










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.7 no.4 Joinville Dez. 2010
ORIGINAL RESEARCH ARTICLE
Evaluation of professors' and students' knowledge on crown-root fractures
Paola Cristine ValençaI; Carla Castiglia GonzagaI; Gisele Maria CorrerI; Tatiana Miranda DeliberadorI; Gisele Aihara HaragushikuI; Denise Piotto LeonardiI; Flares Baratto FilhoI,II
IDentistry Course, Positivo University – Curitiba – PR – Brazil
IIDentistry Course, University of Joinville – Joinville – SC – Brazil
ABSTRACT
OBJECTIVE: The aim of this study was to evaluate the knowledge on crown-root fractures among professors and students of a school of dentistry.
MATERIAL AND METHODS: A questionnaire comprising the treatment options for crown-root fractures at different depths and their follow-up periods was applied to 122 subjects divided into three groups: 1) students who had not attended any Endodontics and Surgery disciplines, 2) students who had concluded these disciplines; and 3) professors. The data was analyzed by descriptive statistics.
RESULTS: Most of Group 1 (90.3%) did not know the procedures to be adopted in cases of crown-root fractures. Conversely, more than 80% of Group 2 and 95% of Group 3 knew the procedures. Concerning to crown-root fractures up to 2mm deep, 26.9% of Group 1 and 48.5% of Group 3 would perform crown lengthening; 46.2% of Group 2 would perform fragment rebonding. In relation to fractures between 2 and 4mm deep, 21.2% of Group 1 would perform tooth extraction; 28.6% of Group 2, fragment rebonding; and 40.7% of Group 3, orthodontic extrusion. In fractures more than 4mm deep, most members of all groups would perform tooth extraction followed by implant. With regard to follow-up appointments, most members of all groups stated that their frequency should be at every 6 months (during the first year) and every year (for 5 years).
CONCLUSION: Students of Group 1 showed poor knowledge on crown-root fractures, while members of Groups 2 and 3 showed a proper knowledge.
Keywords: trauma; Endodontics; dental education.
Introduction
Dental traumas have been considered emergency conditions in Dentistry, since the immediate first-care treatment must be performed as soon as possible to prevent tooth loss [11]. The most common causes of dentoalveolar traumas have been falls from height or bicycle, automobile accidents, and fights or robberies [2, 13]. Epidemiological reports indicate that dental trauma is a serious health problem and could lead to aesthetic, psychological, social and therapeutic complications [2].
Crown-root fracture (CRF) is one type of dental trauma, and has been defined as the fracture involving enamel, dentin and cementum. This type of trauma is relatively common, comprising between 30 and 50% of the injuries to dental hard tissues. Most frequently, it has been the result of a horizontal impact [2]. The fracture line is usually single, but multiple fractures might occur. If they are present, the main fracture often will be the starting point [2]. In most cases, the fracture begins in the crown and extends in an oblique and downward direction very close to or below the alveolar bone crest. Depending on this extension, it may damage dental pulp
[2, 4]. Literature has reported that dental pulp has been involved in up to 80% of crown-root fracture cases [4]. This type of fracture is easily diagnosed. Intraorally, the crown would show mobility, and generally, the patient would report pain during mastication. The fracture line is not easily seen in radiographies and, when observed, it starts from the crown towards the root [6].
Crown-root fractures have attracted dentists' attention due to their prevalence, the variety of causes and multiplicity of outcomes, and treatment options [4], which depend on their depth and direction. The treatment strategy is mainly based on fracture depth (i.e., subgingival), lesion morphology, root length and morphology, and the aesthetic requirements of each case [6]. In superficial crown-root fractures, the fragment could be adhesively bonded, the tooth could be directly or indirectly restored and, if necessary, a gingivectomy could be performed [6]. Concerning to crown-root fractures between 2 and 4mm in depth, orthodontic and surgical extrusions have been possible options [5, 15]. However, in cases where the fracture is located further than 4mm in depth, depending on the root's length, its insertion in the alveolar bone, and the direction of the fracture line, the following procedures can be properly indicated: orthodontic extrusion, surgical extrusion, intentional replantation with 180º rotation, and tooth extraction [5, 10, 15]. In young patients, the risk-benefit ratio of each treatment option should be carefully evaluated, always taking into account the patient's age, stage of root development and the preferences of parents and/or the patient [15].
The understanding of the causes, besides the severity and distribution of different types of dental trauma may help clinicians to establish effective treatment protocols for these conditions and prevent further trauma [2, 3, 5, 7, 10, 12, 16]. At the same time, given the multiplicity of treatment options that may be performed in crown-root fractures, it is important and necessary to evaluate the dentist's knowledge. Special attention should be given to the academic environment, including professors and undergraduates in Dentistry. In the dental school where this study was carried out, problem-based learning is the method of choice for teaching the theoretical basis of some disciplines of the curriculum. In this model, the responsibility for learning is transferred from the professors to the students, who become the prime source of knowledge, autonomously seeking the information to solve a particular problem. The professors guide the work of the students. The teaching of emergency care, especially dental trauma, is supplemented by seminars, and by individual and group work activities. It is important to state that in the last few years, an integrated curriculum design was implemented at this dental school, which has enabled the students to recognize several concepts and inter-related disciplines. This new curriculum has allowed interdisciplinary articulation in order to lead the students to integrate the contents and interdisciplinary modules of increasing complexity from the beginning of the course.
The aim of this study is therefore to evaluate the knowledge on crown-root fracture of Dentistry students and professors, aside from the treatment options, through the application of a questionnaire.
Material and methods
A questionnaire was distributed to 94 students and 28 professors of the School of Dentistry of the Positivo University (Curitiba, PR, Brazil). The respondents were divided into 3 groups: 1) students who had not attended any Endodontics and Oral Surgery disciplines; 2) students who had concluded these disciplines or who had had at least a theoretical knowledge on the treatment of crown-root fractures; and 3) professors of all disciplines.
The questionnaire comprised 9 closed-end questions about the knowledge on crown-root fractures and different treatment options. The questionnaire was pre-tested in a population similar to the one involved in the study, and it was applied after the approval of the institutional review board. The individuals willing to participate in the study were informed of its voluntary nature and strict confidentiality was assured. After receiving the questionnaire, the respondents had 10 minutes to answer the questions.
The answers to all questions were assessed and data were analyzed by descriptive statistics.
Results
A total of 122 questionnaires were returned. Fourteen were excluded from the analysis, because they were not completely answered. Thus, 108 questionnaires were considered as valid, totaling 52, 32, and 24 questionnaires for Groups 1, 2 and 3, respectively.
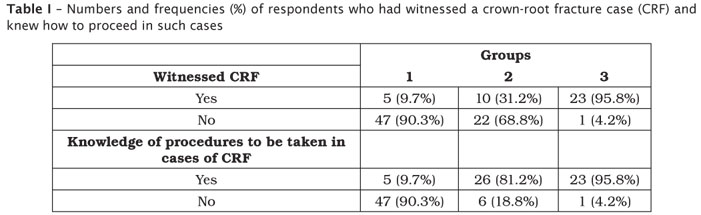
Table I shows the responses to the questions of CRF cases observation and knowledge of CRF procedures to be adopted in such cases. The vast majority of Group 1 (90.3%) reported that they had not witnessed any cases of CRF and did not know how to proceed in such cases. Among the students of Group 2, 31.2% had already witnessed at least one case of CRF and 81.2% claimed to know the treatment procedures. Among professors (Group 3), 95.8% had already witnessed at least one case of CRF and knew the clinical procedures to be performed in these cases.
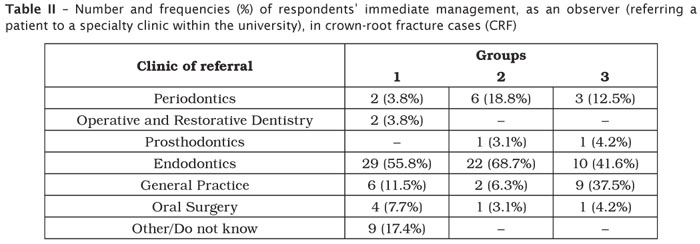
Table II lists the immediate procedure performed by the respondents in cases of CRF, as an observer. In all groups, most of the respondents indicated that these cases would be sent first to an Endodontics clinic. It is worth noting that, in Group 1, even without attending the disciplines of Endodontics and Oral Surgery, only 17.4% of students were unable to answer the question, and, in Group 2, all students were able to answer this question. In Groups 2 and 3, none of the respondents would refer these patients to Operative and Restorative Dentistry clinics.
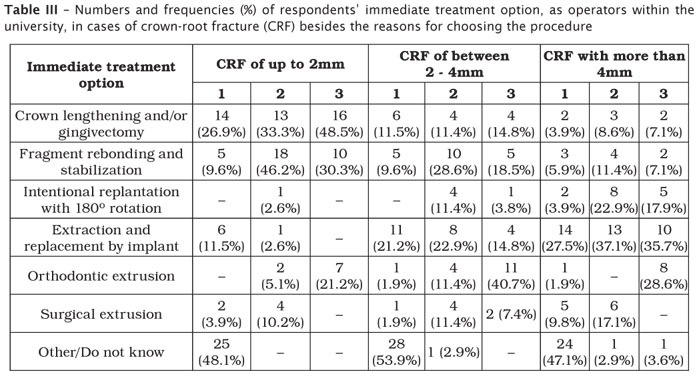
Table III indicates several treatment options for CRF at 3 depths (up to 2mm, between 2 and 4mm, and more than 4mm) considering the respondents as operators. Considering CRF up to 2mm deep, 26.9% would perform crown lengthening and/or gingivectomy; in CRF between 2 and 4mm in depth, 21.2% would perform extraction and replacement by implant; cases of CRF with more than 4mm in depth, 27.3% would execute the treatment options of extraction and replacement by implant.
Group 2 showed more varied responses. In CRF up to 2mm deep cases, 46.2% would execute dental fragment rebonding and splinting (stabilization). With CRF between 2 and 4mm in depth, 28.6% would perform fragment rebonding, and in CRF with more than 4mm in depth, tooth extraction and replacement by implant would be carried out by 37.1% of the respondents. Interestingly, 22.9% would perform intentional replantation with 180º rotation.
In Group 3, the treatment options for CRF up to 2mm in depth were crown lengthening and/or gingivectomy (48.5%); for CRF between 2 and 4mm in depth, 40.7% would perform orthodontic extrusion; and for CRF with more than 4mm in depth, 35.7% would execute tooth extraction and replacement by implant. Unlike in Group 2, 28.6% would perform orthodontic extrusion instead of intentional replantation.
Figure 1 shows the reasons for the choice of the clinical procedure in cases of crown-root fracture for the three groups. In Group 1, 50% of the respondents did not indicate the main reason of the treatment choice for the three depths of fracture studied. This was probably because they had declared in the previous questions of the questionnaire that they did not know the correct treatment option for CRF. The most cited reason for the treatment choice was "to be a more conservative procedure", followed by "fast aesthetical results"(Group 1). In CRF that were more than 4mm deep, this latter answer was the most chosen, followed by "more conservative procedures". In Group 2, most of the respondents chose "more conservative procedures", followed by "fast aesthetical results", for all CRF depths. With Group 3, the most cited reason was "more conservative procedure", followed by "lower cost", except for CRF up to 2mm deep, where "more conservative procedures"was the most cited answer, followed by "fast aesthetical results".
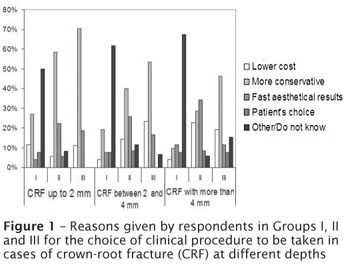
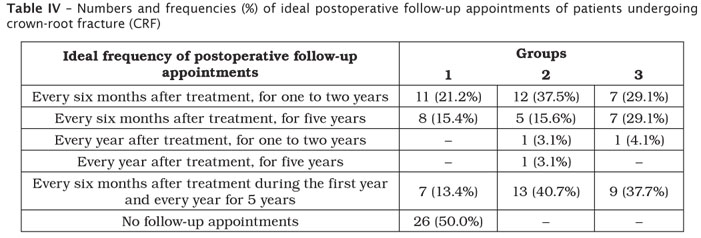
Table IV presents the respondents' ideal frequency of postoperative follow-up appointments of patients undergoing CRF. Half of the respondents of Group 1 did not answer the question; 21.2% indicated postoperative follow-up appointments at every 6 months after treatment, from 1 to 2 years. Most of the students of Group 2 (40.7%) would consider ideal postoperative follow-up appointments every 6 months after treatment in the first year, and once a year for 5 years, while in Group 3, 37.7% would schedule postoperative follow-up appointments every 6 months after treatment in the first year, and every year for 5 years.
Discussion
Crown-root fractures are common in the academic environment, because in dental school practice clinics, the treatments are often performed separately, at different disciplines, and consequently there is almost no integrated treatment. Therefore, it is relatively common that, for example, patients who have finished endodontic treatment may not be able to undergo the restorative treatment as soon as possible, because they must be referred to either the Restorative dentistry or the Prosthodontics practice clinic. During this period, the possibility of fracture occurrence will be increased should there be a trauma in the facial region. Additionally, if an injury occurs, many patients will seek treatment at the university's dental practice clinics or emergency services.
Even without knowing the adequate procedures to be performed in cases of CRF, it is extremely important that students be familiar with the correct dental specialty practice clinic for referring these patients. In relation to this specific question, students of Group 1 answered that they would refer these patients to the Endodontics, General Practice, and Oral Surgery clinics. This shows that although these students did not yet know and/or were not able to perform the treatment for this fracture type, they were able to refer these patients to the specific clinics, where the appropriate treatment would be performed. The same could be said about the students of Group 2, who indicated the Endodontics and Periodontics clinics for referring patients who had undergone CRF (table II).
These results could be attributed to the educational philosophy of this university, which has adopted the problem-based learning methodology, in addition to an integrated curriculum. Therefore, since the first year, the students are introduced to clinical training and are able to perform less complex procedures. This new integrated curriculum was implemented at this university in the last few years, when teachers were encouraged to use active learning methodologies, such as problem-based learning and discussions, even though traditional classes were not completely abandoned. Curriculum integration through use of problem- or case-based approaches has many advantages, improves the quality of instruction, reinforces the cohesiveness of the curriculum, and invigorates the learning process by developing students' critical thinking skills [9, 14].
Traumatology has been an appropriate subject for an integrated teaching and for problem-based learning, because problems and/or questions can be easily constructed around trauma cases, and the students can search for knowledge and suggest treatment protocols with an integrated approach [1]. As part of this new curriculum design, first-year students can assist senior students in their clinical practice and observe professors performing demonstrative procedures. The opportunity for students to observe and assist before their clinical years of dental school practice, can promote a smoother transition to clinic practice, enhance learning retention, and improve clinician-patient interaction [8].
In crown-root fractures that are less than 2mm in depth, the fractured fragment may be removed, and depending on its integrity, be adhesively bonded. Other protocols have comprised the direct or indirect restoration of the tooth and, if necessary, a gingivectomy can be performed [10]. In this study, the answers given by the respondents of the three groups were satisfactory, indicating that a good percentage of respondents would opt for adequate procedures (table III). In Groups 2 and 3, 33.3% and 48.5%, respectively, indicated crown lengthening and/or gingivectomy; 46.2% and 30.3%, respectively, indicated fragment rebonding. Since the respondents could choose up to two treatment options, the respondents selected these two approaches, probably depending on the clinical situation, in an attempt to restore the fractured tooth aesthetically.
It should also be noted that in Group 1, 26.9% and 9.6%, chose the options of crown lengthening and fragment rebonding, respectively. At the same time, 11.5% indicated less conservative procedures, such as tooth extraction, even in a clinical situation in which the fracture could be repaired and the tooth vitality maintained. This fact indicates that some students still need to improve their knowledge on conservative clinical treatments of superficial crown-root fractures. It should be emphasized, however, that these students had not attended the Endodontics and Oral Surgery disciplines, in which they would have improved their clinical knowledge on CRF.
If the fracture reached 3 or 4mm deep into dental root, it would be unlikely that the single use of the known restorative techniques could provide a good result, and it would be necessary to select another treatment technique [16]. Orthodontic extrusion is one possible option, and although it is slow and uncomfortable for the patient, it offers good aesthetic results and preserves tooth vitality [10].
Another option for the conservative treatment of fractures up to 4mm deep has been surgical extrusion. Nevertheless, it should only be used when the root fragment is long enough to allow the placement of a cast post and core and a crown. The intentional replantation with 180º rotation was firstly used to treat complex cases of endoperiodontal lesions [16] and iatrogenic complications, such as root perforations [3]. In cases of lingual oblique fractures, 180º rotation should be considered to enable the prosthetic preparation. The tooth should be endodontically treated 3 weeks after replantation and prosthetically restored after 2 months. In literature, this procedure is considered fast and safe, but it must be correctly indicated, requiring a multidisciplinary approach [2].
The success of these treatments depends not only on the dentist's ability, but also on a fast decision-making process, since the treatment should be initiated as soon as possible after the occurrence of the fracture. Although there has been a tendency to maintain the tooth in the mouth for as long as possible, the extraction of the tooth is usually recommended, especially when the fracture involves more than a third of the crown and root; in these cases, prosthetic restoration is not possible [5].
As shown in table III, most of Group 1 students, who had chosen one of the treatment options for fractures between 2 and 4mm deep, indicated tooth extraction. Although this procedure is not been considered wrong, the patient must be informed and must approve this treatment option, since other more conservative treatments, such as orthodontic extrusion, could be indicated. It is worth noting that, although intentional replantation with 180º rotation has been frequently reported in the literature and shows good success rates [6, 15], only 11.4% of students in Group 2 and 3.8% of teachers in Group 3 indicated this treatment option for fractures up to 4mm deep.
In cases where the fracture is more than 4mm in depth, many of these treatment options have been also considered correct. Orthodontic extrusion, surgical extrusion, intentional replantation with 180º rotation, and tooth extraction could be indicated depending on the root's length, its insertion in the alveolar bone, and the direction of the fracture line [4, 6]. However, in this study, tooth extraction and replacement by implant was the treatment option more frequently indicated by the three groups. On the one hand, it is believed that this occurred due to the high success rates and patients' greater acceptance of implants. On the other hand, Groups 2 and 3 also indicated intentional replantation, surgical extrusion (Group 2) and orthodontic extrusion (Group 3), as an attempt to preserve and restore the remanent root.
Concerning the reasons for the choice of the clinical treatments to be taken in cases of CRF, it is observed in figure 1 that, regardless of the fracture's depth, there was a strong tendency of the three groups towards justifying their treatment choice as more conservative. This tendency was most pronounced in Group 3 (comprising professors), indicating that these professionals seem to prefer alternative treatments in order to maintain the teeth in the oral environment as long as possible. Accordingly, the students followed the teachers' point of view, also tending to choose, whenever possible, the most conservative treatment protocols. It should be noted, however, that the percentage of reasons for the choice of conservative procedures was greater in cases of superficial fractures (with up to 2mm in depth). In cases of fractures between 2 and 4mm deep, besides choosing more conservative procedures, Group 2 students also indicated procedures with faster aesthetical results, and Group 3 indicated lower-cost procedures. With crown-root fractures that were more than 4mm deep, the teachers justified their procedures' choices as being more conservative, while Groups 2 and 3 justified their procedures' choices in terms of producing faster aesthetical results. These results also reflect a strong tendency towards aesthetics, since the professionals tend, in most cases, to choose treatment options that present good aesthetic outcomes, and that satisfy their patients' demands.
Since the choice of the best treatment option in each case and its implementation are extremely important, each of the procedures described above as treatment options for crown-root fracture should be clinically and radiographically monitored for a certain period of time. Generally, in superficial fractures showing the preservation of tooth vitality, postoperative follow-up appointments could be scheduled at every 2 months after treatment, for 1 year post-trauma [2]. Considering deeper fracture cases and depending on the treatment complexity, follow-up appointments should be scheduled at every 6 months after treatment for 5 years post-trauma [2]. The results of this study (table IV) indicated that all groups showed a good understanding regarding the postoperative follow-up of patients with crown-root fracture, since 28.8%, 59.4% and 66.8% of respondents in Groups 1, 2 and 3, respectively, indicated postoperative follow-up of 5 years post-trauma.
Conclusion
Within the limitations of this study, it can be concluded that students who had not attended the Endodontics and Oral Surgery disciplines showed poor knowledge on CRF. Both students who had concluded these disciplines and professors showed adequate knowledge on CRF, although there were some differences in their clinical procedure options.
References
1. Andersson L. Trauma in the undergraduate curriculum. Dent Traumatol. 2009 Feb;25(1):1. [ Links ]
2. Andreassen JO, Andreassen FM. Textbook and colour atlas of traumatic injuries to the teeth 3rd ed. Copenhagen: Munksgaard Publishers; 1994. [ Links ]
3. Barnett RJ, Burton WE, Nuckles DB. Intentional replantation: report of a successful case. Quintessence Int. 1992;23:755-7. [ Links ]
4. Castro JC, Poi WR, Manfrin TM, Zina LG. Analysis of the crown fractures and crown-root fractures due to dental trauma assisted by the integrated clinic from 1992 to 2002. Dent Traumatol. 2005;21:121-6. [ Links ]
5. Dale RA. Dentoalveolar trauma. Emerg Med Clin North Am. 2000;18:521-39. [ Links ]
6. Fariniuk LF, Ferreira EL, Soresini GC, Cavali AE, Baratto Filho F. Intentional replantation with 180 degrees rotation of a crown-root fracture: a case report. Dent Traumatol. 2003;19:321-5. [ Links ]
7. Feldens CA, Kramer PF, Vidal SG, Faraco Junior IM, Vítolo MR. Traumatic dental injuries in the first year of life and associated factors in Brazilian infants. J Dent Child. 2008;75(1):7-13. [ Links ]
8. Horst JA, Clark MD, Lee AH. Observation, assisting, apprenticeship: cycles of visual and kinesthetic learning in dental education. J Dent Educ. 2009;73(8):919-33. [ Links ]
9. Howard KM, Stewart T, Woodall W, Kingsley K, Ditmyer M. An integrated curriculum: evolution, evaluation, and future direction. J Dent Educ. 2009;73(8):962-71. [ Links ]
10. Lin S, Levin L, Goldman S, Peleg K. Dento-alveolar and maxillofacial injuries: a 5-year multi-center study. Part 1: general vs facial and dental trauma. Dent Traumatol. 2008;24:53-5. [ Links ]
11. Oliveira TM, Sakai VT, Moretti ABS, Silva TC, Santos CF, Machado MA. Knowledge and attitude of mothers with Regards to Emergency Management of Dental Avulsion. J Dent Child. 2007;74(3):200-2. [ Links ]
12. Ruviere DB, Costa MMTM, Cunha RF. Conservative management of severe intrusion in a primary tooth: a 4-year follow-up. J Dent Child. 2009;76(1):87-91. [ Links ]
13. Shayegan A, De Maertelaer V, Vander Abbeele A. The prevalence of traumatic dental injuries: a 24-month survey. J Dent Child. 2007;74(3):194-9. [ Links ]
14. Snyman WD, Kroon J. Vertical and horizontal integration of knowledge and skills – a working model. Eur J Dent Educ. 2005;9(1):26-31. [ Links ]
15. Wang Z, Heffernan M, Vann Jr. WF. Management of a complicated crown-root fracture in a young permanent incisor using intentional replantation. Dent Traumatol. 2008;24:100-3. [ Links ]
16. Yu L, Xu B, Wu B. Treatment of combined endodontic-periodontic lesions by intentional replantation and application of hydroxyapatites. Dent Traumatol. 2003;19:60-3. [ Links ]
 Corresponding author:
Corresponding author:
Flares Baratto Filho
65 Geraldo Lipka St., apt. 101
ZIP code 81200-100 – Curitiba – PR
E-mail: fbaratto@uol.com.br
Received for publication: April 23, 2010.
Accepted for publication: June 2, 2010.

{kind=link}
{kind=link}
{kind=link}
{kind=link}