










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.1 Joinville Jan. 2011
CASE REPORT ARTICLE
Large ameloblastic fibro-odontoma in a 3 year-old child: case report
Laurindo Moacir SassiI; Roberta Targa StramandinoliI; José Luis DissenhaI; Fernando Luis ZanferrariI; Juliana Lucena SchusselII
IDepartment of Oral and Maxillofacial Surgery of Erasto Gaertner Hospital – Curitiba – PR – Brazil
IIUniversity of São Paulo – São Paulo – SP – Brazil
ABSTRACT
INTRODUCTION: The ameloblastic fibro-odontoma is a rare mixed neoplasm composed of proliferating odontogenic epithelium, ectomesenchymal tissue, and varying degrees of dental hard tissue formation. The mean age of the incidence is from 8-12 years and there is no gender or anatomic site predilection, but it is most commonly found in children's or teenager's jaws.
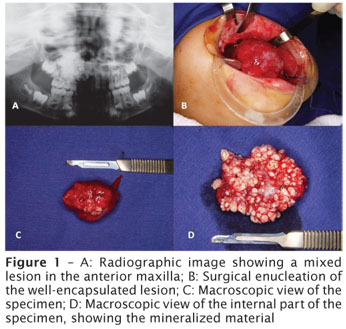
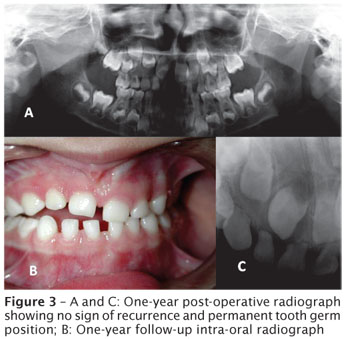
CASE REPORT: A 3-year-old female patient showed a swelling in anterior maxilla, with facial asymmetry. Radiographically, it presented as a mixed lesion with undefined limits. Clinical hypothesis was odontoma. Enucleating surgery was conducted with tooth germs preservation. The final diagnosis was ameloblastic fibro-odontoma. No recurrence was observed at 1-year follow-up period, and the permanent tooth germs were correctly positioned for eruption.
CONCLUSION: Although ameloblastic fibro-odontoma is a benign lesion, it developed in a very early age, with rapid growth and destruction of cortical bone. Proper surgical enucleation allowed the teeth maintenance.
Keywords: odontogenic tumors; ameloblastic; intraosseous lesion.
Introduction
Ameloblastic fibro-odontoma (AFO) is a rare odontogenic tumor defined by World Health Organization (WHO) as a benign neoplasm composed of proliferating odontogenic epithelium embedded in a cellular ectomesenchymal tissue that resembles dental papilla, and with varying degrees of inductive change and dental hard tissue formation [1]. It is classified into the group of tumors of odontogenic epithelium with odontogenic ectomesenchyme, with or without dental hard tissue formation [1].
The mean age of the incidence is from 8-12 years and there is no gender or anatomic site predilection. Furthermore, the tumor is most commonly found in the mandible of children or teenagers.
The relative arrangement of the soft tissues and the stage of development of the involved tooth are useful criteria for differential diagnosis. According to the revised WHO classification, it is a benign tumor without invasive growth, contrastingly to ameloblastoma [1].
Case report
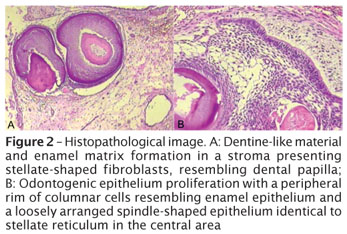
A 3-year-old female patient was referred to the Department of Oral and Maxillofacial Surgery of the Erasto Gaertner Hospital complaining about a swelling area in maxilla. During clinical examination a large swelling in left anterior maxilla was observed, resulting in facial asymmetry. Panoramic radiography showed a mixed lesion affecting a large area from the left deciduous first molar to left deciduous lateral incisor, with undefined margins. The clinical hypothesis was odontoma. The lesion was enucleated under general anesthesia and the specimen was sent to analysis (figure 1). Microscopic features revealed an odontogenic neoplasia characterized by an odontogenic epithelium proliferation, island and strand-like of varying sizes, with a peripheral rim of columnar cells resembling enamel epithelium, and a loosely arranged spindle-shaped epithelium identical to stellate reticulum in the central area. The lesion stroma showed stellate-shaped fibroblasts in a myxoid arrangement resembling dental papilla. Dentine-like material and enamel matrix were observed in other areas, and sometimes surrounding the odontogenic epithelial islands (figure 2). The large amount of calcifying tissue presence was unusual considering the patient's age. The permanent tooth germs were preserved. No recurrence was observed at 1-year follow-up period, and permanent tooth germs seem to be correctly positioned for eruption (figure 3).
Discussion
This case report's lesion differential diagnosis included odontoma, ameloblastoma, odontoameloblastoma, and ameloblastic fibroma. On the one hand, the presence of both dentin and enamel is important to differentiate the lesion from ameloblastic fibroma, which shows no sign of tooth differentiation. On the other hand, the exclusive presence of dentin characterizes another entity, ameloblastic fibrodentinoma [3]. Odontoameloblastoma usually is an unencapsulated lesion, whose behavior resembles the ameloblastoma. For this reason, it must be similarly treated. Ameloblastic areas and ghost cells presence helps the differential diagnosis [1].
Philipsen et al. (1997) [5] found 86 cases of AFO in literature, with only 1 case with an age at diagnosis of >20 years. AFO average age at presentation was 9 years old (raging from 1 to 22 years old), with a male-female ratio of 1.4:1. The most common occurrence site was the posterior mandible, with a mandible-maxilla ratio of 2.4. In this case report, the lesion was found in a 3 year-old girl, at the anterior maxilla. Usually, the lesion is discovered by investigative radiographs to determine the cause of failed tooth eruption [6]. Similarly to this case report's patient, AFO is commonly asymptomatic and often presents with expansion of the involved bone [5].
The histological characteristics of AFO cannot be distinguished from odontoma, and consequently, some authors [6] believe that ameloblastic fibro-odontoma is an immature complex odontoma. In the same way, no ultrastructural differences were observed between AFO and ameloblastic fibroma [6]. The large amount of calcifying tissue present in the lesion may speak in favor of the theory that AFO is an early stage of odontoma. The amount of calcified material within the lesion is considerably variable. Lesions can vary from a mostly radiolucent lesion to one that is nearly completely radiopaque. This case report's lesion presented the formation of many denticles, similar to an odontoma.
The incidence of AFO varies from 0.3% to 1.7% [4, 2] among the odontogenic tumors, and when only pediatric cases are considered it represents 4.6% [4]. The mean age of incidence is between 8 to 12 years. This case report's lesion presented at very early age, with formation of a large amount of calcifying tissue. Since the lesion was well-encapsulated, it was possible to preserve the permanent teeth. After 1-year follow-up period, no sign of recurrence was observed.
Radiographically, AFO shows radiopaque and radiolucent areas that vary from one lesion to another; sometimes large amounts of mineralized tissue may resemble an odontoma [4]. The radiographic images and localization of our case report's lesion were suggestive of an odontoma. Usually, AFO is well encapsulated and different from ameloblastoma, presenting no local invasion. This was the reason for a more conservative treatment, as recommended by literature [5]. The lesion was removed without capsule laceration, which was better for prognosis.
The case reported here presented at very early age, with an important swelling but with no pain complaint. Enucleation of the lesion was a satisfactory treatment with good prognosis. Moreover, it preserves the teeth at the lesion's area, without recurrence risk.
Conclusion
The differential diagnosis with odontoameloblastoma and odontoma is essential for the correct treatment and follow-up, as well as, to reduce patient morbidity.
References
1. Barnes L, Eveson JW, Reihcart P, Sidransky D (eds.). Pathology & genetics head and neck tumours – World Health Organization classification of tumours. v. 9. Iarc Press; 2005. [ Links ]
2. Buchner A, Merrell P, Carpenter W. Relative frequency of central odontogenic tumors: a study of 1.088 cases from Northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg. 2006;64:1343-52. [ Links ]
3. Friedrich RE, Siegert J, Donath K, Jäkel KT. Recurrent ameloblastic fibro-odontoma in a 10-year-old boy. J Oral Maxillofac Surg. 2001;59(11):1362-6. [ Links ]
4. Guerrisi M, Piloni M, Keszler A. Odontogenic tumors in children and adolescents. A 15-year retrospective study in Argentina. Med Oral Patol Oral Cir Bucal. 2007;12:E180-5. [ Links ]
5. Philipsen HP, Reichart PA, Praetorius F. Mixed odontogenic tumours and odontomas: considerations on interrelationship. Review of the literature and presentation of 134 new cases of odontomas. Oral Oncol. 1997;33:86-99. [ Links ]
6. Slootweg PJ. An analysis of the interrelationship of the mixed odontogenic tumors – ameloblastic fibroma, ameloblastic fibro-odontoma, and the odontomas. Oral Surg. 1981;51:266. [ Links ]
 Corresponding author:
Corresponding author:
Juliana Lucena Schussel
201, Dr. Ovande do Amaral St. – Jardim das Américas
ZIP code 81520-060 – Curitiba – PR – Brazil
E-mail: julianals24@hotmail.com
Received for publication: May 17, 2010.
Accepted for publication: June 14, 2010.
