










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.64 no.3 Porto Alegre Jul./Set. 2016
ORIGINAL / ORIGINAL
Performance in vitro of apex locators in determining root length in primary molars
Desempenho in vitro de localizadores apicais na determinação de comprimento radicular em molares decíduos
Fernanda Mara Paiva BERTOLII; Carolina Dea BRUZAMOLINI; Flares BARATTO FILHOI; Débora Andrade da SILVAI; Flávia Fagundes Sens TOMAZINHOI; Carla Castiglia GONZAGAI ; Juliana Feltrin de SOUZAII
I Universidade Positivo, Programa de Pós-Graduação em Odontologia Clínica. Curitiba, PR, Brasil
II Universidade Federal do Paraná, Faculdade de Odontologia, Departamento de Estomatologia
ABSTRACT
Objective
The aim of the study was to evaluate performance of digital radiographic and two electronic apex locators, Propex II and Root ZX in root canal length determination in primary molars.
Methods
25 primary molars were divided into two groups, G1 without root resorption and G2 with root resorption. The exams were performed using all methods by two experienced examiners, with 1-week interval. The gold standard was determined by visual examination. The methods were statistically analyzed regarding the values of reproducibility and correlated with the gold standard by Pearson´s correlation coefficient.
Results
The root canal length determination coincided with gold standard in 22.7% for Root ZX, 17.5% for Propex II and 12.5% for digital radiography. Correlation values were higher in G1, the Root ZX presented the highest values. In G2 the digital radiography showed the lowest correlation. In G1, the intra-examiner reproducibility values ranged from 0.925 to 0.523, and interexaminer 0.863 to 0.670. In G2, the values of intraexaminer reproducibility ranges from 0.864 to 0.097, and inter was 0.774 to 0.379.
Conclusion
It was concluded that the methods performance varying according to examiner's experience. The Root ZX presented the highest reproducibility and accuracy.
Indexing terms: Apex locator. Digital radiography. Endodontics. Primary teeth. Root ZX.
RESUMO
Objetivo
Avaliar o desempenho in vitro de radiografia digital e de dois localizadores apicais eletrônicos, Propex II e Root ZX na determinação do comprimento de canal em molares decíduos.
Métodos
Foram selecionados 25 molares decíduos divididos em dois grupos, G1, sem reabsorção radicular e G2 com reabsorção radicular. Os exames foram realizados utilizando todos os métodos por dois examinadores experientes, com intervalo de 1 semana. O padrão ouro foi determinada por exame visual. Os métodos foram analisados estatisticamente em relação aos valores de reprodutibilidade e correlacionada com o padrão ouro pelo coeficiente de correlação de Pearson.
Resultados
A determinação de comprimento de canal coincidiu com padrão-ouro em 22,7% para o Root ZX, 17,5% para Propex II e 12,5% para a radiografia digital. valores de correlação foram maiores no G1, o Root ZX apresentou os maiores valores. Em G2 da radiografia digital apresentou a menor correlação. No G1, os valores de reprodutibilidade intra-examinador variou 0,925-0,523 e interexaminadores 0,863- 0,670. No G2, os valores da reprodutibilidade intra-examinador varia 0,864-0,097, e inter era 0,774-0,379.
Conclusão
Concluiu-se que o desempenho dos métodos varia de acordo com a experiência do examinador. O Root ZX apresentou maior reprodutibilidade e precisão.
Termos de indexação: Localizador apical. Radiografia digital. Endodontia. Dentes decíduos. Root ZX.
INTRODUCTION
The maintenance of the integrity of primary dentition is the major goal of pediatric dentistry, due to the proper skeletal, functional and cognitive child development, once these elements ensure chewing, speech and aesthetics1-3. Thus, endodontic treatment is necessary in order to avoid tooth extractions. Pulpectomies in primary teeth are indicated in cases of pulp necrosis or irreversible pulpits, in teeth with at least 2/3 of root. The root canal length determination is essential for the treatment success, mainly in deciduous, because the risk of permanent damage4. The most used method to determine the root length for primary teeth is the conventional and digital radiography. However, there are many limitations in this method4, such as image distortion, superposition, and the X-ray exposes the patient to ionizing radiation5.
Considering the radiographs limitations, new techniques have been investigated. The electronic apex locators (EAL) provide some advantages in determining the correct root length determination even though in pediatrics endodontics5-6. In the 80s, the EAL's first-generation based on the electrical resistance values to measure the length of the root canal7. However, these devices caused painful during measurement, probably due to cellular necrosis caused by the passage of high voltage electric current8-9. The second generation operates by measuring changes in impedance10 and the third generation, the two frequency impedance-type devices was based on different electrical principles. These values are reliable even though in the presence of pulp tissue2.
In vitro studies showed high efficacy of EAL in primary teeth, providing better quality in endodontic deciduous treatment4,11-13. Thus, the aim of this in vitro study was to compare the performance of two electronic apex locators, Propex II and Root ZX, and digital radiograph in primary molars. The study hypothesis tested was that the methods produced different performance. Moreover, there was no difference between teeth with and without physiologic resorption.
METHODS
This study was approved by the Ethics Committee in Research (report #826.335).
Teeth selection and preparation
For sample preparation 40 primary molars were used and donated by the bank of teeth of the University of São Paulo (USP). The primary molars were selected according to the following inclusion criteria: presence of complete root or root resorption less than 1/3 of the root length. Teeth with greater root resorption 1/3, internal or external resorption, and root fracture were excluded. The teeth were stored in saline solution, changed every day. The teeth were divided into two groups according to the stage of root: without root (Group 1); and roots with root resorption less than 1/3 (Group 2).
Determination of root canal length
The teeth were cleaned properly and then were performed the endodontic access cavity preparation with spherical diamond bur (1016, KG Sorensen, São Paulo, SP, Brazil), followed by channel access through endodontic files (type K File # 10, 21mm, Maillefer, Dentsply).
For determining visual root length, it was used an endodontic file type K-File # 15 inserting in the root canal with rubber stop positioned in the buccal face of the crown until it emerged at the apical foramen. The distance of the rubber stop was measured with a caliper.
For digital radiographic exam, the radiographs were made of standardized manner using digital sensor (Kodak RVG 6100) and X-ray device Gnatus XR 6010, operating at 60 kVp and 10 mA, exposure time of 0.20 seconds, and focus-film distance of 20 cm. The images were displayed through software Kodak Dental System. The image of each teeth were determined the apparent root length of each root. After this measurement, the apparent length was transferred to an endodontic file type K-File # 15, being inserted into the root canal with rubber stop positioned in the buccal face of the crown, and new digital radiographs were taken with each root. Thus, the image was analyzed and determined the root length of each root.
Previously to determining the root length by EAL, each tooth was individually placed in a standard position for apex locator (IM Brazil, Sao Paulo, Brazil) with sponge soaked in sodium hypochlorite. Propex II (Maillefer, Dentsply, Switzerland) and Root ZX (Morita, São Paulo, Brazil) were used. These methods were applied in an endodontic file type K-File # 15 was initially inserted into each root canal, when the apex locator charges, it represents that the file is in the apical foramen, the course file was slipped to the reference edge of the crown and recorded the measure as electronic length / foramen (CEF).
The methods were performed by two examiners trained and independently. Each examiner ran the measurements twice with 1-week interval.
Statistical analysis
Data were statistically analyzed using SPSS 14.0 (Statistical Package for the Social Sciences for Windows®, SPSS Inc., Chicago, IL, US). The methods were analyzed according the accuracy with the gold standard (Visual examination) by the Spearman's Rank coefficient correlation. In addition, the reproducibility of the methods was determined by the values of inter- and intra-examiner according the Intraclass Correlation Coefficient (ICC). The significance level of 5% was adopted.
RESULTS
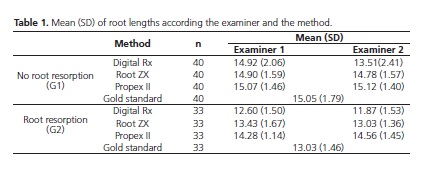
From the 40 primary molars, 73 roots were in accordance with the selection criteria, being 40 without root resorption (Group 1), and 33 roots with root resorption (Group 2). The mean of root lengths and standard deviation determined by each method from each examiner are reported in Table 1.
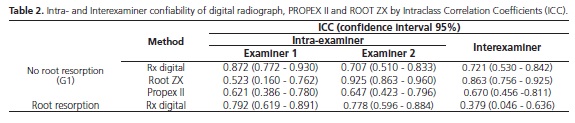
The reproducibility values are shown in Table 2. The values of intra-examiner for examiner 1 were 0.872 and 0.792 (digital Rx), 0.523 and 0.703 (Root ZX) and 0.621 and 0.097 (Propex II) in G1 and G2 respectively. Regarding examiner 2, the values values of intraexaminer were 0.707 and 0.778 (digital rx), 0.925 and 0.834 (Root ZX), and 0.647 and 0.299 (Propex II) in G1 and G2 respectively.
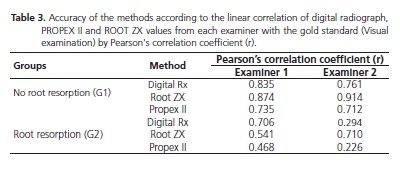
The accuracy of the methods was analyzed using Spearman's Rank coefficient correlation with the gold standard values (Table 3). It can be seen that in G1 the methods presented a strong correlation for both examiners, being Root ZX locator the most accurate method (0.874 and 0.914). In G2, Propex II presented the lowest correlation 0.468 and 0.226, for examiner 1 and 2, respectively.
Table 4 and 5 show the real difference in mm appointed from the methods to the apex (gold standard). Root ZX presented 22.5% of the sample values equal to the gold standard. The Propex II locator presented values farthest from the gold standard in G2, once 42.2% of the sample this 2.0 <d ≤3.0 apex. The digital Rx method had a higher frequency of values in negative relation from the apex, 25% of the sample (10 roots, -2.0 ≤ d <-1.0).


DISCUSSION
The apical limit determination is one of the most important factor in successful endodontic therapy to prevent under or over instrumentation, it can damage the permanent germ and, on the other hand, the under filling is a risk for infection relapse2-3,14.
There are no standardized methods for the exact measurements of the root canal length in primary teeth3, thus this study investigated the distinct methods for determining the root length in primary molars by two examiners. Although radiography method is the most used, it presented limitation in detecting minor degrees of root physiological resorption4,15. Moreover, the underposition of the structures may difficult to predict the exact root length, and this method is subjective because is extremely dependent on the professional.
In this study were used Root ZX and Propex II. Root ZX its measurements are performed by calculating the impedance quotient of two distinct frequencies (0.4 and 8.0 kHz) and show precision rates greater than 90%, even when used in unfavorable conditions, such as teeth root resorption. The propex II operates by capturing the signals of two alternating currents (0.5 and 8.0 kHz) and for this calculation, the mean square root of impedances at these two frequencies are measured separately and have a problem with the amplitude of the signal, being lesse affected by any interference in the root canal16.
Another problem for the radiograph exam is the position of the film inside the child's mouth and the exposition to radiation hazards4. Our finds demonstrated that the radiography methods noticed more difference between the examiners, mainly, due to professional experience. It can be evidenced by the interexaminer reproducibility; the digital Rx method presented a lower value in resorption group. While, the examiner 1, the most experienced have higher reproducibility (intra-examiner).
New electronic methods have been developed in order to overcome all these difficulties. There are a few studies investigating the EAL in primary dentition2-4,16. Two electronic apex locators were tested in this study, Propex II and Root ZX. The use of Root ZX exhibited, in G1, high level of agreement between the examiners in relation to other methods. On the other hand, the Propex II method had the less of agreement between the examiners, being lower than Rx digital method. Thus, these results suggest that the radiography, as a conventional method could not be replaced, however, it is known others tools to determine the root length, furthermore, the EALs also reduce radiation exposure and time care14.
Our findings demonstrated that all methods had more difficulties in resorption roots. In the group without resorption, the methods presented a strong correlation with the gold standard for both examiners. However, it was lower in root with resorption, being the Propex II method the weakest correlation tool. Other authors showed no differences between resorbed and no resorbed roots and two types of EAL (Root ZX and Endex)3,16. The Propex II presented the lower performance in this study, different from Nelson-Filho et al.12 that recommend this EAL to primary teeth. Chakravarthy Pishipati (2013) showed in permanent teeth that Root ZX and Propex II did not present significant difference in determining root length17. Patiño-Marín et al. (2011), who used the Propex II, which showed better accuracy compared to visual and radiographic method18. The studies can notice different results due to the methodology differences, such as tools and teeth studied.
Considering the difference of the measures from the apex, Root ZX had the highest frequency of real root length in G1 (22.5%) and G2 (18.2%), moreover within ±0.5 and ±1 mm the accuracy of Root ZX in G1 was 72.5% and 85% respectively, and in G2 was 54.7% and 72.9%, better results than Bodur et al.3 was 54.9% and 70.6% in no resorption roots and 25.8% and 63.4% in resorption roots. Beltrame et al.19 observed accuracy of ±0.5 mm 69% and 65% of the canals in roots without and with resorption, respectively using Root ZX. The studies showing that Root ZX and Root ZX II are the most common EALs used in primary teeth3,14,19-20. This is an electronic canal length measuring device based on the ratio method, which simultaneously measures impedance values at two frequencies (8 KHz and 0.4 KHz) and calculates a quotient of impedances2.
Andrade et al.6 and Barololoomi et al.21 compared the use apex locator Root ZX with the visual and radiographic methods in primary teeth. The authors found that the locator presented higher values and accuracy to the location of the apical foramen of teeth either with or without resorption. Faced with this, the electronic method may be useful in the effectiveness and for the success of endodontic treatment in primary teeth.
If the root length wasn't accurately measured, the endodontic treatment can be failure, which can result in overinstrumentation or underinstrumentation. In our results, in both groups (with our without resorption), the Root ZX showed to be the most accurate method. On the other hand, the radiographic was less accurate method, presenting values under from the apex, while, Propex showed values over from the apex. Regarding primary teeth, overinstrumentation and overfilling can be damage, once it can affect the germ of permanent tooth. Moreover, underintrumentation/underfilling can be increasing the failure risk2.
Although, the EAL using Root ZX is a good method to determine the root length, radiographic image provide an observation of a number of anatomical details2. Thus, the EAL could be applied to complement the conventional exam (radiograph) in determining the root lengths and resorption.
A limitation of the present study is an in vitro design, thus this results can be interpreted with care when it is extrapolled for in vivo measurements. It can be concluded that the presence of resorption affected the performance of the methods. The Root ZX may be recommended for use for determining the root length of primary teeth, which can be applied in association with conventional diagnostic measures, such as radiograph, for examiners no trained for its use. Further, in vivo evaluations of these devices in primary teeth should be carried out of different electronic apex locators available commercially.
Collaborators
FMP BERTOLI and CD BRUZAMOLIN have substantial contributions to the design of the study and its approval by the Committee for Ethics in Research, data acquisition and interpretation of data, and wrote the paper. F BARATTO-FILHO performed statistical analysis, wrote and revised the paper. DA SILVA was also responsible for interpretation of data and wrote the paper. FFS TOMAZINHO contributed to the design of the study and its approval by the Committee for Ethics in Research and interpretation of data. CC GONZAGA performed the study design and contributed to its approval by the Committee for Ethics in Research and wrote the paper. SJF SOUZA also contributed to the design of the study and its approval by the Committee for Ethics in Research, statistical analysis, interpretation of data and revised the final version to be published.
REFERENCES
1. Pinheiro SL, Araujo G, Bincelli I, Cunha R, Bueno C. Evaluation of cleaning capacity and instrumentation time of manual, hybrid and rotary instrumentation techniques in primary molars. Int Endod J. 2012;45(4):379-85. doi: 10.1111/j.1365- 2591.2011.01987.x [ Links ]
2. Leonardo MR, Silva LA, Nelson-Filho P, Silva RA, Raffaini MS. Ex vivo evaluation of the accuracy of two electronic apex locators during root canal length determination in primary teeth. Int Endod J. 2008;241(4):317-21. doi: 10.1111/j.1365- 2591.2007.01366.x
3. Bodur H, Odabas M, Tulunoglu O, Tinaz AC. Accuracy of two different apex locators in primary teeth with and without root resorption. Clin Oral Investig. 2008;12(2):137-41. doi: 10.1007/s00784-007-0157-5
4. Silva EJ, Herrera DR, Souza-Júnior EJ, Rosa TP. Evaluation of the multifrequency electronic apex locator Joypex 5 in primary teeth. Eur Arch Paediatr Dent. 2014 Feb;15(1):51-4. doi: 10.1007/s40368-013-0065-0
5. Chita JJ, Silva PGD, Pereira KFS, Onoda HK, Junior JDCB, Ramos CAS. Precisão e confiabilidade de um novo localizador foraminal eletrônico: estudo in vivo. Pesq Bras Odontoped. 2012;12(4):7.
6. Andrade A, Silva S, Imparato J, Duarte DA, Bueno C, Cunha RS. Viability of Artificial Primary Teeth for Electronic Working Length Determination. Pesq Bras Odontoped Clin Integr. 2013;3(1):83-7.
7. Silva TMD, Alves FRF. Localizadores apicais na determinação do comprimento de trabalho: a evolução através das gerações. Rev Bras Odontol. 2011;68(2):6.
8. Ushiyama J. New principle and method for measuring the root canal length. J Endod. 1983 Mar;9(3):97-104. doi: 10.1016/ S0099-2399(83)80105-8
9. O'Neill LJ. A clinical evaluation of electronic root canal measurement. Oral Surg, Oral Med Oral Pathol. 1974;38(3):469- 73. doi: 10.1016/0030-4220(74)90376-4
10. Kim YJ, Chandler NP. Determination of working length for teeth with wide or immature apices: a review. Int Endod J. 2013; 46(6):483-91.
11. Krishnan IS, Sreedharan S. A comparative evaluation of electronic and radiographic determination of root canal length in primary teeth: an in vitro study. Contemp Clin Dent. 2012;3(4):416-20.
12. Nelson-Filho P, Luciano MP, Leonardo MR, da Silva RA, da Silva LA. Electronic working length determination in primary teeth by propex and digital signal processing. Aust Endod J. 2010;36(3):105-8.
13. Kaufman AY, Keila S, Yoshpe M. Accuracy of a new apex locator: an in vitro study. Int Endod J. 2002; 35(2):186-92. doi: 10.1046/j.1365-2591.2002.00468.x
14. Ahmed HM. Anatomical challenges, electronic working length determination and current developments in root canal preparation of primary molar teeth. Int Endod J. 2013;46(11):1011-22. doi: 10.1111/iej.12134
15. Kielbassa AM, Muller U, Munz I, Monting JS. Clinical evaluation of the measuring accuracy of ROOT ZX in primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003;95(1):94- 100. doi: 10.1067/moe.2003.99
16. Angwaravong O, Panitvisai P. Accuracy of an electronic apex locator in primary teeth with root resorption. Int Endod J. 2009;42(2):115-21. doi: 10.1111/j.1365-2591.2008.01476.x
17. Chakravarthy Pishipati KV. An In vitro comparison of propex ii apex locator to standard radiographic method. Iran Endod J. 2013;8(3):114-17. doi: 10.1097/00004770-200202000- 00017
18. Patino-Marin N, Zavala-Alonso NV, Martinez-Castanon GA, Sanchez-Benavides N, Villanueva-Gordillo M, Loyola-Rodriguez JP. Clinical evaluation of the accuracy of conventional radiography and apex locators in primary teeth. Pediatr Dent. 2011;33(1):19-22.
19. Beltrame AP, Triches TC, Sartori N, Bolan M. Electronic determination of root canal working length in primary molar teeth: an in vivo and ex vivo study. Int Endod J. 2011;44(5):402- 6. doi: 10.1111/j.1365-2591.2010.01839.x
20. Carvalho AL, Moura-Netto C, Moura AA, Marques MM, Davidowicz H. Accuracy of three electronic apex locators in the presence of different irrigating solutions. Braz Oral Res. 2010;24(4):394-8. doi: 10.1590/S1806-83242010000400004
21. Bahrololoomi Z, Soleymani AA, Modaresi J, Imanian M, Lotfian M. Accuracy of an Electronic Apex Locator for Working Length Determination in Primary Anterior Teeth. J Dent. 2015;12(4):243-8. J Dent (Tehran). 2015;12(4):243-8.
 Correspondence to:
Correspondence to:
JF SOUZA
Av. Prefeito Lothário Meissner, 632
80210-170, Curitiba, PR, Brasil
e-mail: julianafeltrin@hotmail.com
Received on: 29/4/2016
Final version resubmitted on: 11/5/2016
Approved on: 29/6/2016
