










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRGO.Revista Gaúcha de Odontologia (Online)
versão On-line ISSN 1981-8637
RGO, Rev. gaúch. odontol. (Online) vol.64 no.4 Porto Alegre Out./Dez. 2016
CLÍNICO / CLINICAL
Goldenhar Syndrome in a pediatric patient: a case report and review of literature
Síndrome de Goldenhar em um paciente infantil: relato de caso e revisão da literatura
Mauro Antonio Dall AGNOLI; Amy Louise BROWNII;Luiz Alexandre THOMAZII; José Luiz Cintra JUNQUEIRAIII; Luciana Butini OLIVEIRAII
I Universidade Comunitária da Região de Chapecó – UNOCHAPECÓ, Curso de Odontologia
II Faculdade São Leopoldo Mandic, Curso de Odontologia, Programa de Pós-Graduação em Odontologia. Campinas, SP, Brasil
ABSTRACT
Goldenhar Syndrome is a rare, generally sporadic condition, whose physical manifestations include asymmetric incomplete facial development, epibulbar dermoids, auricular malformations e auricular appendices, vertebral anomalies, central nervous system disturbances, ocular irregularities and visceral abnormalities. Its etiology is not fully understood, with its incidence ranging from 1:3500 to 1:5600 live births, and a gender ratio of 3:2 (male: female), presenting more frequently in children with congenital deafness. The purpose of this case report was to describe clinical presentation of Goldenhar syndrome in a five-year old male with no significant family history, where almost all of the classic signs of the condition were present. Considering its involvement in craniofacial structures, its rarity, and its wide spectrum of symptoms and associated systemic abnormalities, knowledge of this condition is paramount for the dental surgeon.
Indexing terms: Craniofacial abnormalities. Diagnosis. Goldenhar syndrome.
RESUMO
A Síndrome de Goldenhar é rara e suas principais manifestações físicas incluem assimetria e desenvolvimento facial incompleto, tumores dermoides epibulbares, malformações na orelha e apêndices auriculares, anomalias vertebrais, distúrbios no sistema nervoso central, irregularidades oculares e anomalias viscerais. A etiologia desta condição não é claramente esclarecida e apresenta-se geneticamente variável. A incidência da Síndrome de Goldenhar pode variar de 1:3500 até 1:5600 nascidos vivos e relação por sexo de 3:2 (masculino: feminino), apresentando mais frequentemente em crianças com surdez congênita. O objetivo deste trabalho é apresentar um caso clínico de Síndrome de Goldenhar em paciente infantil de 5 anos de idade do sexo masculino, sem história familiar relevante relacionada à síndrome e que apresenta características claras desta condição. Considerando o envolvimento das estruturas craniofaciais da Síndrome de Goldenhar, sua raridade e o amplo espectro de sintomas e anormalidades sistêmicas associadas, o conhecimento desta condição é primordial para o cirurgião-dentista.
Termos de indexação: Anormalidades craniofaciais. Diagnóstico oral. Síndrome de Goldenhar.
INTRODUCTION
Goldenhar syndrome, also known as Oculo- Auriculo-Vertebral Spectrum (OAVS), lateral facial dysplasia, Goldenhar complex or first and second branchial arch syndrome1, is a rare condition that was first described in the early 1950s2.
It is considered a variant of craniofacial (hemifacial) microsomia (CFM), a group of congenital malformations that occur during the embryonic development of the first and second branchial arches, which give rise to the ear, face and eyelids3-5. Therefore, patients present with the classic signs of CFM, such as unilateral asymmetric incomplete facial development, which may affect the mandible, maxilla, ears, soft tissues and nerves, as well as epibulbar dermoids and vertebral anomalies6-7.
The incidence of Goldenhar syndrome ranges from 1:3500 to 1:5600 live births, with a gender ratio of 3:2 (male:female), presenting more frequently in children with congenital deafness, at a rate of approximately 1:1000 live births8-9. Although its etiology is not yet fully understood, it has been postulated that an abnormal embryonic vascular supply, or disruption to the mesoderm, among other factors, may lead to a defective formation of the branchial arches10.
Although most cases are sporadic, the presence of an autosomal dominant genetic marker, as well as multifactorial heredity have been suggested. However, while some chromosomal studies have not revealed any specific genetic abnormalities, it has been suggested that the 22q11 locus contains important genes that may influence regulatory signaling events in the development of the pharyngeal arch, which could potentially contribute to craniofacial dysmorphism11.
The use of drugs such as thalidomide, retinoic acid, tamoxifen and cocaine during pregnancy have been suggested as risk factors for the development of this syndrome, while gestational diabetes, rubella and influenza have also been proposed as potential etiological factors12-13.
Taking into consideration its involvement in the formation of craniofacial structures, its rarity, its vast spectrum of physical characteristics and potential associated systemic abnormalities, knowledge of Goldenhar syndrome is paramount for dental surgeons14.
Therefore, the present study reports a case of Goldenhar syndrome in a five-year-old male, with no significant family history, where almost all of the classic signs of the condition were present. Early diagnosis and management of Goldenhar syndrome by pediatric dentists can have a significant impact on the health of affected children.
CASE REPORT
A 5-year-old male was referred to the Pediatric Dental Clinic of São Leopoldo Mandic Dental School, Campinas, Brazil, seeking advice regarding dental treatment. The mother described an unrelenting need for dental treatment, with the chief complaint being "rotten teeth".
The patient medical history revealed consultations with neurologists, cardiologists, otolaryngologists and orthopedic surgeons, as well as sessions with speech and language therapists. A congenital heart defect was also reported (ventricular septal deviation, VSD), which was corrected surgically.
The family history was unremarkable, with the patient's siblings reported as healthy and without any congenital malformations. No teratogenic medications, alcohol or illicit drugs were used during pregnancy. The patient was born at term by caesarean section, and was considered appropriate for gestational age. Breastfeeding continued until 45 days of life, where formula milk was then introduced.
General examination revealed a mild scoliosis, with the presence of cuneiform vertebrae. Asymmetry of the face with unilateral CFM (left-sided) as well as hypoplasia of the muscles of mastication and facial expression, and the mandible, maxilla and zygomatic bones was observed. Unilateral (left-sided) macrostomia with excessive extension of the labial commissure (lateral extension of the angle of the mouth in a cleft fashion), which had undergone surgical repair (Figure 1), was also observed.
Micrognathia, left maxillary and mandibular hypoplasia and subsequent dental malocclusion, with the presence of cross-bite and open bite, and incomplete lip seal were also observed. In addition, an obvious nasal septum deviation was detected.

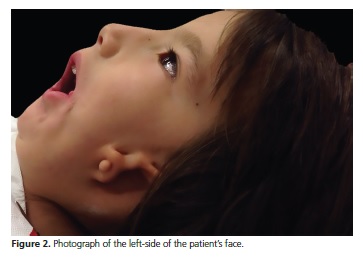
Microtia, pre-auricular skin tags and a narrow auditory canal were also observed on the left side (Figure 2), with a diagnosis of partial deafness established by an otolaryngologistist. A small coloboma and a convergent strabismus were observed in the left eye.
His dental history, began at six months of age, reporting regular visits to the dentist (ever four months, on average). The mother reported a high intake of sweets by the patient, which may explain the presence of multiple active caries lesions found during intraoral examination.
Clinical examination revealed the presence of a mixed dentition, compatible with the patient's age, and a sharp deviation from the dental midline were also observed.
Periapical radiographs also revealed multiple caries lesions, as well as the morphology of the primary dentition, which also demonstrated physiological root resorption.
Panoramic radiography (OPG) confirmed the mixed dentition and, also revealed morphological changes in the coronoid process of the mandible and absence of the left condyle, with hypoplasia of this region showing reduced thickness of the ascending limb, in addition to irregularities in the supporting structures of the teeth. It is important to highlight that technical difficulties were encountered during radiographic acquisition due to the difficulties in immobilizing the patient within the equipment. Periapical radiography emphasized the maxillary atresia observed on the left side (Figure 3).
The information described in this case report was obtained from details provided by the mother, as well as from clinical, radiological and photographic data from the medical and dental records.

DISCUSSION
Reporting of individual case reports has heavily influenced the history of dentistry and its scientific development. Sharing of individual experiences, discussions on diagnosis and treatment plans, and the presentation of patients for intra-professional learning have been considered excellent strategies for spreading knowledge between professionals.
The patient described, herein, presented with clinical features compatible with Goldenhar Syndrome, showing manifestations of the classic triad of ocular, auricular and vertebral signs, associated with facial and cardiac malformations15-17.
Facial asymmetry, characteristic of CFM, with the presence of mandibular hypoplasia, a small coloboma, and preauricular skin tags, were observed. The patient also presented vertebral defects and congenital heart disease (VSD), consistent with the description of associated anomalies described in the literature, the prevalence, of which, is reported as varying between 5 and 58%18-19.
The presence of syndromes that manifest in craniofacial malformations, particularly those that affect the oral cavity, require not only a prompt and precocious diagnosis, but also strict planning by a multidisciplinary team to prioritize and screen for potentially serious events20-21, a finding that was observed in the present clinical case.
In addition, associated cardiac and renal manifestations, which are often present in this syndrome, require treatment with the appropriately trained team22-23, as demonstrated in this report by the surgical intervention for the VSD.
Auricular malformations and partial deafness (unilateral), as well as speech and language therapies, provided by specialists in otorhinolaryngology and speech therapy, are also paramount for the development of the affected individual.
It is important to highlight that, according to Brosco et al.24 only 6% of patients with Goldenhar syndrome manifesting with unilateral auricular malformations reported hearing loss in the contralateral ear. This finding was corroborated by the current report, which describes deafness on the left side only.
Gorlin et al.25 reported that 40 to 60% of patients with Goldenhar syndrome may have wedge-shaped vertebrae, spina bifida, scoliosis, synostosis or fusion of several vertebrae or semi-vertebrae. Therefore, the presence of anomalies of the vertebral column is now considered characteristic of this condition. In agreement with the aformentioned statistics, several abnormal vertebrae, as well as a mild scoliosis, were observed in the current case report.
One must not neglect the role of the dental surgeon in cases such as described herein. A precarious oral condition may compromise other treatment approaches necessary by the multidisciplinary team, once again reiterating the importance of inter-professional working relationships.
In order to correct the malformations of the face and jaws, a team consisting of maxillofacial and plastic surgeons, along with orthodontists are required. The aim of treatment is to achieve a well functioning and esthetically pleasing outcome, allowing the patient to lead as close to a normal life as possible.
CONCLUSION
In conclusion, a critical analysis of the current case and comparison with the literature allows one to conclude that the craniofacial malformations presented in this report are of paramount importance for dental surgeons. In addition, knowledge of its clinical characteristics and systemic manifestations are necessary in order to achieve a satisfactory outcome, both functionally and esthetically. Additionally, treating these patients in a multidisciplinary team will allow timely interventions that will provide the most benefit to these patients.
Collaborators
MAD AGNOL and LA THOMAZ assisted the patient and in writing the draft of the paper. AL BROWN, JLC JUNQUEIRA and LB OLIVEIRA critically revised and wrote the paper. All authors approved the final version to be published.
REFERENCES
1. Goldenhar, M. Associations malformatives de l'oeil et de l'oreille, en particulier le syndrome dermoïde epibulbaire-appendices auriculaires-fistula auris congenita et ses relations avec la dysostose mandibulo-faciale. J Genet Hum. 1952;1: 243-82. [ Links ]
2. Converse JM, Coccaro PJ, Becker M, Wood-Smith D. On hemifacial microsomia. The first and second branchial arch syndrome. Plast Reconstr Surg. 1973;51:268-79.
3. Lam CH. A theory on the embryogenesis of oculo-auriculo-vertebral (Goldenhar) syndrome. J Craniofac Surg. 2000;11(6):547-52.
4. Monahan R, Seder K, Patel P, Alder M, Grud S, O'Gara M. Hemifacial microsomia. Etiology, diagnosis and treatment. J Am Dent Assoc. 2001;132(10):1402-8. doi: 10.14219/jada. archive.2001.0055
5. Tuin J, Tahiri Y, Paliga JT, Taylor JA, Bartlett SP. Distinguishing Goldenhar Syndrome from Craniofacial Microsomia. J Craniofac Surg. 2015;26(6):1887-92. doi: 10.1097/ SCS.0000000000002017
6. Lessick M, Vasa R, Israel J. Severe manifestations of oculoauriculovertebral spectrum in a cocaine exposed infant. J Med Genet. 1991;28:803-4.
7. Sant'Anna EF, Lau GW, Marquezan M, de Souza Araújo MT, Polley JW, Figueroa AA. Combined maxillary and mandibular distraction osteogenesis in patients with hemifacial microsomia. Am J Orthod Dentofacial Orthop. 2015;147(5):566-77. doi: 10.1016/j. ajodo.2014.12.027
8. McCarthy JG. The role of distraction osteogenesis in the reconstruction of the mandible in unilateral craniofacial microsomia. Clin Plast Surg. 1994;21:625-31.
9. Senggen E, Laswed T, Meuwly JY, Maestre LA, Jaques B, Meuli R, et al. First and second branchial arch syndromes: multimodality approach. Pediatr Radiol 2011;41(4):549-61. doi: 10.1007/ s00247-010-1831-3
10. Hartsfield JK. Review of the etiologic heterogeneity of the oculoauriculo- vertebral spectrum (Hemifacial Microsomia). Orthod Craniofac Res. 2007;10: 121-8.
11. Beleza-Meireles A, Hart R, Clayton-Smith J, Oliveira R, Reis CF, Venâncio M, et al. Oculo-auriculo-vertebral spectrum: clinical and molecular analysis of 51 patients. Eur J Med Genet. 2015;58:455- 65.
12. Kumar R, Balani B, Patwari AK, Anand VK, Ahuja B. Goldenhar syndrome with rare associations. Indian J Pediatr. 2000;67:231-3.
13. Ewart-Toland A, Yankowitz J, Winder A, Imagire R, Cox VA, Aylsworth AS, et al. Oculoauriculovertebral abnormalities in children of diabetic mothers. Am J Med Genet. 2000;90:303-9.
14. Pinheiro AL, Araújo LC, Oliveira SB, Sampaio MC, Freitas AC. Goldenhar's syndrome--case report. Braz Dent J. 2003;14(1):67- 70. doi: 10.1590/S0103-64402003000100013
15. Hennersdorf F, Friese N, Löwenheim H, Tropitzsch A, Ernemann U, Bisdas S. Temporal bone changes in patients with Goldenhar syndrome with special emphasis on inner ear abnormalities. Otol Neurotol. 2014;35(5):826-30. doi: 10.1097/ MAO.0000000000000278
16. Martelli H Jr, Miranda RT, Fernandes CM, Bonan PR, Paranaíba LM, Graner E, et al. Goldenhar syndrome: clinical features with orofacial emphasis. J Appl Oral Sci. 2010;18:646-9. doi: 10.1590/ S1678-77572010000600019
17. Shrestha UD, Adhikari S. Craniofacial Microsomia: Goldenhar Syndrome in Association with Bilateral Congenital Cataract. Case Rep Ophthalmol Med. 2015;2015:435967. doi: 10.1155/2015/435967.
18. Rad EM. Goldenhar syndrome with right circumflex aortic arch, severe coarctation and vascular ring in a twin pregnancy. Ann Pediatr Cardiol. 2014;7(3):217-20. doi: 10.4103/0974- 2069.140857
19. Beleza-Meireles A, Clayton-Smith J, Saraiva JM, Tassabehji M. Oculo-auriculo-vertebral spectrum: a review of the literature and genetic update. J Med Genet. 2014;51:635-45.
20. Sharma N, Passi S. Goldenhar syndrome. Indian J Dent Res. 2013;24:149.
21. Caron CJ, Pluijmers BI, Joosten KF, Mathijssen IM, van der Schroeff MP, Dunaway DJ, et al. Feeding difficulties in craniofacial microsomia: a systematic review. Int J Oral Maxillofac Surg. 2015;44:732-7. doi: 10.1016/j.ijom.2015.02.014
22. Modica RF, Barbeau LD, Co-Vu J, Beegle RD, Williams CA. Goldenhar syndrome associated with extensive arterial malformations. Case Rep Pediatr. 2015;2015:954628.
23. Jones KL, Smith DW. Smith's recognizable patterns of human malformation. 7th ed. Philadelphia: Elsevier Saunders; 2013.
24. Brosco KC, Zorzetto NL, Costa AR. Audiology profile in patients with Goldenhar's syndrome. Rev Bras Otorrinolaringol. 2004;70:645-9. doi: 10.1590/S0034-72992004000500011
25. Gorlin RJ, Jue KL, Jacobsen U, Goldschmidt E. Oculoauriculovertebral Dysplasia. J Pediatr. 1963;63:991-9.
 Correspondence to:
Correspondence to:
MAD Agnol
Av. Senador Attílio Fontana, 591-E, Efapi
89809-000, Chapecó, SC, Brasil
e-mail: mauroccs@gmail.com
Received on: 18/3/2016
Final version resubmitted on: 7/6/2016
Approved on: 6/7/2016
