










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.3 Joinville Jul./Set. 2011
ORIGINAL RESEARCH ARTICLE
Statistical analysis of the prevalence, severity and some possible etiologic factors of gingival recessions among the adult population of Thamar city, Yemen
Abdullah Gh. AmranI; Mansour Ali S. AtaaII
I Dentistry School, Department of Periodontology, Thamar University
II Dentistry School, Department of Biostatistics, Sanaa University
ABSTRACT
Introduction and objectives: Gingival recession is an undesirable condition resulting in root exposure which is often not esthetic and may lead to sensitivity and root caries. The objective of the current study was to quantify and analyze the prevalence and severity of the gingival recession problem and also to identify the influence of some risk factors on gingival recession's occurrence. The current study is arguably important because there was no previous study of this type in Yemen. Material and methods: This study was performed on 602 non missing teeth participants of age class ≥ 20 years old who attending the learning dental clinics of faculty of dentistry at Thamar University, and Thamar General Hospital during the period January to October 2010. All measurements of gingival recession and loss of attachment were done with periodontal probe and under sufficient illumination. Furthermore the severity of gingival recessions was evaluated based on Miller's classification. Some measurements were done twice randomly in order to examine intra-observer agreement of data. Statistical analysis was accomplished using Chi-squares test and Logistic Linear Regression. Results: Our findings showed that 60.5% of patients had gingival recessions. The trend of gingival recession was upward within 20-29 (15.0%) to 30-39 years of age (16.8%) and was descending within 40-49 (15.9%) to 50 years of age and older (12.8%). Prevalence of gingival recession in females (33.6%) was found to be significantly higher than that in males (26.9%), (P<0.05). The localized recession (26.7%) and that of generalized (33.7%) were found to be significantly different, (P<0.05). The most significant differences of prevailed recessions were detected in buccal-labial & balatal-lingual (44.5%) and the upper & lower teeth (34.6%), respectively, (P<0.05). In addition, the recession in the anterior teeth (25.7%) was significantly much higher than that in posterior teeth (6%). Moreover, Class I Miller was significantly (P<0.05) the most common type of recession (30.5%) when compared to the other classes. The recession percentages of gingival recession size; < 3 mm (26.9), 3-4 mm (9.1) and > 4 mm (24.4), were found to differ significantly, (P<0.05). Similarly, the percentages of recessions in loss of attachment size; < 3 mm (8.8), 3-4 mm (9.3) and > 4 mm (42.5), were also significantly different, (P<0.05). Finally, the relationship between gingival recession and the concomitant risk factors was significant (P<0.05). Conclusion: Considering the high prevalence of gingival recession (60.5%) among Yemeni population may relate to the destructive periodontitis, and khat chewing so the implementation of oral hygiene instructions programs among Yemeni population would be a necessity.
Keywords: gingival recession; prevalence; Miller's classification; Chi-Squares tests.
Introduction
Gingival recession has been defined as a clinical condition on which the marginal periodontal tissue is located apical to the cementoenamel junction (CEJ) with concomitant exposure of the root surface. It is commonly observed in adult subjects 21. Gingival recession can be localized or generalized and often be associated with one or more surfaces 17. It leads to root exposure which is not esthetically desirable and may lead to sensitivity and root caries 11.
There are many factors that may cause gingival recession. Some of reviewed cross-sectional epidemiologic studies of gingival recession indicated that the prevalence of recession was associated with trauma, sex, malpositioned teeth, tobacco consumption and inflammation.
The presence and extent of gingival recession was also found to increase with age 3. Albandar and Kingman 2 studied the prevalence of gingival recession among subjects in the age group 30 to 90 years using a sample of 9,689 subjects and found that 23.8 million people have one or more tooth surfaces with gingival recession of 3 millimeters or more. They found that the prevalence of 1 mm or more recession in people aged 30 years and older was 58 percent. They also found that the recession appeared to increase with age. Susin et al 18 found that a high prevalence of GR was reported in Brazilian population and was also found that more than half of the individuals were presenting ≥ 3 mm recession defects. Gingival recessions were associated with a high level of periodontal disease.
Similarly, Gorman 4 found that the frequency of gingival recession increased with age and was greater in men than in women of the same age. Malpositioned teeth and toothbrush trauma were found to be the most frequent etiologic factors associated with gingival recession. Recession associated with labially positioned teeth occurred in 40 percent of patients with 16 to 25 years of age and increased to 80 percent of patients in the 36 to 86 years of age group. Those findings were corroborated by Murray 12, who examined 4,000 subjects and found that the incidence of gingival recession increased with age. The prevalence of gingival recession at the anterior lower teeth was more than that in the anterior upper teeth. This result might be related to the fact that the keratinized mucosa in the upper area is often much thicker and wider than its counterpart in the lower anterior area 9.
There are other factors which may play a significant role in the occurrence of gingival recession such as Anatomical, Pathological and Physiological factors. Anatomical factors include fenestration, dehiscence of the alveolar bone, abnormal tooth position in the arch, aberrant path of eruption of the tooth and individual tooth shape 3. Physiological factors may include the orthodontic movement of teeth to positions outside the labial or lingual alveolar plate which are leading to dehiscence formation 20. Pathological factors include bone resorption as a sequel to microbially induced periodontal diseases. In addition to psychological factors, various forms of trauma – such as vigorous tooth brushing, aberrant frenal attachment, occlusal injury, operative procedures and tobacco chewing have been thought to play a role in the etiology of recession 6.
Epidemiological studies have concluded that traumatic tooth brushing may be associated with gingival recession where buccal gingival recession was noted more frequently on the left side of the jaw 1. The concept of multiple etiologies of gingival recession was also reported in parallel longitudinal studies conducted in Norwegian and Sri Lankan populations during the period 1969 to 1990 among 15 to 50 years of age 8. In Yemen there is another factor that may cause gingival recession. This factor is often called khat chewing (Catha edulis). The habit of chewing fresh leaves and twigs of khat is thought to stimulate amphetamine-like effects 7. It causes gingival recession by causing pressure force and mechanical effect on the gingiva, especially in the side being used for chewing khat 5. There are also other epidemiological studies that focused on the prevalence of gngival recession in some countries, for example: in the USA, gingival recession was reported in 78 to 100% of middle-aged individuals where 22 to 53% of the teeth were found to be affected 14. In Oslo, Norway, 51% of the adult subjects aged more than 18 years had gingival recession 15. In New Guinea, 11 to 40% of the adult individuals were found to be associated with gingival recession 16. In Urban Brazilian the gingival recession was reported to be 51.6%, 18 and in Finland, it was reported that 68% of the subjects were associated with gingival recessions 19. Gingival recessions were further reported following the criteria suggested by Miller in 1985 10.
The objective of the current study was to quantify and analyze the prevalence and severity of the gingival recession problem and also to identify the influence of some risk factors on gingival recession's occurrence. The current study is arguably important because there was no previous study of this type in Yemen.
Material and methods
The study sample composed of 602 adult subjects aged ≥20 years old, randomly selected from the patients attending to the learning dental clinics of the faculty of dentistry at Thamar University, and the department of diagnosis and dental treatment in Thamar City's General Hospital for dental treatment and check ups. All participants were informed on the evaluation to which they would be submitted and signed an informed consent term for participation in the study. All measurements of gingival recession and loss of attachment were done with a graduated periodontal probe and under sufficient illumination. The information and data were registered in a special questionnaire designed to include important information that would help us to detect the correlation between gingival recession and some risk factors as age, tooth brushing, smoking , khat chewing, and the other risk factors which evaluated by examination like occlusal injury, high frenium attachment, tooth malposition, teeth crowding and periodontitis. According to the respective age classes: 20 to 29, 30 to 39, 40 to 49 and more than or equal to 50 years, the subjects of both genders were divided into four groups with sizes of 204 patients for Group I, 190 patients for Group II, 117 patients for Group III and 91 patients for Group IV, respectively. The selection criteria comprised age 20 years and a mean number of 28 natural teeth of each participant. 16856 teeth of all subjects were examined; any patient has missing one or more than one tooth was excluded except the missing of third molars in order to prevent the adverse effect of the edentulous area on the adjacent gingiva. The participants of the present study were evaluated by the examiner himself. The sample included 329 women and 273 men. A graduated periodontal probe marked up to 15mm, model Color Coded Probe, code CP-15UNC-PCPUNC15, Hu-Friedy, and was employed for evaluation of the teeth of each subject. Four surfaces of each tooth were evaluated: mesial, buccal - labial , distal and lingual – palatal, by measuring the distance from cementoenamel junction (CEJ) to the gingival margin and loss of attachment measurements were obtained from the cementoenamel junction to the bottom of the pocket in the teeth which were infected with gingival recession. In cases on which the cementoenamel junction was covered by calculus, hidden by a restoration or possibly lost due to wear or carious lesions. Accordingly, the location of such junction was estimated on the basis of the adjacent teeth.
Three categories were established according to the gingival recession measurements of the root surface exposed; small recessions less than 3mm of root surface exposed, moderate recessions 3 to 4mm of root surface exposed and advanced recessions more than 4mm of root surface exposed to the oral environment. Furthermore, the recessions were further scored according to the system suggested by Miller in 1985 10.
GR data variables and notations
The SPSS 18 package was utilized in the analysis. Descriptive statistics were determined for all quantitative variables. The logistic regression model was used for fitting the gingival recession data. Moreover, cross-tabulations of variables were also done to test for strength of association and significance using the chi-squares test statistics. The results of statistical analysis and tests are presented in the form of tables numbered as table I to table V below. For ease of comparison and analysis, ages were recoded into four age groups, namely, 20- 29, 30-39, 40-49 and ≥ 50 years. Gingival recession diagnostic indicator was also coded as a binary variable with 0 and 1 values. The value 0 indicates that the patient is not infected with a gingival recession and 1 to indicate that the patient is having this recession disease. The variables considered in the analysis with their corresponding short notations shown in parentheses are listed as follows: Gingival recession (GR) or the response variable. The other variables are, age group (Age) with categories 1, 2, 3, and 4, sex of the patient with 2 categories, millers' class (GRClass) with 4 categories, gingival recession extension (GRExt) with 2 categories denoted by localized and generalized, upper & lower teeth (UpLo) with categories, 1 for upper, 2 for lower and 3 for both of upper and lower teeth, labial & lingual (LibLing) with categories, 1 for labial , 2 for lingual, and 3 for both of labial and lingual, anterior and posterior teeth (AntPos) categorized as 1 for anterior, 2 for posterior and 3 for both. On the other hand, the size (in mm) of gingival recession (GRmm) and Loss of attachment (Lossmm) were recoded as 1 for size <3 mm, 2 for size 3-4 mm, and 3 for size >4 mm. Furthermore, eight risk factors of binary scores (Yes or No) were also considered in the analysis. These variables are periodontitis (periodo), chewing Khat (ChKat), crowding teeth, malpostion (Malp), occlusal injury (Oclnj), smoking, aberrant frenal attachment (ApFrAtt) and Tooth brushing.
Statistical data analysis results
Table I reveals that the percentage of patients having recessions increased significantly with age, rising from 15.5 percent in the age group of (20- 29) mean age of 24.53 years to 16.5 percent in the age group of (30-39) mean age of 34.05 years and then gradually decreased from 15.7 percent in the age group of (40-49) mean age of 43.86 years to 12.5 percent and in the age group of ≥ 50 mean age of 59.08 percent. The overall percentage of patients having recessions is 60.5 percent. The results of testing the age group versus the gingival recession was highly significant as indicated by the corresponding large value of Chi-Squares test and the associated probability value (χ2=72.1, P<<<0.05).
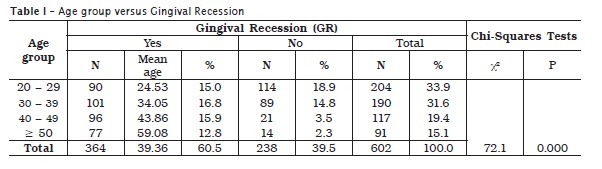
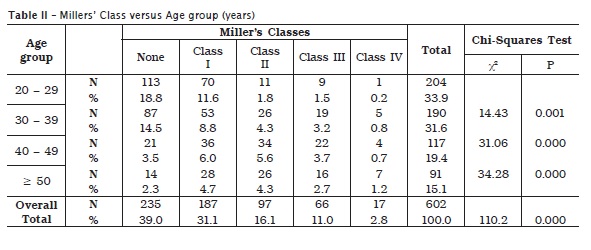
Table II displays the distribution of miller's classes versus age groups. The number of patients across the miller's classes and the corresponding age group were found to be significantly different (P<<<0.05). It can be seen that the age group of (20- 29) years is associated with the largest number of patients (204; 33.9%). Moreover, the most prevalent patients are those of miller's class I (39.0%). Multiple comparisons (likelihood-ratio tests) across miller classes, yielded that each of the second, third and fourth groups of age; namely, (30-39), (40-49) and ≥ 50, were significantly different when compared to age group (20-29) years. Moreover, Pairwise comparisons of table II columns indicated that Miller classes (I, II), (I, III) and (I, IV) were significantly different (P<0.000).
Table IIIa shows the results for the gingival recession versus the gender of the patient. The percentages of males and females in the study sample are 45.3 and 54.7 percent, respectively. The percentage of gingival recession in females (33.6 %) was higher than that in males (26.9 %). As can be seen from table IIIa, the association between gingival recession occurrence and the sex of the patient is highly significant at 0.05 confidence levels (P<0.05).
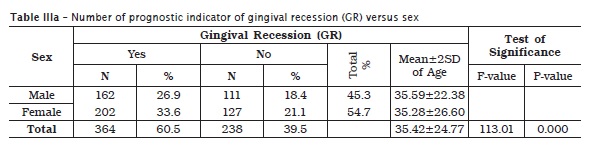
Table IIIb shows that the percentages of females and males who had gingival recessions classified as miller's class I were 20.4 and 10.2 percent, respectively. Moreover, the percentages of females and males associated with recessions in all millers' classes are, respectively, 33.3 and 26.9 percent. These results indicated also that the prevalence of gingival recessions with respect to patient's gender within millers' classes was found to be significantly different. As can be shown in table IIIb, the test results of GR versus Miller's class yielded that χ2 = 268.9 (P<0.05) for the males and χ2 = 320.7 (P<0.05) for the females and thus, sex of the patient was significantly associated with the indicator of the gingival recession across the miller's classes. In addition, Multiple Pairwise comparisons using Tukey procedure of miller classes (I, III), (I, IV), (II, IV) and (III, IV) were found to differ significantly (P<0.001), respectively.
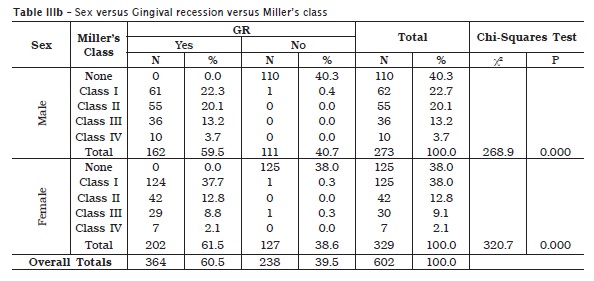
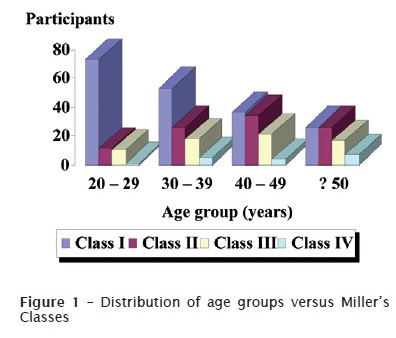
Figure 1 displays the distribution of age group versus miller's classes. As can be seen, the age group 20 to 29 years of class miller I had associated with the largest number of cases having recession in the sample.
Table IV displays the analysis results of fitting gingival recession versus the risk factors: Age group, periodontitis (periodo), chewing Khat (ChKat), crowding teeth, malpostion (Malp), occlusal injury (Oclnj), smoking, aberrant frenal attachment (ApFrAtt) and Tooth brushing. The analysis results shown in table IV, reveal that the relationship between gingival recession and each of these risk factors was seen to be significant (P<0.05). Those variables which were not significantly associated to GR are not included in table IV. Based on these estimates, the gingival recession can be conveniently estimated by those risk factors displayed in table IV.
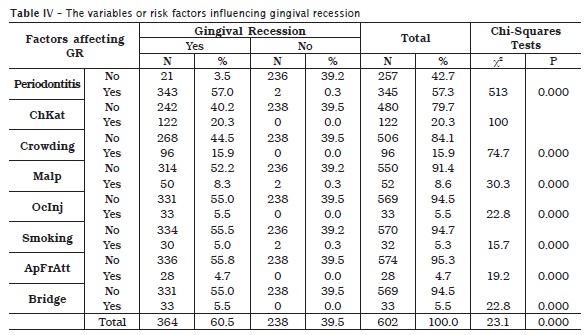
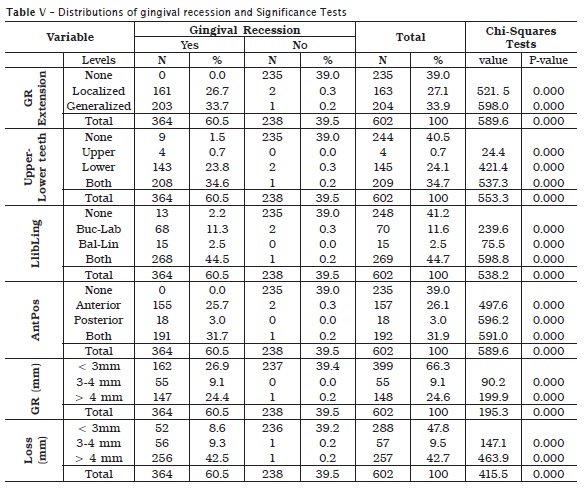
Table V shows the distribution analysis results of gingival recession variables by the number and their respective percentages of infected or non-infected subjects. The percentages of localized and generalized gingival recessions are, respectively, 26.7 and 33.7. The test for any significant difference between localized and generalized gingival recessions was found to be significant at 0.05 levels of significance. Pairwise comparisons of anterior, posterior and both using Bonferroni-corrected method, yielded that the occurrence of gingival recessions in the anterior and posterior teeth was significantly different (P<0.001). Similarly, the occurrence of gingival recessions in the anterior and both of anterior and posterior teeth was also significantly different (P<0.001). For the gingival recessions size, the Pairwise comparisons tests (Bonferroni) of categories (<3 mm, =3-4 mm) and (<3 mm, >4 mm) yielded highly significant differences with (P<0.001) for each pair. Similarly, the Pairwise comparisons tests for the loose of attachment size categories (<3 mm, =3-4 mm) and (<3 mm, >4 mm) produced significant differences with (P<0.001) for each pair.
Discussion
This present study indicates that, among 602 participants, the number of the patients who were found to be affected with gingival recession was 364 (60.5%). This result might be much higher than this if the human sample was included to those participants with extracted teeth as the current study sample has no missing tooth. By excluding patients with extracted teeth, the selection of participants only might make this study distinguishable and even different from other studies. The prevalence of gingival recession is considered to be high in comparison with other studies 15.This diversity might be due to the poor oral hygiene among Yemeni population. In addition, our study indicated that the number of infected participants with gingival recession was not only high but also those participants were found to be associated with chronic periodontitis 18. The percentage of gingival recession in female was 33.6% whereas in male was 26.9%. This result differs from the result of other study where the prevalence of gingival recession in females was less than males 2. The current study showed that, the gingival recession increased within the progress of age among the four age groups. From among 204 participants of the first age group (20-29) of the sample, the number of infected participants with gingival recession was 90 out of 204 (44.12%). For the second group (30-39) years of age, the gingival recession was observed in 101 (53.16%) participants among 190. For the third age group (40-49) years the number of participants who were found to have gingival recession was 96 (82.05%) out of 117 participants and for the fourth age group of the sample (>50) years, 77 (84.62%) out of 91 participants were infected with gingival recession. These findings are consistent with several studies which demonstrated that, the prevalence of GR increased with age. The relationship between increasing the prevalence of gingival recession and age could be due to the longer period of exposure to the agents that caused gingival recession to be associated to intrinsic changes in the organism, both of local and systemic. For Millers' Class versus age group, our study yielded that, the 1st miller class had associated with the largest number of cases having recessions in the sample when compared to that of class II, class III and class IV, respectively, where recession was decreased 1. Moreover, the current study indicated that, the percentage of gingival recession with less than 3mm vertically was 26.9% whereas the percentage of gingival recession with more than 4mm was 24.4%, which indicated that, the prevalence, extension and severity of this clinical aspect increased with age 1,2,4. The loss of attachment of >4mm was the highest percentage (42.5%), compared to that of less than <3mm (8.6 %) and = 4mm (9.3%). This difference was found to be significant at 0.05 levels of significance. The reason for this significantly difference could be related to the poor oral hygiene among most of the participants that tended to increase pocket depth and loss of attachment. The current study found that, the percentage of localized gingival recession was 26.7% which is considered to be high when compared to the generalized gingival recession (33.7%). This might be due to some local factors that caused localized gingival recession as high as franeium attachment, occlusal trauma and localized chronic periodontitis 19. The gingival recession associated with labially positioned teeth more than in the lingual sides with high significant difference and the percentage of recession at the lower teeth was found to be more than that of the upper teeth especially at the anterior region. Such difference might be due to the multiple factors as high as fermium attachment, traumatic tooth brushing and also could be related to the characteristics of the keratinized mucosa, which is wider and/or probably thicker in the maxilla than in the mandible where a strong correlation has been observed between the quantity and quality of gingival tissue 1,4,9. The recession on anterior teeth was 25.7% which is more than that on posterior teeth (3.0%). This might be related to many factors such as anterior teeth crowding, trauma from occlusion and shallow vestibule in anterior region. The percentage of recession in the anterior and posterior teeth together was 31.7%. This result might be related to the chronic periodontitis and kat chewing by the posterior teeth and to the accumulated kat leaves in the vestibule at the posterior region either in the left or right side. This might cause the gingival recession to occur as result of the pressure and mechanical effect on the gingiva 5,6. For the etiological factors which often play a significant role as a determinant of gingival recession, our study demonstrated that there is a strong and highly significant relationship (p<0.000) between the gingival recession occurrence and those factors considered in this study. These factors are the periodontitis which was shown to be the most effective factor 4, crowding teeth, malpostion teeth 4,11, high fermium attachment 6, khat showing 5 and traumatic tooth brushing 1. This result is in agreement with other study which indicated that the gingival recession may occur due to one or more than one of the above mentioned etiological factors 8. For smoking, the current study found that there is a strong correlation between smoking and gingival recession occurrence despite the fact that the number of participants of smokers was only thirty 6,11.
Conclusion
The current study concluded that, the prevalence of gingival recession among adult Yemeni population is considered high (60.5%). This recession in females (33.6%) was higher than that in males (26.9%). The percentage of gingival recession in the labial aspect (44.5%) was higher than that in the lingual sites and the recession in the anterior teeth was seen to be more than that of the posterior teeth. The prevalence, extension and severity observed in older subjects. This study indicated also that poor oral hygiene, destructive periodontitis and khat chewing appeared to be the most etiological factors causing the gingival recession among Yemeni population.
References
1. Addy M, Mostafa P, Newcombe RG. Dentine hypersensitivity: the distribution of recession, sensitivity and plaque. J Dent. 1987;15:242-8. [ Links ]
2. Albandar JM, Kingman A. Gingival recession, gingival bleeding, and dental calculus in adults 30 years of age and older in the United States, 1988-1994. J Periodontol. 1999;70(1):30-43.
3. Alldritt WA. Abnormal gingival form. Proc R Soc Med. 1968;61(2):137-42.
4. Gorman WJ. Prevalence and etiology of gingival recession. J Periodontol. 1967;38:316-22.
5. Imran AG, Murad AH. The effect of Qat chewing on periodontal tissues and buccal mucous membrane. Damascus Univer J. 2009;25(1):493-504.
6. Jenkins WM, Allan CJ. Guide to periodontics. 3. ed. Oxford: Wright; 1994. p. 155-85.
7. Kalix P. Catha edulis, a plant that has amphetamine effects. Pharm World Sci. 1996:18:69-73.
8. Löe H, Anerud A, Boysen H. The natural history of periodontal disease in man: prevalence, severity, and extent of gingival recession. J Periodontol. 1992;63:489-95.
9. Mendonça JAG. Avaliação e análise das distâncias biológicas do periodonto mediante nova metodologia [tese de doutorado]. Bauru: Faculdade de Odontologia de Bauru, Universidade de São Paulo; 2001.
10. Miller Jr. PD. A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985;5(2):9-13.
11. Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc. 2003 Feb;134(2):220-5.
12. Murray JJ. Gingival recession in tooth types in high fluoride and low fluoride areas. J Periodontal Res. 1973;8:243-51.
13. Nwhator OS, Ogunbodede E, Adedigba M, Sagay D. Prognostic indicators of gingival recession in Nigeria: preliminary findings. TAF Prev Med Bull. 2010;9(3):187-94.
14. O'Leary TJ, Drake RB, Crump PP, Allen MF. The incidence of recession in young males: a further study. J Periodontol. 1971;42:264-7.
15. Sangnes G, Gjermo P. Prevalence of oral soft and hard tissue lesions related to mechanical toothcleansing procedures. Community Dent Oral Epidemiol. 1976 Mar;4(2):77-83.
16. Schamschula RG, Keyes PH, Hornabrook RW. Root surface caries in Lufa, New Guinea. I. Clinical observations. J Am Dent Assoc. 1972 Sep;85(3):603-8.
17. Smith RG. Gingival recession: reappraisal of an enigmatic condition and a new index for monitoring. J Clin Periodontol. 1997;24:201-5.
18. Susin C, Haas AN, Oppermann RV. Gingival recession: epidemiology and risk indicators in a representative urban Brazilian population. J Periodontol. 2004;75:1377-86.
19. Vehkalahti M. Occurrence of gingival recession in adults. J Periodontol. 1989 Nov;60(11):599-603.
20. Wennström JL, Lindhe J, Sinclair F, Thilander B. Some periodontal tissue reactions to orthodontic tooth movement in monkeys. J Clin Periodontol. 1987;14(3):121-9.
21. Wennström J, Piniprato GP. Terapia mucogengival. In: Lindhe J. Tratado de periodontia clínica e implantologia oral. Rio de Janeiro: Guanabara Koogan; 1999. p. 393-425.
 Correspondence:
Correspondence:
Mansour Ali S. Ataa
P.O. BOX: 87246, Thamar, Yemen
E-mail: ataaman@hotmail.com
Received for publication: January 25, 2011
Accepted for publication: March 10, 2011
