










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.63 no.3 Porto Alegre Jul./Set. 2015
ORIGINAL / ORIGINAL
Retention evaluation of two glass ionomer cement sealants: sixmonth clinical follow-up
Retenção de dois selantes ionoméricos: 6 meses de acompanhamento clínico
Alline FRAYI; Thaís Manzano PARISOTTOII; Gabriela Azevedo de Vasconcelos Cunha BONINII; Regina Maura Coli SIEGLI; José Carlos Pettorossi IMPARATOIII
I Faculdade São Leopoldo Mandic, Curso de Odontologia, Programa de Pós-Graduação Odontopediatria. Rua José Rocha Junqueira, 13, Swift, 13045- 755, Campinas, SP, Brasil
II Universidade São Francisco. Bragança Paulista, SP, Brasil
III Universidade de São Paulo, Faculdade de Odontologia, Departamento de Ortodontia e Odontopediatria. São Paulo, SP, Brasil
ABSTRACT
Objective
The aim of this study was to evaluate the retention of glass ionomer sealant, Vitro Molar® (DFL) and Ketac Molar Easy Mix® (3 m ESPE) as pit and fissure sealants on first permanent molars, fully or partially erupted.
Methods
The study sample consisted of 412 molars, among 110 children. The sealant retention was evaluated after 6 months of the application.
Results
The results were collected through digital photographs and the retention results were assessed by the following System: score 0 - total retention; score 1 - sealant present in more than 50% of the pit and fissure system; score 2 - sealant present in less than 50% of the pit and fissure system; score 3 - missing sealant. Regarding the presence of the sealants in less than 50% of the occlusal surface, lower percentages were found for the two materials used as follows: score score 2 - Vitro Molar® (9,52% examiner 1 and 11.9% examiner 2) and score 2 - Ketac Molar Easy Mix® (9.52% examiner 1 and 10.71% examiner 2). Approximately 90% of the teeth sealed with Ketac Molar Easy Mix® or Vitro Molar® presented total loss (score 3). Thus, there was no statistical difference between the materials and between the examiners (p>0.05).
Conclusion
Therefore it was concluded that the sealant retention in the studied population was not satisfactory for any of the materials used.
Indexing terms: Glass ionomer cements. Molar. Pit and fissure sealants.
RESUMO
Objetivo
Avaliar a retenção do cimento de ionômero de vidro, Vitro Molar® (DFL) e Ketac Molar Easy Mix® (3M ESPE) como selantes para fóssulas e fissuras em primeiros molares permanentes hígidos, parcialmente ou totalmente irrompidos.
Métodos
A amostra para este estudo foi de 412 molares selados condizentes com um total de 110 crianças. A avaliação da retenção dos selantes foi realizada após 6 meses da aplicação.
Resultados
Os resultados foram coletados por meio de fotografias digitais através do Sistema de Avaliação de Selantes: escore 0 = selante presente em toda o sistema de fissuras; escore 1 = selante presente em mais de 50% do sistema de fissuras; escore 2 = selante presente em menos de 50% do sistema de fissuras; escore 3 = selante ausente. Com relação a presença dos selantes em menos de 50% das fissuras, as porcentagens foram baixas para os dois materiais: score 2 - Vitro Molar® (9,52% avaliador 1 e 11,9% avaliador 2) e score 2 - Ketac Molar Easy Mix® (9,52% avaliador 1 e 10,71% avaliador 2). Cerca de 90% dos dentes selados com Ketac Molar Easy Mix® ou Vitro Molar® apresentaram perda total (score 3). Portanto, não houve diferença estatística tanto entre os materiais como entre os examinadores (p>0.05).
Conclusão
Sendo assim, concluiu-se que a retenção dos selantes na população estudada foi insatisfatória para os 2 materiais.
Termos de indexação: Cimentos de ionômeros de vidro. Dente molar. Selantes de fossas e fissuras.
INTRODUCTION
There has been a continuous decrease in the levels of caries over the last 30 years, due to advanced technology and scientific development especially in more developed countries1. According to the SB Brazil 2010 project2, the decrease of dental caries has been irregular and the prevalence reaches about 80% of caries in 5 yearold children. In the permanent dentition, 20% of the 12 year-old population presents at least one decayed tooth.
The caries reduction is due to different factors, such as: general health improvement, decreased consumption of sugar3, treatment and dental diagnosis development as well as the use of various preventive measures, mainly fluorides4-5. Nevertheless, the caries illness has still been harmful to human health6.
Pits and fissures are biofilm stagnation sites and affect more than 80% of caries lesions, compared to smooth surfaces, where the decreased prevalence of caries has mostly occurred once oral hygiene prevention and fluoride treatments are more effective7-8.
Thus, prevention of the occlusal surface is essential, particularly in children, since they usually present greater risks, due to the highly cariogenic diet and teeth erupting phase, which facilitate retention of food residues and microorganisms9. Systematic reviews, randomized controlled clinical trials and consulted Meta-analyzes emphasize that the pit and fissure ionomer sealing is highly effective in preventing caries lesions and treatment of incipient lesions8,10-16.
Glass ionomer cements are very suitable for permanent molars erupting, since they are less sensitive to humidity compared to resin sealants17. Thus, they are more proper in erupting teeth and do not allow complete isolation. They also present good adhesion and chemical release and incorporate fluoride. Furthermore, both ionomeric and resin sealants are effective in preventing the disease. Nevertheless one advantage of the ionomer sealant is that its partial loss does not necessarily indicate ineffectiveness since part of the material remains trapped in the bottom of the fissure, releasing fluoride and preventing caries.
Therefore, this study has evaluated the retention of two ionomeric sealants after a 6-month follow up despite of total or partial retention, once many studies have shown effectiveness against caries lesions, due to material particles found at the pit and fissure bottom. However, further studies comparing glass ionomer materials are needed in order to improve oral health.
METHODS
The survey was performed after approval by the Ethics Research Committee of the Faculty of São Leopoldo Mandic Dental School under number 2012/0002. A Term of Consent, allowing the child to participate in the survey was delivered to the parents or legally responsible for him and data were kept confidential and only patients who had signed this agreement participated in the study.
This study was composed of 5-7 year-old male and female children, from different race groups, who were assisted at the Health Centers in the city of Serra Negra, State of São Paulo, Brazil.
The sample consisted of 110 children and 412 teeth sealed with glass ionomer materials (Vitro Molar (DFL) and Ketac Molar Easy Mix® (3M ESPE).
Inclusion criteria
The criteria for inclusion in the study were as follows: the age group 5-7 years old; a signed free and informed consent, the Secretary of Health's authorization and patient presenting at least two healthy first permanent molars, partially or fully erupted.
The patients, who were excluded from the study and presented unmistakable caries lesion in permanent molars, undermined enamel, or detectable floor or wall softening, were referred for treatment in the Health Center of the city of Serra Negra, State of São Paulo, Brazil.
Sample capture
The survey was released by a researcher of the study who visited the city public schools, previously selected. The ages 5 to 7 years old defined the presence of erupting or fully erupted permanent molars. At this time, the Free Informed Consent ,was delivered to the (a) coordinator (a) in charge of each school, who made it available to the parents and legally responsible for the children and that were present at the Teachers and Parents' School meetings thus avoiding a possible loss of the document and the possible research misunderstandings The researcher previously met, at the time of visit, with each coordinator (a) in order to clarify details concerning the objective, implementation and results of the research.
Data collection
A month afterwards the researcher's visit to the city of Serra Negra, State of São Paulo, Brazil for sample collection, the Terms of Consent Form were collected and the best time for sealing treatment accomplishment was set as well a data collection after 6 months.
The procedures were performed in each school environment in accordance with the morning and evening periods and each teacher efficiently took 3 students/ authorized patients at a time to the place agreed for the treatment. Some schools made tables, extra stretchers and chairs available and a better spot of enhanced lighting was asked for whenever needed. The procedures were also performed in classrooms food patios, sport courts where a better lighting was required and provided. No dental chair, sucking nor reflectors were provided as help.
The sessions were carried out by two people: a glass ionomer material manipulator, also present for the performance of image capture equipment and after at the six- month follow-up, and the researcher who performed clinical procedures and data collecting / patient information.
Sample design
The study sample was divided into two groups
In both groups, upon arriving at the place determined by each school and all table procedures and camera were prepared. The patients had already undergone prophylactic procedures using their own toothbrushes and fluoride toothpastes with a concentration above 1000 ppmF as usual; instructed by the teachers themselves. Then, each patient's file was separated by name, and taken to the stretcher, chair or table and because they were 5-7 year old children proper behavior management was carefully fulfilled by the researcher. By doing so no patient's rejection to the treatment was noticed and the fact that they were observed by two other classmates was a great motivation and help during the treatment.
After this, the clinical examination was performed, the presence of two or more first permanent healthy molar eruption or fully erupted was verified. The procedure chosen was the mouth divided randomly, that is , for any 16 and / or 36 teeth using Molar® Vitro (DFL) (Group I) and for every tooth 26 and / or 46 teeth using Ketac Molar Easy Mix® (3M ESPE) (Group II).
Pit and fissure sealing
The person who manipulated the material had been properly trained before and the materials were applied according to manufacturers' instructions
Technique for sealing with glass ionomer
a) brushing teeth with fluoride toothpaste - held by teachers in a determined place for tooth brushing at school facilities;
b) mouth washing using the water coming from the place for tooth brushing, using indefinite time;
c) isolation with cotton rollers - was only used mouth openers were only used for help for patients who did keep their mouth open or had little opening; d) drying of the occlusal surface with cotton balls/pellets;
e) Initial image capture;
f) etching with polyacrylic acid according to the manufacturer's recommendations for 10 seconds;
g) Wash with cotton pellet humidified by water;
Material handling - performed by the person who captured the images, while the researcher dealt with the isolation.
Vitro Molar® (DFL) (COMPOSITION: The powder contains: Barium and Aluminum silicate, and Dehydrated Polyacrylic Acid and Iron Oxide.
The liquid portion contains: Polyacrylic Acid, Tartaric Acid and Distilled Water. The conditioner contains: Polyacrylic Acid, Glycerin, 200 Aerosil, Blue CI 52015 Methylene and deionized water - with a paper pad, plastic spatula - one part of glass-ionomer cement to one drop of the liquid, dividing the powder into two parts, using the spatula for 10 seconds until a homogeneous, smooth and shiny mass is formed and a1cm strand is prepared.
Ketac Molar Easy Mix® (3M ESPE) (Composition - Powder: fluorsilicate glass, strontium and lanthanum, liquid: policarbonic acid, tartaric acid and water - with a paper pad, plastic spatula - one part of Glass- ionomer cement for one drop of the liquid, dividing the powder into two parts, using the spatula for 30 seconds until forming a homogeneous, smooth and glossy mass until a 1cm strand comes out.
a) occlusal surface insertion using spatula;
b) wait for material adherence; c) Ketac Molar Easy Mix® (3M ESPE) - 3 minutes;
d) Vitro Molar® (DFL) - 30 seconds;
e) digital pressure with a gloved Vaseline finger;
f) removal of exceeding with curette or probe, protecting with Vaseline(cotton);
g) rubber dam removal and occlusion test;
h) patient's guidance and advice which was also passed on to TEACHERS who registered in each school report - minimum of 1 hour after the procedure for eating and the next day, feeding should include soft and non-solid food and good oral hygiene observed;
i) final image performed.
Sealed teeth were re-examined after six months of material application. The researcher returned to the city of Serra Negra and patients were located through their records
These results were observed through assistance with images taken from the same camera and the researcher's help for mouth opening and mirror positioning.
The assessment of the sealant retention was carried out by a third and fourth blind person, through the criteria of Sealants Evaluation System criteria proposed as adequate and flexible methodology for assessing the sealant quality18.
These people were trained by the study researcher through the sheet for records of demographic data and analysis of retention of sealants. Thus, the sealants were classified into 4 scores: score 0 = sealant present in all the fissure system; score 1 = sealant present in more than 50% of the fissure system; score 2 = sealant present in less than 50% of the fissure system; score 3 = absent sealant.
Data analysis
Data were analyzed using descriptive statistics (percentages) and the Mann-Whitney test (α = 0.05) to compare the retention of the two materials. Data normality was verified by Lilliefors test (α = 0.05) which showed nonnormal distribution.
RESULTS
This study evaluated a total of 412 sealed teeth, 50% with ionomer Vitro Molar® materials and the other half, 50% with ionomer Ketac Molar Easy Mix® materials.
Each child received both materials by cross technique.
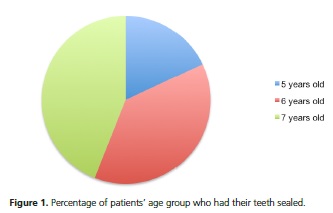
The age of these patients ranged from 5 to 7 years of age, according to the observed, 18.18% of patients were 5 years old, 38.18% were 6 years old and 43.63% were 7 years old (Figure 1).
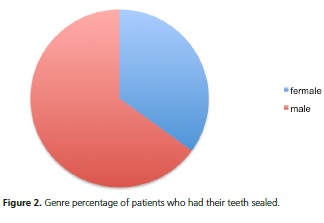
The patients who had their teeth sealed were 35.45% female and 64.54% were male (Figure 2).
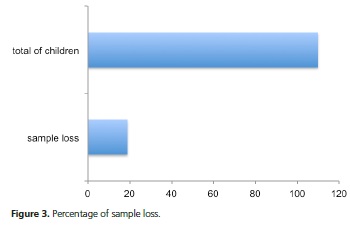
Among the sealed teeth, it was observed that the total of 110 children was assisted, but there was a sample loss of 17.27% afterwards in the six month assessment due to the children's absence at school. The main reason for this loss was that the patients moved from city or changed school (Figure 3). By age, schools are divided into kindergartens and elementary school and the year selected was precisely the last preschool year, that is the total study time led to last year in that school and since these students/patients come from a small town, many change their children to schools in neighboring towns.
After 6 months these teeth were evaluated for retention of glass ionomer materials.
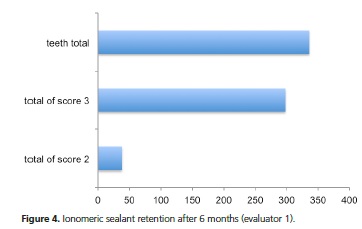
Two blinded evaluators reported the score for each tooth sealed through photographic images. The first evaluator obtained 90.47% score 3, that is total loss of sealants and 9.53% of score 2, this sealant in less than 50% of the fissures system (Figure 4).
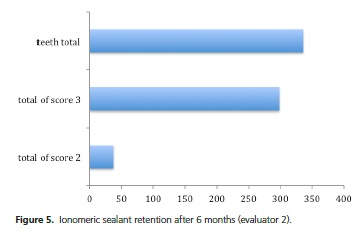
The second reviewer observed 3 88.69% of score 3, that is complete loss of sealant, and 11.30% of score 2; this sealant was observed in less than 50% of the fissure system (Figure 5).
Concerning the retention of ionomeric materials, the teeth which showed some retention of the sealant, i.e. the material in less than 50% of the fissure system (score 2) corresponded to 9.52% and 11.9% for Vitro Molar® (evaluator 1 and 2 respectively) and 9.52% and 10.71% for Ketac Molar Easy Mix® (evaluator 1 and 2 respectively). About 90% of teeth sealed with Ketac Molar Easy Mix® or Molar® Vitro presented a total loss (score 3) (Figure 6).
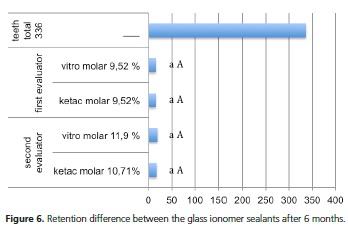
Equal lowercase letters indicate: no statistical difference by Mann-Whitney test (α = 0.05) comparing the two materials by the evaluator 1 (p = 0993) and 2 (p = 0.991); Equal capital letters indicate: no statistical difference by Mann-Whitney test (α = 0.05) comparing the two evaluators as to the Ketac Molar Easy Mix® (p = 0.777) and Molar® Vitro (p = 0776).
DISCUSSION
Regarding the materials used, Vitro Molar® and Ketac Molar Easy Mix®, similar retention was observed for both materials, ranging around 2% for Ketac Molar Easy Mix®, being the latter chosen for this study due to its largest number of research evidence and the choice of Molar® Vitro due to its lower cost in public health. As in this study, there was no statistical difference regarding the retention of materials, Vitro Molar ® (DFL) was indicated as an option for public health use.
At preschool age, it is common for children to present a highly cariogenic diet and bad hygiene due to their fact still poor motor skills and permanent teeth eruption. These factors contribute to the greater food and microorganism accumulation, which brings considerable importance for the occlusal surface protection9. One way to accomplish this is through protective pit and fissure sealants to prevent the development of caries13,19 as if a physical barrier20. On the other hand, the fact that the tooth is fully or still erupting , does not go along with the increase in retention of sealants but with poor oral hygiene providing the greatest accumulation of food and consecutively increase in the risk of caries activity.
The aim of this study was to evaluate the retention of two different glass ionomer materials on first permanent healthy molars chosen for easy handling in school settings, nonetheless their implementation is impaired by factors as such: patient's positioning, site lighting,difficulty in accessing posterior teeth small pits and the absence of any suitable drying for sucking site, although excellent patients' behavior overcome all these impairments besides the fact that this environment is more natural for the patients, there is no dentist chair and the absence of some dental instruments which they sometimes fear and also the fact that the patients can see their colleagues' teeth being sealed The same goes for reports of a study where glass ionomer sealants were also made in prevention of benefit programs associated with the formula with fluoride released in the oral cavity, since they are not sensitive to moisture when compared to resin sealants, easy implementation and patients 'acceptance; which greatly contributes to public health and economic factors in the country19,21.
Despite being difficult to find children who participated in the six month survey afterwards , due to the grade change and students moving to other cities, sample loss results were of only 17.27 %.,which is considered a low percentage considering the number of children assisted and the contribution to their oral health.
Preventive sealing performed in the school setting have shown excellent results as the prevention of caries activity19.The rapid loss of sealants shows failure in retention, but does not mean failure in the preventive effect by the presence of some of the material on the fissure background. This supports the fact that even with the result of low retention among the materials chosen for this study after six month evaluation, added to the difficulties of performance at the school environment and the absence of a dental professional for the prior prophylaxis performed, (oral hygiene was perfomed with the teachers) the sealing effectively helped in preventing caries22.
There was no statistically significant difference between the two evaluators in the retention criterion comparing the two materials (Figure 6). Both had a close percentage 90.47% / 88.69% of total loss of sealant and 9.52% / 11.30% sealant present in less than 50% of the fissure system. Therefore, the result was similar for the two different evaluators.
The evaluation criterion through photographs was chosen for the following reasons: it facilitates approximate assessment due to the place where the sealings were performed; by the photograph zoom extension, once seeing directly would impair this view. There were also the following difficulties:-To return to the city of Serra Negra with two assessors due to the distance, enter the schools at any time, preventing the progress of students' school activities and find the students who had perhaps changed their school and / or moved to another city. The study showed that the fact that the same person who captured the initial and final images eliminates error percentages of this study.
The greatest difficulty in providing a clear capture all the sealed teeth, was the fact that many children did not have good mouth opening and the mirror fogged up quickly by the absence of air surface drying.
However, more studies should be performed about this method and materials used. Health promotion includes education, food and good life quality,therefore prevention is essential. One suggestion would be to evaluate the caries preventive effect with this retention research.
CONCLUSION
It was concluded that the retention of the two glass ionomer sealants used was low, and there was no statistical difference between them.
Collaborators
A FRAY, JCP IMPARATO, GAVC BONINI, RMC SIEGL, TM PARISOTTO participated in all stages of preparation of the article.
REFERENCES
1. Bonecker M, Ardenghi TM, Oliveira LB, Sheiham A, Marcenes W. Trends in dental caries in 1- to 4-year-old children in a Brazilian city between 1997 and 2008. Int J Paediatr Dent. 2010;20(2):125-31. doi: 10.1111/j.1365-263X.2009.01030 [ Links ]
2. Brasil. Ministério da Saúde. Projeto SB Brasil 2010: condições de saúde bucal da população brasileira 2010 - Resultados parciais. Brasília; Ministério da Saúde; 2011 [citado 204 Nov 10]. Disponível em: < http://dab.saude.gov.br/CNSB/sbbrasil/ arquivos/projeto_sb2010_relatorio_final.pdf >.
3. Neumann SRB, Freitas SFT, Lacerda JT. Prevalência de cárie e fatores associados na Dentição decídua em escolares de sete anos de idade da rede pública de Joinville, SC, Brasil. Pesq Bras Odontoped Clin Integr. 2010;10(3):405-11.
4. Fejerskov O. Concepts of dental caries and their consequences for understanding the disease. Community Dent Oral Epidemiol. 1997;25(1):5-12.
5. Cagnani A, Barros AMS, Sousa LLA, Oliveira AMG, Zanin L, Flório FM. Association between preference for sweet foods and dental caries. RGO, Rev Gaúch Odontol. 2014;62(1):25-9.
6. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. 2007; 369(9555):51-9.
7. Karlzén-Reuterving G, van Dijken JW. A three-year follow-up of glass ionomer cement and resin fissure sealants. ASDC J Dent Child. 1995;62(2):108-10.
8. Ripa LW. Sealants revisted: an update of the effectiveness of pit and fissures sealants. Caries Res. 1993;27(1):77-82.
9. Menoli APV, Oliveira LB, Imparato JCP. Uso de selantes na prevenção de cárie oclusal em crianças e adolescentes: revisões sistemáticas da literatura. In: Imparato JCP, Raggio DP, Mendes FM. Selantes de fossas e fissuras. São Paulo: Santos; 2008. P. 25-37.
10 Baldini V, Tagliaferro EPS, Ambrosano GMB, Meneghim MC, Pereira AC. Use of occlusal sealant in a community program and caries incidence in high - and low - risk children. J Appl Oral Sci. 2010;19(4):396-402.
11. Guler C, Yilmaz Y. A two-year clinical evaluation of glass ionomer and Ormocer based fissure sealants. J Clin Pediatr Dent. 2013;37(3):263-7.
12. Ahovuo-Saloranta A, Hiiri A, Nordblad A, Mäkelä M, Worthington HV. Pit and fissure sealants for preventing dental decay in the permanent teeth of children and adolescents. Cochrane Database Syst Rev. 2013;8(4):CD001830.
13. Beiruti N, Frencken JE, van't Hof MA, Taifour D, van Palenstein Helderman WH. Caries-preventive effect of a one-time application of composite resin and glass ionomer sealants after 5 years. Caries Res. 2006;40(1):52-9. doi:10.1159/000088907
14. Muller-Bolla M, Lupi-Pégurier L, Tardieu C, Velly AM, Antomarchi C. Retention of resin-based pit and fissure sealants: a systematic review. Community Dent Oral Epidemiol. 2006;34(5):321-36.
15. Mickenautsch S, Yengopal V. Caries-preventive effect of glass ionomer and resin-based fissure sealants on permanent teeth: An update of systematic review evidence. BMC Res Notes. 2011; 4(1):22. doi: 10.1111/j.1600-0528.2006.00319.x
16. Yengopal V, Mickenautsch S. Resin-modified glass-ionomer cements versus resin-based materials as fissure sealants: a metaanalysis of clinical trials. Eur Arch Paediatr Dent. 2010;11(1):18- 25.
17. Morales-Chávez MC, Nualart - Grollmus ZCN. Retention of a resin-based sealant and a glass ionomer used as a fissure sealant in children with special needs. J Clin Exp Dent. 2014;6(5):e551- 5. doi: 10.4317/jced.51688
18. Deery C, Fyffe HE, Nugent ZJ, Nuttal NM, Pitts NB. A proposed method for assessing the quality of sealants - the CCC Sealant Evaluation System. Community Dent Oral Epidemiol. 2001;29(2):83-91. doi: 10.1111/j.1600-0528.2001.290202.x
19. Frencken JE, Wolke J. Clinical and SEM assessment of ART high viscosity glass-ionomer sealants after 8-13 years in 4 teeth. J Dent. 2010 Jan;38(1):59-64. doi: 10.1016/j.jdent.2009.09.004
20. Berger S, Goddon I, Chen C-M, Senkel H, Hickel R, Stösser L, et al. Are pits and fissure sealants needed in children with a higher caries risk. Clin Oral Investig. 2010 Oct;14(5):613-20. doi: 10.1007/s00784-009-0343-8
21. Joseph B, Dennison MS, Lloydh MS. Effectiveness of sealant treatment over five yers in in an insured population. J Am Dent Assoc. 2000;131(5):597-605.
22.Torppa-Saarinen E, Seppa L. Short-term retention of glass-ionomer fissures sealants. Proc Finn Dent Soc. 1990;86(2):83-8.
 Correspondence to:
Correspondence to:
A FRAY
e-mail: allinefray@gmail.com
Received on: 1/12/2014
Final version resubmitted on: 5/3/2015
Approved on: 25/5/2015
