










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.63 no.4 Porto Alegre Out./Dez. 2015
CLÍNICO / CLINICAL
Intramuscular lipoma in the temporal region: a case report
Lipoma intramuscular em região temporal: relato de caso clínico
Marcia Maria de GouveiaI; Ophir Ribeiro JúniorI; Rodrigo Autran de Paiva NunesI; Alexandre Meireles BorbaI; Carlos Augusto Ferreira AlvesI; Jayro Guimarães JúniorI
I Universidade de São Paulo, Hospital Universitário, Divisão de Odontologia, Departamento de Cirurgia Bucomaxilofacial
ABSTRACT
Few reports of intramuscular lipoma in the temporal region are seen in the literature. Because of its invasives characteristics, this neoplasm may be mistaken as a liposarcoma. Although image exams help in the differential diagnosis between benign and malignant lipomatous lesions, the histopathological exam is the only one capable of a definitive diagnosis. Total removal of the lesion is essential because the recurrence rate without complete excision may be as high as 62.5 %. A patient with an intramuscular lipoma located in the temporal region is presented along with the mentioned treatment. Great importance should be given to these uncommon lesions that may present as a challenge to professionals that work in the maxillofacial region.
Indexing terms: Lipoma. Muscle neoplasms. Temporal muscle.
RESUMO
Poucos relatos de lipoma intramuscular na região temporal são vistos na literature. Devido as suas características invasivas, essa neoplasia pode ser confundida com um lipossarcoma. Apesar de exames de imagem ajudarem no diagnóstico diferencial entre lesões lipomatosas benignas ou malignas, o exame histopatológico é o único capaz de diagnóstico definitivo. Remoção total da lesão é essencial pois a taxa de recidiva sem completa excisão pode ser de até 62,5%. Uma paciente com um lipoma intramuscular localizado na região temporal é apresentada com o devido tratamento da lesão. Grande importância deve ser dada a essas lesões incomuns que podem se apresentar como um desafio aos profissionais que atuam na região maxilofacial.
Termos de indexação: Lipoma; Neoplasias musculares. Músculo temporal.
INTRODUCTION
The intramuscular lipoma is a benign neoplasm of slow growth, composed by mature adipose cells permeated in a skeletal musculature, with invasive characteristics. Importance is given to the differential diagnosis of this neoplasm with liposarcoma because the similar clinical appearance of both diseases.
This tumor is rare in the maxillofacial region and associated with local recurrences. We report an intramuscular lipoma in the temporal muscle treated surgically, with no signs of recurrence after one decade of follow-up.
CASE REPORT
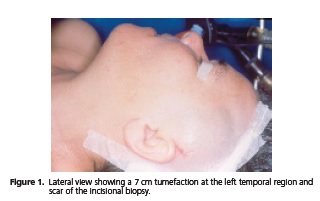
A white 42-years-old woman, referred swelling of slow growth in the left temporal region noticed nine months before. The patient related headache in the temporal region that extended to the frontal and parietal areas. The physical exam showed tumefaction of 7 cm at the left temporal region, painless to palpation, semi-firm consistency, and added to deeper layers (Figure 1). She also showed a slight functional limitation for mouth opening.
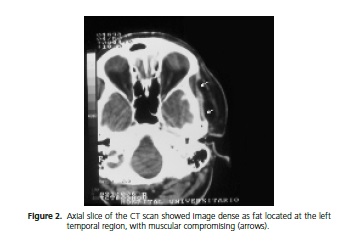
Computed tomography (CT) scans showed an image with the attenuation suggestive of fat, with welldefined margins, with muscular invasion (Figure 2). An incisional biopsy was executed to diagnose, through little supra-auricular incision on the left scalp. The histopathological result came as intramuscular lipoma.
The exeresis was done few days after, under general anesthesia. A hemi-coronal approach was made on the left side followed by dissection of the subcutaneous layer and identification the lesion's capsule (Figure 3). During the dissection, adhesion to the temporal muscle was observed. At the adhered region, muscle tissue was annexed to the exeresis.

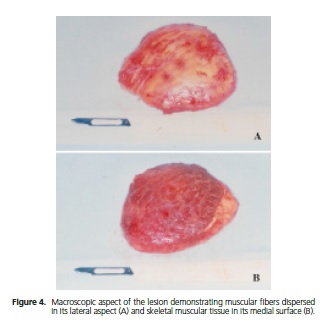
The macroscopic aspect showed a specimen measuring 7,0 x 6,5 x 2,4 cm, presenting yellow tissue with lobulated aspect and muscular fibers through it, covered externally at one face by skeletal muscle tissue (Figure 4). Microscopic examination showed neoplastic growth inter and intramuscular, with absence of lipoblasts, nuclear atypia or mitoses figures (Figure 5). The histopathologic exam confirmed the previous diagnosis.

In 10 years of observation, the patient presented good general health, with no complains or signs of recurrences and functional restrictions.
DISCUSSION
The intramuscular lipoma distinguishes itself from conventional lipomas because of its rarity and clinicpathological characteristics. This neoplasm is rare at neck and head region, being reported in the trapezius, sternocleidomastoid, tongue, cheek, floor of mouth and temporal muscle1-6. In some cases, it may be associated to a functional limitation of the affected muscle. Symptoms as headache and trismus are observed in cases that affect the temporal region4,6.
The CT scan is useful to define the limits of the intramuscular lipomas and evaluate its invasion in the surrounding tissues, but it is considered deficient for the differentiation with malignant lipomatoses. Magnetic resonance images are more effective than CT on the differentiation of the lipomas and liposarcomas, including the well-differentiated variant7. However, the histopathologic exam is essential to conclude the diagnosis3.
Recurrences are related to its invasive nature and the difficulty of its excision. The percentages varied from 3% to 62,5% and these rates might be related to the extension of exeresis1-2. Kindblom et al.2 showed a series of 33 intramuscular lipomas excised with margin of uninvolved surrounding tissues or myotomy. On their series, only one case (3%) recurred after 17 years. In our case, the lesion was totally removed, along with the muscular part added to its medial face. The patient has been observed for 10 years and has not shown signs of recurrence.
CONCLUSION
The intramuscular lipoma represents a rare lesion of the temporal region. Due to its great similarity with the liposarcoma, this lipomatose presents a diagnostic challenge for the several professionals that act in the maxillofacial region. As this lesion tends to local recurrence, removal of soft tissues adhered to it seems advisable for successful therapeutical achievement.
Collaborators
All authors provided the conception of the article, acquisition of data, drafting the manuscript and final approval of the submitted version.
REFERENCES
1. Garavaglia J, Gnepp DR. Intramuscular (infiltrating) lipoma of the tongue. Oral Surg Oral Med Oral Pathol. 1987;63:348-50. [ Links ]
2. Kindblom LG, Angervall L, Stener B, Wickbom I. Intermuscular and Intramuscular lipomas and hibernomas. A clinical, roentgenologic, histologic, and prognostic study of 46 cases. Cancer. 1974;33(3):754- 62. doi: 10.1002/1097-0142(197403)33:3<754::AIDCNCR2820330322> 3.0.CO;2-F
3. Piatelli A, Fioroni M, Rubini C. Intramuscular lipoma of the cheek: a case report. J Oral Maxillofac Surg. 2000;58(7):817-9. doi:10.1053/joms.2000.7281
4. Uemura T, Suse T, Yokoyama T, Mitsukawa N, Yoshikawa A. Intramuscular benign lipoma of the temporalis muscle. Scand J Plast Reconstr Surg Hand Surg. 2002;36(4):231-4.
5. Scolozzi P, Lombardi T, Maire G, Pedeutour F, Richter M. Infiltrating intramuscular lipoma of the temporal muscle. A case report with molecular cytogenetic analysis. Oral Oncol. 2003;39(3):316-22. doi:10.1016/S1368-8375(02)00117-3
6. Ban M, Kitajima Y. Intramuscular lipoma within the temporal muscle. Int J Dermatol. 2002;41(10):689-90. doi: 10.1046/j.1365-4362.2002.01618.x
7. Ohguri T, Aoki T, Hisaoka M. Differential diagnosis of benign peripheral lipoma from well-differentiated liposarcoma on MR imaging: is comparison of margins and internal characteristics useful? AJR Am J Roentgenol. 2003;180(6):1689-94. doi: 10.2214/ajr.180.6.1801689
 Correspondence to:
Correspondence to:
AM Borba
e-mail: alex80@terra.com.br
Received on: 28/10/2013
Final version resubmitted on: 17/1/2014
Approved on: 14/2/2014
