










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.64 no.2 Porto Alegre Abr./Jun. 2016
CLÍNICO | CLINICAL
Septic arthritis of the TMJ: a case report
Artrite séptica da ATM: relato de caso
Hécio Henrique Araújo de MORAIS I; Tony Santos PEIXOTO II; Jimmy Charles BARBALHO I; Tasiana Guedes de Sousa DIAS I; Ricardo José de Holanda VASCONCELLOS II; Eudes Euler de Souza LUCENA II
I Universidade do Estado do Rio Grande do Norte, Faculdade de Odontologia, Departamento de Cirurgia Buco-Maxilar
II Universidade Estadual da Paraíba, Departamento de Odontologia. Bodocongó, PB, Brasil
III Universidade de Pernambuco, Faculdade de Odontologia, Departamento de Cirurgia Oral e Maxilofacial. Camaragibe, PE, Brasil
ABSTRACT
Septic arthritis of the temporomandibular joint (TMJ) is an uncommon condition; thus, reports in the specialized literature are still scarce. The TMJ may be affected by extension of a local infectious process, by post-traumatic hematoma, or secondarily, by hematogenous spread. Septic arthritis is more common in the large joints, with the knee and hip most frequently affected. It is characterized by insidious onset and a marked inflammatory process, and is monoarticular in 80% of cases. The present report describes the case of a 6-year-old boy with a history of rheumatoid arthritis who presented with pain, swelling, and redness in the right TMJ region, as well as limited jaw opening, closure, and lateral excursion bilaterally. The differential diagnosis and treatment of this rare clinical entity are described. Aspects concerning antibiotic therapy and imaging studies are also addressed.
Indexing terms: Arthritis, infectious. Infection. Temporomandibular joint disorders.
RESUMO
A artrite séptica da articulação têmporo-mandibular (ATM) é uma entidade pouco freqüente, e por isso ainda pouco descrita na literatura internacional especializada. A articulação têmporo-mandibular pode ser afetada por uma extensão de um processo séptico local, hematoma pós-trauma ou secundariamente por disseminação pela via hematogência. É mais comum a sua apresentação nas grandes articulações, com o joelho e articulação coxo-femural liderando essa estatística. Apresenta-se de forma insidiosa, com intenso processo inflamatório, que em 80% dos casos é mono articular. O presente trabalho relata um caso clínico em uma criança, do sexo masculino, leucoderma, de seis anos de idade, que evoluía com dor, edema e eritema em região da ATM direita, bem como limitação dos movimentos mandibulares de abertura, fechamento e lateralidade bilateral. Possuía histórico de artrite reumatóide. Aborda-se também neste trabalho diagnósticos diferenciais e medidas terapêuticas para esta rara entidade nosológica. Aspectos referentes à antibioticoterapia e exames de imagens também são abordados.
Termos de indexação: Artrite infecciosa. Infecção. Transtornos da articulação temporomandibular.
INTRODUCTION
Septic arthritis is a form of acute arthritis caused by the presence of a microbial pathogen within the joint. It is characterized by insidious onset and a marked inflammatory process, and is monoarticular in 80% of cases. In this condition, the causative microorganism usually reaches the joint via hematogenous seeding. Less commonly, the pathogen enters the joint through a skin lesion or spreads from adjacent osteomyelitis. Inflammatory infiltrate and pus may compress intra-articular vessels, thus reducing circulation to the cartilage and subchondral bone. Pressure within the joint may also induce necrosis of articular structures1.
After entering the joint, the bacteria colonize the synovial membrane, produce an acute inflammatory response, and reach the synovial fluid. Pro-inflammatory cytokines are produced in response to the bacterial insult, intensifying the inflammatory response. The byproducts of inflammation can rapidly destroy the synovial membrane and collagen matrix, thus inhibiting cartilage synthesis. As the infection progresses, signs of inflammation (such as redness and edema) may appear2.
Septic arthritis affects 2–10 in 100,000 individuals and is most common in children, particularly under 3 years of age. The most common causative agent in children is Haemophilus influenzae type B. However, with the increasing prevalence of community-acquired methicillinresistant Staphylococcus aureus, septic arthritis caused by this organism is on the rise. Rheumatoid arthritis or osteoarthritis, systemic lupus erythematosus, diabetes mellitus, chronic kidney disease, replacement arthroplasty, skin and soft tissue infections, immunosuppression, alcoholism, and intra-articular injection of corticosteroids are predisposing factors for septic arthritis. The prognosis is guarded in older adults and those with prosthetic joints3.
The clinical manifestations of septic arthritis are pain (dolor), heat (calor), redness (rubor), and limited range of joint motion. Intense pain not relieved by rest is strongly characteristic of this condition. The signs and symptoms usually persist for 2 weeks and may regress thereafter, depending on the virulence of the causative agent and on the patient's immune status. The large joints are more often involved, with the knees and hip most commonly affected4.
Certain subgroups of children are particularly predisposed to septic arthritis, namely, neonates, children with hemophilia (due to hemarthrosis), and the immunocompromised. In adults, Staphylococcus aureus is the leading causative agent. Anaerobes are more common in elderly and immunocompromised patients, as well as when a history of trauma is present5.
The cell count can be used to distinguish inflammation from infection. Polymorphonuclear leukocyte counts below 50,000 mm3 indicate a lower likelihood of infection, but cannot rule it out completely. The goldstandard method for diagnosis of septic arthritis is to examine the synovial fluid for causative microorganisms. Cultures are more sensitive than Gram staining, which is positive in only 50% of cases6.
Juvenile rheumatoid arthritis, or juvenile idiopathic arthritis, is a chronic inflammatory autoimmune disease. It is not fatal, but if left untreated, can cause lifelong debilitating complications, potentially resulting in loss of normal function of a limb or even inability to walk, thus making children completely dependent on their families for the activities of daily living7.
Fever, rash, lymphadenopathy, hepatosplenomegaly, pericarditis, pleuritis, and arthritis per se are the major manifestations of this condition8.
Septic arthritis of the temporomandibular joint (TMJ) is an uncommon disease entity. The TMJ may be affected as a consequence of local extension of an infectious process, or secondary to hematogenous spread of a systemic infection. The microorganisms most commonly implicated are Staphylococcus aureus and Streptococcus species9.
Diagnosis is based on a combination of clinical data, imaging findings, and microbiological testing. The clinical picture of septic arthritis of the TMJ consists of fever and localized pain, especially when attempting to move the jaw. There may also be pre-auricular erythema, localized lymphadenopathy, trismus, and lateral deviation of the mandible. The imaging modalities of choice are computed tomography (CT) and magnetic resonance imaging (MRI). MRI and CT can detect joint abnormalities earlier than conventional radiography. Aspiration of the joint and Gram staining of the fluid thus obtained are essential for identification of the causative pathogen.
The treatment of choice is antibiotic therapy and arthrocentesis of the TMJ as needed. The purpose of treatment is to prevent ankylosis and extension of the infectious process to adjacent structures (cranial nerves VIII-XII, jugular vein thrombosis, skull base osteomyelitis)10.
CASE REPORT
A 6-year-old white male presented to the emergency department with a 1-week history of spiking fevers (peak temperature 38.5 °C), with only transient improvement provided by antipyretics. The patient exhibited enlargement and tenderness of the right TMJ region, as well as limited range of mouth opening and pre-auricular erythema ipsilaterally (Figure 1). The external auditory canal was free of inflammatory or purulent secretion. There was no limitation of neck flexion or extension. According to the patient's mother, he had been receiving amoxicillin since symptom onset, with no improvement. The patient was admitted with a nonspecific diagnostic hypothesis of "lymphadenitis" and prescribed empiric antibiotic therapy (intravenous clindamycin). Fever persisted, peaking at 40.5°C, and was controlled with paracetamol and ibuprofen. There was no effusion in any other peripheral joint. The patient had no history of otitis media, mastoiditis, or trauma to the neck or facial region. However, he had been previously diagnosed with rheumatoid arthritis.

Ultrasonographic examination of the TMJ and right temporal fossa revealed a 0.7-mm hypoechoic fluid level in the temporal fossa, extending into the right zygomatic arch, as well as fluid within the right TMJ. These findings were consistent with septic arthritis. There was reactive lymphadenopathy of the parotid and cervical lymph nodes.
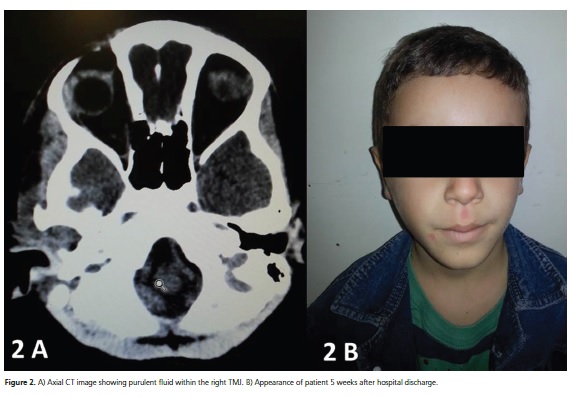
CT confirmed the finding of fluid within the right TMJ (Figure 2A).
Arthrocentesis of the right TMJ yielded purulent fluid, which was sent for culture and antibiotic susceptibility testing. The aspirate tested positive for Staphylococcus aureus (a finding consistent with the literature) sensitive to vancomycin, which was being administered since the second hospital day. The usual vancomycin dosage for children is 10 mg/kg IV every 6 hours. Laboratory characterization of Staphylococcus aureus was achieved by Gram staining (G+) and the catalase test (catalasenegative). Of all Staphylococcus species, S. aureus is the most important. It is the second leading cause of infections in humans. S. aureus is present in the upper respiratory tract (particularly in the nares) of approximately 60% of the healthy population, and does not cause disease under normal conditions. Five weeks after hospital discharge, our patient had made a complete recovery, with no evidence of abnormalities in the previously affected joint (Figure 2B).
DISCUSSION
CT scans may sometimes reveal an effusion within the temporomandibular joint. In pediatric patients, this finding has been reported as a consequence of ankylosing spondylitis, juvenile rheumatoid arthritis, trauma, nonspecific septic arthritis, ganglion cyst, synovial chondromatosis, infections of various origins, and malignancy4,6.
Septic arthritis of the TMJ most commonly occurs as the result of hematogenous spread of microorganisms from a remote primary site. TMJ infection may also spread from adjacent soft tissues, as in cases of septic arthritis secondary to mastoiditis, middle ear disease, or blunt trauma to the area. The most commonly implicated microorganism is Staphylococcus aureus. Aspiration of joint fluid for culture confirms the diagnosis in 60% of cases. Juvenile rheumatoid arthritis frequently involves arthritis of the cervical spine (C2/C3) and TMJs. In children, TMJ arthritis is usually painless and not associated with edema. TMJ monoarthritis as the sole presenting manifestation of juvenile rheumatoid arthritis is exceedingly rare. Therefore, chronic arthritis is a rare finding in a child with no signs of inflammation in other joints, particularly considering the rapid resolution of the effusion with anti-inflammatory and antibiotic therapy7.
The TMJ may be infected via hematogenous spread or by extension of a local septic focus (such as the oral cavity or ear). As the synovial fluid is highly vascularized and not bounded by any membrane, it is extremely vulnerable to infection via the former route. Predisposing factors for the development of TMJ arthritis include trauma, preexisting joint disease, burns, and conditions associated with immunosuppression, such as diabetes, rheumatoid arthritis, alcoholism, and corticosteroid therapy. The patient reported herein had been previously diagnosed with rheumatoid arthritis.
Blood cultures are less sensitive, and are positive in only 40% of cases. In some cases, less common microorganisms are found, such as Pseudomonas aeruginosa, although its true pathogenic role is unclear. When Pseudomonas aeruginosa is confirmed as the causative organism, arthritis is usually attributable to local extension of an ear infection, which was ruled out in our patient8,10.
Hypersensitivity reactions to vancomycin have been reported, including maculopapular rash and anaphylaxis. Phlebitis and pain at the injection site are unusual. Chills, fever, and a shock-like reaction may occur during the intravenous infusion. The most significant adverse reactions involve ototoxicity and nephrotoxicity. Our patient did not experience any adverse reaction to vancomycin.
CONCLUSION
Septic arthritis of the TMJ usually occurs as a complication of head and neck infections. Its course usually involves substantial morbidity, and the outcome may be fatal. Early diagnosis is generally associated with a more benign progression. Imaging modalities, such as CT, allow early diagnosis and confirmation of suspected cases, which, in turn, enables institution of proper treatment and prevents potentially harmful consequences. Special attention should be given to the clinical history and physical examination (locoregional and general), which may provide clues as to the primary focus of infection and guide the selection of initial empiric antibiotic therapy.
Collaborators
HHA MORAIS, TS PEIXOTO, JC BARBALHO, TGS DIAS, RJH VASCONCELLOS and ES LUCENA were responsible for the conduct of the case, review and article writing.
REFERENCES
1. Pintor F, Carrasco R, Verdugo F, Landaeta M. Artritis infecciosa de la articulación temporomandibular consecutivo a otitis necrotizante: reporte de un caso. Rev Med Chile. 2015;143(6):805-8. doi: 10.4067/S0034-98872015000600015 [ Links ]
2. Cai XY, Yang C, Zhang ZY, Qiu WL, Chen MJ, Zhang SY. Septic arthritis of the temporomandibular joint: a retrospective review of 40 cases. J Oral Maxillofac Surg. 2010;68(4):731-8. doi: 10.1016/j.joms.2009.07.060
3. Bakhos D, Trijolet J, Morinieri S, Pondaven S, Al Zahrani M, Lescanne E. Conservative management of acute mastoiditis in children. Arch Otolaryngol Head Neck Surg. 2011;137(4):346- 50. doi: 10.1001/archoto.2011.29
4. Varghese L, Chacko R, Varghese GM, Job A. Septic arthritis of the temporomandibular joint caused by Aspergillus flavus infection as a complication of otitis externa. Ear Nose Throat J. 2015;94(3):E24-6.
5. Leighty SM, Spach DH, Myall RW, Burns JL. Septic arthritis of the temporomandibular joint: review of the literature and report of two cases in children. Int J Oral Maxillofac Surg. 1993;22(5):292-7.
6. Thomson HG. Septic arthritis of the temporomandibular joint complicating otitis externa. J Laryngol Otol. 1989;103(3):319-21.
7. Galvan N, Middleton JR, Cook C, Britt LG, Kuroki K. Otitis interna, media, and externa with destruction of the left tympanic bulla and subluxation and septic arthritis of the left temporomandibular joint in an alpaca (Vicugna pacos). Can Vet J. 2013;54(3):283-5.
8. Sembronio S, Albiero AM, Robiony M, Costa F, Toro C, Politi M. Septic arthritis of the temporomandibular joint successfully treated with arthroscopic lysis and lavage: case report and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103(2):e1-6.
9. Kito S, Hirashima S, Yoshioka I, Habu M, Kodama M, Kokuryo S, et al. A case of chronic infectious arthritis of the temporomandibular joint associated with osteomyelitis without malocclusion. Open Dent J. 2010;4:29-32. doi: 10.2174/1874210601004010029
10. Arabshahi B, Baskin KM, Cron RQ. Reactive arthritis of the temporomandibular joints and cervical spine in a child. Pediatr Rheumatol Online J. 2007;5:4. doi: 10.1186/1546-0096-5-4.
 Correspondence to:
Correspondence to:
HHA MORAIS
Rua André Sales, 667, Paulo XI
59300-000, Caicó, RN, Brasil
e-mail: heciomorais@hotmail.com
Received on: 27/8/2015
Final version resubmitted on: 29/2/2016
Approved on: 3/3/2016
