most commonly a mandibular third molar; the maxillary canine is the second most commonly affected tooth. A dentigerous cyst associated with a maxillary central incisor in an 8-year-old child has been reported in the literature3. Approximately 75% of all dentigerous cysts are found in the mandible. One case of bilateral maxillary dentigerous cysts has been reported4; the authors stressed the importance of computed tomography for better treatment planning in the reported case.
These cysts are generally asymptomatic and diagnosed incidentally on routine radiographs or during etiological investigation of an unerupted tooth1. Signs and symptoms arise when the cyst expands enough to cause pain and bone expansion5. Although clinical complaints are valuable, histological examination is essential for definitive diagnosis1.
Histologically, dentigerous cysts may be inflamed or uninflamed. When uninflamed, they are characterized by a wall of relatively loose connective tissue, and an epithelial lining consisting of two to four layers of cuboidal cells. When inflamed, the fibrous wall is more collagenized, with a chronic inflammatory infiltrate. The epithelial lining is hyperplastic, and a keratinized surface is sometimes observed.
The exact histogenesis of dentigerous cysts is still unknown, but most authors agree they are of developmental origin.
It has been suggested that two types of dentigerous cysts exist6. The first are developmental cysts of the permanent dentition, and are usually the result of an impacted tooth. These cysts occur in the second or third decade of life and are discovered on routine radiographs. The second type are inflammatory cysts that occur in immature teeth, as a result of periapical inflammation, generally due to a nonvital deciduous tooth or to dissemination of an inflammatory process affecting the follicle of a permanent tooth. These cysts are diagnosed in the first or second decade of life. It has also been suggested that concomitant use of ciclosporin and calcium channel blockers may have an influence on the formation of maxillary cysts. These drugs may alter mechanisms that regulate gingival stromal tissue reabsorption, thus causing gingival hypertrophy, which may obstruct tooth eruption and, consequently, facilitate cyst development7.
The role of the p53 protein in the development of odontogenic cysts through alterations in cell proliferation was studied by Piattelli et al.8, who found that p53- positive tissues appear to exhibit greater proliferative activity; of the 24 cases of dentigerous cysts studied, 9.1% were positive for this protein.
On radiography, a dentigerous cyst should be suspected if the follicular space is larger than 5 mm2. The lesion appears as a radiolucent, unilocular area, with well-defined sclerotic borders, associated with the crown of an unerupted tooth. Cortical expansion and root resorption are often observed1, but other lesions have also been reported. Lung et al.9 reported a case of intra- and extraosseous dental displacement, with migration of the tooth into the submandibular soft tissues.
Clinically, the differential diagnosis of dentigerous cyst must include other cystic lesions, such as keratocyst and primordial cyst, and odontogenic tumors such as mural ameloblastoma, unilocular ameloblastoma, ameloblastic fibroma, and adenomatoid odontogenic tumor5,10. Even more severe entities, such as glandular odontogenic cyst11 or even squamous cell carcinoma, the management of which differs substantially from that of dentigerous cysts, should be considered in the differential diagnosis of these lesions12-13.
In a study of 327 patients with head and neck infections requiring hospitalization14, the underlying etiology was a dentigerous cyst in 7 cases.
The usual treatment is judicious enucleation of the cyst and removal of the impacted or unerupted tooth. If eruption of the involved teeth is viable, enucleation alone may be performed. Large cysts may be marsupialized instead to facilitate decompression, and enucleated later through a more conservative surgical procedure. If complete excision is achieved, the prognosis is excellent and recurrence is rare5.
Ertas & Yavuz15 reported a case in which four extremely displaced teeth associated with an extensive dentigerous cyst in a 9-year-old erupted after marsupialization alone, with no need for postoperative orthodontic treatment. The authors believe that eruption is dependent on patient age and incomplete root formation.
Marsupialization is advocated as a treatment option for dentigerous cysts, particularly in children10.
The proposed treatment for cysts considered to be of inflammatory origin is extraction of the nonvital deciduous tooth and marsupialization of the lesion to enable eruption of the permanent tooth6.
CASE REPORT
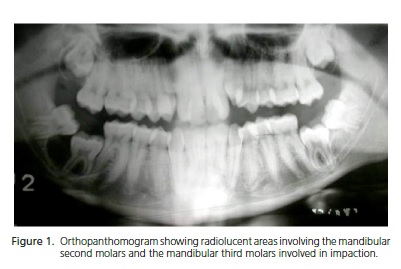
A 15-year-old white male presented to the Department of Oral Surgery of the Universidade de Pernambuco School of Dentistry (FOP/UPE) with a chief complaint of enlargement of the right retromolar region of 6 months' duration. The patient denied any parafunctional habits, smoking, alcohol intake, or systemic changes. Extraoral examination revealed facial asymmetry with marked enlargement in the region of the right mandibular body, which was firm and tender to palpation. Intraoral examination showed a firm, tender area of enlargement of the buccal cortical plate of the mandible, with no mucosal discoloration; teeth #37, #38, #47, and #48 were absent. Radiographs showed unilocular, well-circumscribed radiolucent areas involving the crowns of the mandibular second molars, which were retained due to mechanical restrictions caused by horizontally impacted third molars (Figure 1). History, physical examination, and imaging did not provide any evidence of syndromic or systemic involvement.
Based on the clinical and radiographic characteristic, a tentative diagnosis of dentigerous cyst was established for both lesions. Prior to definitive treatment, bilateral needle aspiration (yielding strawcolored fluid) and incisional biopsies were performed. The surgical specimens were sent to the FOP/UPE Department of Oral Pathology for analysis. Histological examination revealed an uninflamed connective tissue capsule, with remnants of odontogenic epithelium, and three to four layers of cuboidal cells in the epithelium of the cyst. Both lesions received a final histopathological diagnosis of dentigerous cyst.
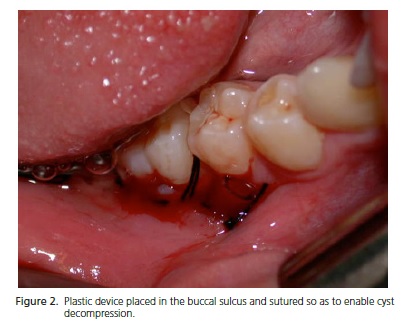
The right-sided cyst was decompressed by placing a plastic device during extraction of the impacted third molar. The device was kept in place for 2 months, and the patient was instructed to perform daily irrigation with 0.9% saline solution through the device and adhere to excellent oral hygiene practices. The cyst was removed completely at a later stage (Figure 2), after its dimensions had been reduced by decompression.
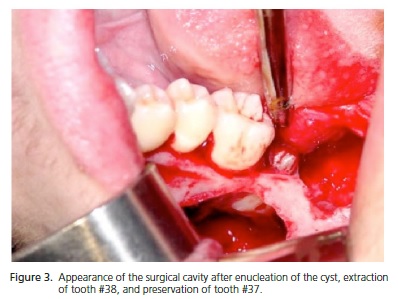
The left-sided cyst was enucleated during extraction of the third molar (Figure 3).
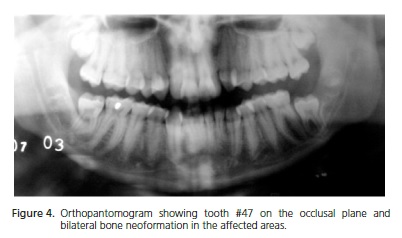
At 7-month follow-up, radiographic examination showed eruption of tooth #47, to the occlusal plane, as well as bone neoformation in the area previously visualized as a large radiolucency in the region of teeth #47 and #48; on the left side, tooth #37 had erupted and there was visible bone neoformation in the region of #37 and #38 (Figure 4), thus demonstrating the absence of recurrence.
DISCUSSION
Bilateral occurrence of dentigerous cysts in nonsyndromic patients is a rare condition9. Only 17 cases of bilateral dentigerous cyst in the absence of a syndrome or systemic disease have been reported.
Dentigerous cysts are typically asymptomatic1, but clinical complications such as development of inferior alveolar nerve paresthesia arouse suspicion of more serious conditions, such as malignancies, direct or indirect neurovascular injury, or systemic diseases such as diabetes or multiple sclerosis. One case of paresthesia in a patient with a mandibular dentigerous cyst was resolved after excision5. In the present case, the patient's only complaint was enlargement and tenderness of the affected area.
The differential diagnosis of dentigerous cyst must include lesions such as keratocyst and primordial cyst and odontogenic tumors such as mural ameloblastoma, unilocular ameloblastoma, ameloblastic fibroma, and adenomatoid odontogenic tumor5,10. Bilateral dentigerous cysts should raise suspicion of a syndrome or systemic condition1. Neither was found in the present case, which is exceedingly rare.
Treatment of dentigerous cysts generally consists of enucleation. However, cysts that cause major dental displacement and involve major bone loss must be decompressed. This treatment modality encourages new bone formation, as marsupialization decreases pressure within the cyst. The main disadvantage of marsupialization is that pathological tissue remains in situ and is not examined histologically. The cyst tissue removed with the bony window can be sent for anatomic pathology examination, but a more aggressive lesion may be present in residual tissue16.
In the case described herein, marsupialization of the right mandibular angle lesion was justified by the risk of fracture with single-stage enucleation. At the left mandibular angle, where the lesion was smaller, the decision to perform single-stage enucleation proved safe and appropriate. As the horizontal position of the mandibular third molars was the true cause of impaction of teeth #37 and #47, the decision was made to extract the third molars and conduct rigorous follow-up of eruption of the second molars.
In the vast majority of cases, dentigerous cysts can be treated via an intraoral approach, as in this report. There are two reports in the literature of enucleation of dentigerous cysts and extraction of the associated tooth via the extraoral (Risdon) approach described by Ellis & Zide17,18. In both cases, the inferior border of the mandible was substantially weakened and the authors decided to use internal fixation to provide reinforcement and prevent mandibular fractures.
Some authors19-20 have reported that surgery is not the only treatment modality for dentigerous cyst. Two rare cases of bilateral dentigerous cysts treated with a conservative approach have been reported; both progressed to spontaneous resolution, preventing an unnecessary surgical procedure19. However, the mechanism involved in spontaneous regression is still unknown. It is believed that rupture of the cyst wall creates an opening into the oral cavity, decompressing the lesion in a manner similar to marsupialization20.
CONCLUSION
This report presented two treatment modalities used to address the same pathological condition. This combination was justified by the discrepancy in size of the two lesions, and enabled successful treatment of both.
When dentigerous cysts are present bilaterally, the patient should be investigated for syndromes or systemic disease, as this presentation is exceedingly rare in nonsyndromic settings.
Collaborators
HHA MORAIS, TGS DIAS, RJH VASCONCELLOS and BV EGITO, were responsible for surgery and writing the article. AR MELO, DA GONDIM and R WATSON were responsible for writing the article.
REFERENCES
1. Freitas DQ, Tempest LM, Sicolis E, Lopes-Neto FC. Bilateral dentigerous cysts: review of the literature and report of an unusual case. Dentomaxillofac Radiol. 2006;35(6):464-8. doi: http://dx.doi.org/10.1259/dmfr/26194891 [ Links ]
2. Ko KS, Dover DG, Jordan RC. Bilateral dentigerous cysts--report of an unusual case and review of the literature. J Can Dent Assoc. 1999;65(1):49-51.
3. Desai RS, Vanaki SS, Puranik RS, Tegginamani AS. Dentigerous cyst associated with permanent central incisor: a rare entity. J Indian Soc Pedod Prev Dent. 2005;23(1):49-50. doi: 10.4103/0970-4388.16030
4. Ustuner E, Fitoz S, Atasoy C, Erden I, Akyar S. Bilateral maxillary dentigerous cysts: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(5):632-5. doi: 10.1067/ moe.2003.123
5. Aziz SR, Pulse C, Dourmas MA, Roser SM. Inferior alveolar nerve paresthesia associated with a mandibular dentigerous cyst. J Oral Maxillofac Surg. 2002;60(4):457-9. doi: 10.1053/joms.2002.31238
6. Benn A, Altini M. Dentigerous cysts of inflammatory origin: a clinicopathologic study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81(2):203-9. doi: 10.1016/S1079- 2104(96)80416-1
7. De Biase A, Ottolenghi L, Polimeni A, Benvenuto A, Lubrano R, Magliocca FM. Bilateral mandibular cysts associated with cyclosporine use: a case report. Pediatr Nephrol. 2001;16(12):993-5.
8. Piattelli A, Fioroni M, Santinelli A, Rubini C. P53 protein expression in odontogenic cysts. J Endod 2001;27(7):459-61.
9. Lung K, Ganatra S, Robinson CE, Dobrovolsky W, Peters E. Multiple multilocular dentigerous cysts with intra-osseous and extraosseous third molar displacement: a case report [cited 2012 Ago 10]. Available from: <http://www.oralhealthgroup.com/news/ multiple-multilocular-dentigerous-cysts-with-intra-osseous-andextra- osseous-third-molar-displacemen/1000204906/>.
10. Martinez-Perez D, Varela-Morales M. Conservative treatment of dentigerous cysts in children: a report of 4 cases. J Oral Maxillofac Surg. 2001;59(3):331-3. doi: 10.1053/joms.2001.21006
11. Kasaboglu O, Basal Z, Usubutun A. Glandular odontogenic cyst presenting as a dentigerous cyst: a case report. J Oral Maxillofac Surg. 2006;64(4):731-3.
12. Yasuoka T, Yonemoto K, Kato Y, Tatematsu N. Squamous cell carcinoma arising in a dentigerous cyst. J Oral Maxillofac Surg. 2000;58(8):900-5. doi: 10.1053/joms.2000.8219
13. Gulbranson SH, Wolfrey JD, Raines JM, Mcnally BP. Squamous cell carcinoma arising in a dentigerous cyst in a 16-month-old girl. Otolaryngol Head Neck Surg. 2002;127(5):463-4. doi: 10.1067/mhn.2002.129039
14. Smith JL 2nd; Kellman RM. Dentigerous cysts presenting as head and neck infections. Otolaryngol Head Neck Surg. 2005;133(5):715-7. doi: 10.1016/j.otohns.2005.07.014
15. Ertas U, Yavuz MS. Interesting eruption of 4 teeth associated with a large dentigerous cyst in mandible by only marsupialization. J Oral Maxillofac Surg 2003;61(6):728-30. doi: 10.1053/ joms.2003.50145
16. Peterson LJ, Edward E, Hupp JR, Myron RT. Cirurgia oral e maxilofacial contemporânea. 2ª ed. Rio de Janeiro: Guanabara Koogan; 2000.
17. Ellis E, Zide MF. Surgical aprroaches to the facial skeleton. 2 ed. Baltimore: Williams & Wilkins; 2006.
18. Mintz S, Allard M, Nour R. Extraoral removal of mandibular odontogenic dentigerous cysts: a report of 2 cases. J Oral Maxillofac Surg. 2001;59(9):1094-6. doi: 10.1053/ joms.2001.25857
19. Chew YS, Aghabeigi B. Spontaneous regression of bilateral dentigerous cysts: a case report. Dent Update. 2008;35(1):63-5.
20. Shah N, Thuau H, Beale I. Spontaneous regression of bilateral dentigerous cysts associated with impacted mandibular third molars. Br Dent J. 2002;192(2):75-6. doi:10.1038/ sj.bdj.4801297
 Correspondence to:
Correspondence to:
HHA MORAIS
e-mail: heciomorais@hotmail.com
Received on: 16/6/2013
Final version resubmitted on: 28/8/2013
Approved on: 17/2/2014
