










 Inglés
Inglés




 Permalink
PermalinkRSBO (Online)
ISSN 1984-5685
RSBO (Online) vol.7 no.4 Joinville dic. 2010
SHORT COMMUNICATION
Casual disclosure of an enlargement of the sella turcica during orthodontic treatment planning
Allan AbuabaraI; Giuseppe V. CruzII; Mário J. NóbregaIII
IHealth Secretary, City of Joinville – Joinville – SC – Brazil
IIDentistry Course, University of Joinville – Joinville – SC – Brazil
IIIDepartment of Ophthalmology, Sadalla Amin Ghanem Eye Hospital – Joinville – SC – Brazil
ABSTRACT
Systemic disorders may be identified during dental care provision at oral and maxillofacial radiographs. We present a casual disclosure of an abnormal enlarged sella turcica with erosion of posterior clinoid process in an asymptomatic 32-year-old female. Although the diagnosis remains undetermined because no follow-up information was obtained from the referring clinician, possible options are discussed. The orthodontists and general practitioners must pay special attention when analyzing dental and maxillofacial images.
Keywords: sella turcica; pituitary tumor; lateral cephalogram.
Introduction
Pituitary gland tumors may cause neurological and hormonal symptoms. The neurological symptoms are due to compression or invasion of adjacent structures, such as the optic nerve, causing visual involvement [10]. The optic chiasm lies in close proximity to the pituitary gland and can be compressed by tumors leading to visual disturbances (bitemporal hemianopsia) [6]. Pituitary tumors may either be clinically silent or secrete hormones, including prolactin, growth hormone (acromegaly), adrenocorticotrophic hormone (Cushing's disease) or, rarely, thyroid-stimulating hormone or gonadotropins. These adenomas may cause clinical infertility, growth disorders and hypercortisolism or metabolic dysfunctions [2]. Lateral view of a skull radiograph is routinely used during the orthodontic treatment and maxillofacial surgery. We present an incidental finding of abnormal enlarged sella turcica with erosion of posterior clinoid process in a 32-year-old female.
Case report
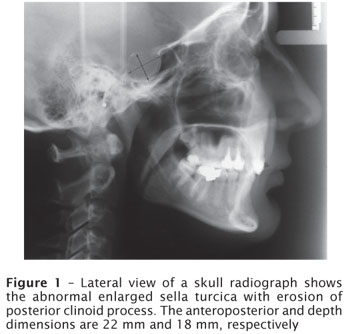
The patient searched for the Orthodontic Clinic for correction of her dental crowding and did not report any systemic symptoms. No significant cephalometric discrepancy was observed. The anteroposterior and depth dimensions of the sella turcica were approximately 22 mm and 18 mm (figure 1), respectively. These measurements exceeded the accepted maximum amplitudes of the adult sella, which are 16 mm in the anteroposterior dimension and 12 mm in depth [5, 7]. The medical history was noncontributory. No signs or symptoms related to pituitary dysfunction were identified. The final diagnosis remains undetermined because no follow-up information was obtained from the referring clinician.
Discussion
The sella dimensions ranges between 5 mm and 16 mm in the anteroposterior diameter and between 4 mm and 12 mm in depth [5, 7]. Some of the differences in the measurements may be secondary to the varying magnifications used in the radiographic procedures [2]. Weisberg et al. [9] evaluated 100 patients with an enlarged sella turcica and the most common cause of its expansion was a primary intrasellar pituitary tumor. According to the authors, the course of patients with enlarged sella turcica is variable. Sometimes, they present initial peripheral visual involvement and develop progressive visual impairment; otherwise, some individuals may have only a headache [9]. Asymptomatic patients with an enlarged sella turcica should have an air study to exclude an "empty sella"syndrome, an anatomical entity in which the pituitary fossa is expanded and partially filled with cerebrospinal fluid owing to the arachnoid herniation, while the pituitary gland is compressed against the posterior rim of the fossa [3]. Differential diagnosis of a large sella also include primary hypothyroidism [9]; adenomas, aneurysm [1]; Hajdu-Cheney syndrome, which is a rare disorder of bone metabolism, associated with acro-osteolysis of the distal phalanges, short stature, distinctive craniofacial and skull changes, premature tooth loss and periodontitis [1]; craniopharyngiomas; Rathke's cleft cysts; arachnoid cysts; parasellar lesions; granulomatous, inflammatory and infectious processes such as tuberculosis, sarcoidosis, giant cell granuloma, sphenoid sinus mucoceles and others [4]. Complementary imaging exams such as computed tomography and magnetic resonance imaging are essential. The magnetic resonance imaging appears to be superior to computed tomography because of its inherently greater soft-tissue contrast, which allows clear visualization of the optic chiasm, optic nerves, cavernous sinuses and carotid arteries; computed tomography is frequently unable to diagnose correctly an empty sella [8].
Systemic disorders may be identified during dental care provision at oral and maxillofacial radiographs. The radiologists, orthodontists and general practitioners must pay special attention when analyzing dental and maxillofacial images. If pituitary tumor is suspected or found, the patient has to be immediately referred to a specialized physician for further investigation.
References
1. Arlot S, Lalau JD, Galibert P, Quichaud J. Intrasellar carotid aneurysm simulating prolactin adenoma. Rev Med Interne. 1985;6:505-9. [ Links ]
2. Chesnokova V, Melmed S. Pituitary tumor-transforming gene (PTTG) and pituitary senescence. Horm Res. 2009;71(Suppl 2):82-7. [ Links ]
3. Degli Uberti EC, Teodori V, Trasforini G, Tamarozzi R, Margutti A, Bianconi M et al. The empty sella syndrome. Clinical, radiological and endocrinologic analysis in 20 cases. Minerva Endocrinol. 1989;14:1-18. [ Links ]
4. Freda PU, Post KD. Differential diagnosis of sellar masses. Endocrinol Metab Clin North Am. 1999;28:81-117. [ Links ]
5. Friedland B, Meazzini MC. Incidental finding of an enlarged sella turcica on a lateral cephalogram. Am J Orthod Dentofacial Orthop. 1996;110:508-12. [ Links ]
6. Reith W. Tumors in the region of the sella turcica. Radiologe. 2009;49:624-31. [ Links ]
7. Shapiro RS, Janzen AH. The normal skull. New York: Paul B. Hoeber; 1960. p. 146-160. [ Links ]
8. Stein AL, Levenick MN, Kletzky OA. Computed tomography versus magnetic resonance imaging for the evaluation of suspected pituitary adenomas. Obstet Gynecol. 1989;73:996-9. [ Links ]
9. Weisberg LA, Zimmerman EA, Frantz AG. Diagnosis and evaluation of patients with an enlarged sella turcica. Am J Med. 1976;61:590-6. [ Links ]
10. Weisberg LA. Asymptomatic enlargement of the sella turcica. Arch Neurol. 1975;32:483-5. [ Links ]
 Corresponding author:
Corresponding author:
Allan Abuabara
400 Fernando Machado St., apt 201
ZIP code: 89204-400 – Joinville – SC
E-mail: allan.abuabara@gmail.com
Received for publication: January 11, 2010
Accepted for publication: February 2, 2010.
