










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.3 Joinville Jul./Set. 2011
ORIGINAL RESEARCH ARTICLE
Secondary protective seal of root canal fillings performed under simulated clinical conditions
Johannes EbertI; Roland FrankenbergerII; Anselm PetscheltI; Matthias Johannes RoggendorfII
I Dental Clinic 1, Operative Dentistry and Periodontology, University of Erlangen – Nuremberg – Erlangen – Germany
II Department of Operative Dentistry and Endodontics, Dental School Philipps, University of Marburg – Marburg – Germany
ABSTRACT
Objective: This study evaluated sealing properties of root canal fillings with an additional composite barrier. The null hypothesis tested was that different sealers and different methods of sealer removal did not influence microleakage. Material and methods: Eighty extracted human molars with fully mature apices had root canal prepared to size 60 taper .02 and divided into eight groups: three experimental groups for each sealer and negative/positive control (n = 10 each). Teeth of experimental groups were mounted into the molar region of a training puppet to simulate clinical conditions. Root canals were filled with AH Plus or GuttaFlow and gutta-percha. Excess sealer was removed with: ethanol-moistened foam pellet only, additional preparation with a water-cooled diamond bur or additional etch-and-rinse procedure (37% phosphoric acid gel). All procedures were carried out until clean as judged by the naked eye. In all groups except the positive control Syntac was applied to the access cavity. Tetric flow was applied in two increments of 1 mm each. A dye penetration test was carried out by centrifugation for 3 min at 30 G within 5% methylene blue dye. Statistical evaluation was carried out with PASW 18.0 (α = 0.05). Results: Although the two sealers had different chemical composition, sealer exhibited no influence on the results, whereas technique of sealer removal did (Two-way-ANOVA, p < 0.001). Groups with "foam pellet" or "bur preparation" showed significantly more leakage than groups with "etch-and rinse" (SNK, p < 0.05). Conclusion: Applying an etch-and-rinse procedure prior to Syntac may be beneficial for the adhesive seal over root canal fillings.
Keywords: dentin bonding; dye penetration; secondary protective seal.
Introduction
When a root canal filling is completed, the situation can occur that a definitive restoration cannot be placed at once. This is the case when an endodontist refers the patient back to his general dentist or the latter does not want to go on with the final restoration because of lack of time or insecure prognosis. In the meantime, passage of microorganisms and fluid from the oral cavity along the root canal has to be prevented 19. Until now, no root canal filling method or material alone is able to hinder coronal bacterial leakage over an extended period of time. In laboratory tests, root canal fillings usually leak after one to three months of exposure to microorganisms 13,24,26,36,37. Commonly used temporary restorations are only able to prevent the penetration of bacteria for up to two weeks 4,6. Therefore, an additional "secondary protective seal" on top of root canal fillings should be immediately applied, preferably using dentin adhesives 8. This additional barrier could be shown to reduce bacterial leakage 7,12 and to improve "clinical outcome" in an animal study 41.
Dentin bonding agents are known to be technique-sensitive 22. When root canals are filled, remnants of gutta-percha and sealer are likely to contaminate surrounding dentin. Compared to adhesive luting of tooth-coloured inlays, the effect of contamination on pulp chamber dentin is not fully clarified 21. Furthermore, the removal of excess sealer and gutta-percha may be impaired by difficult access for sight and handling, especially within the molar region. Thus, the aim of the present study was to investigate the removal of excess of two commonly used sealers with different chemical compositions (AH Plus: epoxy resin; GuttaFlow: silicone) and the application of three different removal protocols prior to adhesive seal of access cavities. The clinical situation of a general dentist was to be simulated by mounting the teeth into the molar region of a training puppet and to do without the use of additional magnification. The null hypothesis tested was that neither the way of sealer removal nor the type of sealer affects coronal microleakage of the secondary protective seal and the root canal filling.
Material and methods
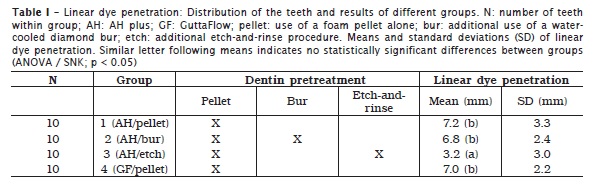
Eighty molars with fully mature apices were selected for the study. Teeth were stored in a 0.5% chloramine-T solution (Merck, Darmstadt, Germany) and used within one month after extraction. Access cavities were prepared and the lengths of the root canals recorded by passing a size 10 k-file through the apex and subtracting 1 mm. Teeth were randomly divided into six experimental groups and two control groups of ten teeth each. Distribution of groups is also shown in table I.
All root canals were instrumented to size 60 taper .02 by nickel-titanium instruments (FlexMaster, VDW, Munich, Germany). Instrumentation was accompanied by copious irrigation with 3% NaOCl and 40% citric acid. Every tooth of the experimental groups was then mounted separately into the molar region of a training puppet (KaVo, Biberach, Germany) to simulate clinical treatment conditions. A final irrigation with 40% citric acid followed by 3% NaOCl and 70% ethanol was performed (2 mL per root canal for approximately 60 s each) and the root canals were dried with paper points. For the teeth of the control groups, the same procedure was carried out, but outside the training puppet.
For each root canal, a gutta-percha cone size 55 taper .02 (Coltène-Whaledent, Langenau, Germany) was adjusted to fit with tug back at working length. Each root canal was obturated with AH Plus (Dentsply DeTrey, Konstanz, Germany) (groups 1 – 3) or GuttaFlow (Coltène Whaledent) (groups 4 – 6) using the single cone technique. All teeth of the positive control group were not filled and left open. All teeth of the negative control group were filled like in group one, including the secondary protective seal, but completely covered with nail polish. Excess gutta-percha was removed with a hot instrument at the orifice of the canals. The floor and the walls of the pulp chamber were cleaned with ethanol-moistened foam pellets until the pulp chamber appeared to be clean as judged by the naked eye.
Bur preparation
A thin layer of pulp chamber dentin was ground away with a rough water-cooled diamond bur mounted in a high-speed handpiece (KaVo, Biberach, Germany) to remove possible remnants of adhering sealer material. This procedure was carried out on teeth of groups 2 and 5 only.
Etch-and-rinse
Dentin was etched for 10 s with 37% phosphoric acid gel, rinsed with water-spray for 30 s. This procedure was carried out on teeth of groups 3 and 6 only.
Dentin bonding
Dentin was gently air-dried. Then Syntac Primer (Vivadent, Schaan, Liechtenstein) was applied for 15 s and air-dried. Then Syntac Adhesive (Vivadent) (i.e. second primer) was applied for 10 s and also dried. Finally, Heliobond (Vivadent) was applied, air-thinned, and light-cured for 40 s (Polylux II; KaVo). After adhesive pretreatment, two consecutive coats of Tetric flow were applied on the pulp chamber floor and root canal orifices and light cured 40 s each. These two layers resulted in approximately 2 mm of restorative placed onto the pulp chamber floor.
Dye penetration test
Following the completion of root canal filling and adhesive seal, each tooth was removed from the training puppet and stored in a wet chamber (37°C / 100% humidity) for one week to allow complete setting of the sealer. Afterwards, the clinical crown was cut off, leaving the adhesive seal of the root canal intact. The coronal surfaces of the specimen were gently ground flat with wet 600-grit SiC paper to expose the cross-sectional area of the adhesive seal and its transition to dentin. The roots of the teeth were covered with two layers of nail polish, leaving out the coronal surface, except for the negative controls, which were completely covered. Then the teeth were placed into test tubes together with 5% methylene blue dye solution (Merck), pipetted to a height of 30 mm. A dye-penetration test of coronal microleakage was performed using centrifugation for 3 min at 30 G (Varifuge-K, Heraeus Christ, Osterode, Germany; 400 rpm).
All specimens of each group were embedded in a resin material (Modralit-3K; Dreve Dentamid, Unna, Germany) and serial sectioned using an inner-diameter saw (Roditi, Hamburg, Germany). Transversal cuts were made perpendicular to the long axis under water cooling to obtain eight slices in distances of 1 mm.
Dye penetration was scored along the restoration-dentin interface using a microscope (Wild stereomicroscope, Leica Geosystems AG, Heerbrugg, Switzerland) at x40 magnification. Linear dye penetration was recorded using a simple yes / no decision for presence of dye for each tooth section; for example, the first plane without dye being at 3 mm from the coronal aspect was counted as 3 mm of linear dye penetration. The maximum value possible for linear dye penetration was defined as 9 mm, when dye was still present at the level of 8 mm from the coronal aspect.
Data were statistically analyzed with PASW 18.0 (SPSS Inc., Chicago, IL, USA), using Kolmogorov-Smirnov tests, one-way ANOVA with Student-Newman-Keuls (SNK) post hoc-test and two-way-ANOVA. The level of significance was set at α = 0.05.
Results
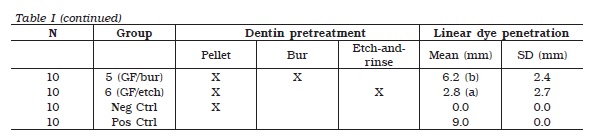
All specimens of the positive control group displayed dye penetration along the entire length of the root canal, whereas none of the specimen of the negative control group showed any coloration. Results for dye penetration are presented in table I. Kolmogorov-Smirnov-tests revealed normal distribution for all experimental groups (p > 0.05). Thus, parametric tests were applied. Statistically significant differences between all groups were identified (one-way-ANOVA, p < 0.001). The sealer material exhibited no influence on the results (two-way-ANOVA, p = 0.57), but the method of cleaning the access cavity did (two-way-ANOVA, p < 0.001). Groups 3 and 6 (etch-and-rinse) showed significantly less leakage than the other groups (SNK, p < 0.05). Between groups 3 and 6 as well as among groups 1, 2, 4 and 5, no significant differences could be found (SNK, p > 0.05).
Discussion
Statistical analysis detected a significant impact of the way of pretreatment. Thus, the null hypothesis was rejected for this aspect. Regarding the influence of sealer, the null hypothesis was confirmed.
Looking on leakage tests in general, a debate is going on whether these tests are of any worth at all 15,38, based on the findings of Oliver and Abbott 30 who revealed no correlation between clinical success and apical dye leakage. However, the sealing ability remains an important issue 38, so leakage tests for new materials and methods in the field of endodontics are still needed.
The value of bacterial leakage tests, like the ones mentioned in the introduction, was challenged within a recently published review article 31. The critic stated that the question whether the bacteria pass along the root canal filling or a different route, for example between the isolation and the outer root surface, is still not answered. However, it is unlikely that statistically significant differences within some of these studies appear with the same outer isolation of the roots, irrespective of the different root canal fillings evaluated. So, until these points of criticism are clarified, we should not disregard the results of these studies.
The fluid movement model is another possible method that is used frequently for apical leakage testing in endodontics 39. It was also successfully used to evaluate the seal of an intraorifice composite barrier 23. However, these tests were carried out without using a sealer, which is not the situation within endodontic treatment, where a combination of sealer and cones is required 19. Sealers can cause contamination of the dentinal surface and impair proper bonding to this tooth structure 25. Within the present study, this aspect – contamination with sealer – was to be tested. A combined system of root canal filling and adhesive seal was created. By use of the fluid movement model, a poor coronal seal may have been masked by a good seal of the root canal filling. Dye penetration tests enable the detection of areas of leakage and their extent. Therefore, when visualization of leakage is needed, dye penetration tests may be preferred, like in previous studies on coronal leakage of additional barriers over root canal fillings 17,18.
Dye penetration tests are relatively easy to carry out 11,34. Methylene blue is a small molecule that penetrates further than other dyes 1 and radioisotopes 27. It was also shown that dye penetration tests allow better distinction between groups than bacterial leakage tests 5, and that dye leakage can be found in bacterial leakproof root canal fillings 16. The method of dye extraction was also recommended to get over the lack of revealing significantly different results found for the classical passive dye leakage test using methylene blue 11. However, in recently published studies using the same method as the present study, significant differences between groups could be revealed 17,18,32. Thus, coronal dye penetration with methylene blue was chosen for this study. Another possible argument against methylene dye leakage tests is that studies may reveal misleading results when utilizing methylene blue in conjunction with various sealers 35. However, no difficulties were reported in this study for AH plus, one of the sealers used within the present study. The other sealer, a silicone, is known to be relatively inert to the surrounding media. The potential problem of entrapped air was addressed using a dye leakage test under centrifugation 29.
Within the present study, microleakage occurred in all groups. It is known that the dentin of the access cavity is a relatively difficult substrate to bond to, especially the pulpal floor when self-curing composites are used 2,3. Leakage may also be associated with polymerization shrinkage of Tetric flow. Further studies using other composite materials with less shrinkage are carried out at the moment to clarify whether less shrinking composites provide superior results.
Within our study, the single cone technique was used, like in some recently published studies 10,28,32,33,40. For the single cone technique, a greater amount of sealer is necessary compared to several compaction techniques. In this way, a "worst-case-scenario" should be simulated according contamination by sealer remnants. Further studies should clarify whether other root canal filling techniques may cause less microleakage of the secondary protective seal.
Within the present study, specimens leaked more than those of a comparable study in which molar teeth were also used, but not mounted into a training puppet 18. Especially the groups with foam pellet only and with the use of bur preparation showed inferior results, when compared with this previous study 18. This may be due to the fact that when the sight is impaired, this will more likely impair cleaning with the pellet and dentin pretreatment by bur preparation than the etch-and-rinse procedure. It may be argued whether this could be compensated by the use of a microscope. However, the use of additional magnification and illumination is not the rule for the treatment situation of a general dentist what mainly was to be simulated within the present study. The use of the microscope is also known to improve the detection rate of additional root canals 14,42, and to be a suitable tool for the detection of residual root canal filling material during retreatments 34. Furthermore, the fine motor skills, needed for the secondary protective seal with composite, were shown to be improved by magnification 9. Thus, the effect of additional magnification and illumination on the secondary protective seal should be a topic of future research.
Surprisingly, the results of the leakage test did not depend on the sealer, although materials with different chemical compositions were used. In agreement with previous studies 17,18, the application of an etch-and-rinse procedure facilitated a good coronal seal against ingress of dye, which may be due to a greater surface area available after etching 20. Before general recommendations can be given, studies including other sealers and other dentin bonding agents as well as other methods of leakage testing have to be carried out.
Conclusion
Within the present study, the chemical composition of the sealers had no effect on coronal microleakage of adhesively sealed, root-filled teeth. An etch-and-rinse protocol may be useful for cleaning the access cavity within the clinical situation.
References
1. Ahlberg KM, Assavanop P, Tay WM. A comparison of the apical dye penetration patterns shown by methylene blue and India ink in root-filled teeth. Int Endod J. 1995;28(1):30-4. [ Links ]
2. Akagawa H, Nikaido T, Burrow MF, Tagami J. Influence of cavity configuration on the adhesion of two resin-based composites to pulpal floor dentin. Am J Dent. 2005;18(4):233-6.
3. Akagawa H, Nikaido T, Takada T, Burrow MF, Tagami J. Shear bond strengths to coronal and pulp chamber floor dentin. Am J Dent. 2002;15(6):383-8.
4. Balto H, Al-Nazhan S, Al-Mansour K, Al-Otaibi M, Siddiqu Y. Microbial leakage of Cavit, IRM, and Temp Bond in post-prepared root canals using two methods of gutta-percha removal: an in vitro study. J Contemp Dent Pract. 2005;6(3):53-61.
5. Barthel CR, Moshonov J, Shuping G, Ørstavik D. Bacterial leakage versus dye leakage in obturated root canals. Int Endod J. 1999;32(5):370-3. 6. Barthel CR, Strobach A, Briedigkeit H, Göbel UB, Roulet JF. Leakage in roots coronally sealed with different temporary fillings. J Endod. 1999;25(11):731-4.
7. Barthel CR, Zimmer S, Wussogk R, Roulet JF. Long-term bacterial leakage along obturated roots restored with temporary and adhesive fillings. J Endod. 2001;27(9):559-62.
8. Belli S, Zhang Y, Pereira PN, Özer F, Pashley DH. Regional bond strengths of adhesive resins to pulp chamber dentin. J Endod. 2001;27(8):527-32.
9. Bowers DJ, Glickman GN, Solomon ES, He J. Magnification's effect on endodontic fine motor skills. J Endod. 2010;36(7):1135-8.
10. Brackett MG, Martin R, Sword J, Oxford C, Rueggeberg FA, Tay FR et al. Comparison of seal after obturation techniques using a polydimethylsiloxane-based root canal sealer. J Endod. 2006;32(12):1188-90.
11. Camps J, Pashley D. Reliability of the dye penetration studies. J Endod. 2003;29(9):592-4.
12. Çelik EU, Yapar AG, Ateş M, Şen BH. Bacterial microleakage of barrier materials in obturated root canals. J Endod. 2006;32(11):1074-6.
13. Chailertvanitkul P, Saunders WP, MacKenzie D. Coronal leakage of obturated root canals after long-term storage using a polymicrobial marker. J Endod. 1997;23(10):610-3.
14. Coutinho Filho T, Cerda RS, Gurgel Filho ED, de Deus GA, Magalhães KM. The influence of the surgical operating microscope in locating the mesiolingual canal orifice: a laboratory analysis. Braz Oral Res. 2006;200(1):59-63.
15. De Deus G. New directions on old leakage methods. Int Endod J. 2008;41(8):720-1.
16. De Deus G, Leal F, Soares J, Luna AS, Murad C, Fidel S et al. Dye extraction results on bacterial leakproof root fillings. J Endod. 2008;34(9):1093-5.
17. Ebert J, Frankenberger R, Karl C, Petschelt A, Roggendorf MJ. Adhesive coronal seal of Syntac and Tetric flow following different dentine pretreatment protocols. RSBO. 2010;7(4):439-44.
18. Ebert J, Löffler C, Roggendorf MJ, Petschelt A, Frankenberger R. Adhesive sealing of the pulp chamber following endodontic treatment: influence of thermomechanical loading on microleakage. J Adhes Dent. 2009;11(4):311-7.
19. European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006;39(12):921-30.
20. Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjör IA. Bonding to root canal: structural characteristics of the substrate. Am J Dent. 2000;13(5):255-60.
21. Frankenberger R, Krämer N, Lohbauer U, Nikolaenko SA, Reich SM. Marginal Integrity: is the clinical performance of bonded restorations predictable in vitro? J Adhes Dent. 2007;9(Suppl 1):107-16.
22. Frankenberger R, Krämer N, Petschelt A. Technique sensitivity of dentin bonding: effect of application mistakes on bond strength and marginal adaptation. Oper Dent. 2000;25(4):324-30.
23. Galvan Jr. RR, West LA, Liewehr FR, Pashley DH. Coronal microleakage of five materials used to create an intracoronal seal in endodontically treated teeth. J Endod. 2002;28(2):59-61.
24. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed obturated root canals. J Endod. 1993;19(9):458-61.
25. Macchi RL, Capurro MA, Herrera CL, Cebada FR, Kohen S. Influence of endodontic materials on the bonding of composite resin to dentin. Endod Dent Traumatol. 1992;8(1):26-9.
26. Magura ME, Kafrawy AH, Brown Jr. CE, Newton CW. Human saliva coronal microleakage in obturated root canals: an in vitro study. J Endod. 1991;17(7):324-31.
27. Matloff IR, Jensen JR, Singer L, Tabibi A. A comparison of methods used in root canal sealability studies. Oral Surg Oral Med Oral Pathol. 1982;53(2):203-8.
28. Monticelli F, Sadek FT, Schuster GS, Volkmann KR, Looney SW, Ferrari M et al. Efficacy of two contemporary single-cone filling techniques in preventing bacterial leakage. J Endod. 2007;33(3):310-3.
29. Oliver CM, Abbott PV. Entrapped air and its effects on dye penetration of voids. Endod Dent Traumatol. 1991;7(3):135-8.
30. Oliver CM, Abbott PV. Correlation of clinical success and apical dye penetration. Int Endod J. 2001;34(8):637-44.
31. Rechenberg D-K, De Deus G, Zehnder M. Potential systematic error in laboratory experiments on microbial leakage through filled root canals: review of published articles. Int Endod J. 2011;44(3):183-94.
32. Roggendorf MJ, Ebert J, Petschelt A, Frankenberger R. Influence of moisture on the apical seal of root canal fillings with five different types of sealer. J Endod. 2007;33(1):31-3.
33. Sagsen B, Er O, Kahraman Y, Orucoglu H. Evaluation of microleakage of roots filled with different techniques with a computerized fluid filtration technique. J Endod. 2006;32(12):1168-70.
34. Schirrmeister JF, Hermanns P, Meyer KM, Goetz F, Hellwig E. Detectability of residual Epiphany and gutta-percha after root canal retreatment using a dental operating microscope and radiographs – an ex vivo study. Int Endod J. 2006;39(7):558-65.
35. Souza EM, Pappen FG, Shemesh H, Bonanato-Estrela C, Bonetti-Filho I. Reliability of assessing dye penetration along root canal fillings using methylene blue. Aust Endod J. 2009;35(3):158-63.
36. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally unsealed endodontically treated teeth. J Endod. 1990;16(12):566-9.
37. Wolanek GA, Loushine RJ, Weller RN, Kimbrough WF, Volkmann KR. In vitro bacterial penetration of endodontically treated teeth coronally sealed with a dentin bonding agent. J Endod. 2001;27(5):354-7.
38. Wu MK. Response to: new directions in old leakage methods. Int Endod J. 2008;41(8):721-3.
39. Wu MK, De Gee AJ, Wesselink PR, Moorer WR. Fluid transport and bacterial penetration along root canal fillings. Int Endod J. 1993;26(4):203-8.
40. Wu MK, van der Sluis LW, Wesselink PR. A 1-year follow-up study on leakage of single-cone fillings with RoekoRSA sealer. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101(5):662-7.
41. Yamauchi S, Shipper G, Buttke T, Yamauchi M, Trope M. Effect of orifice plugs on periapical inflammation in dogs. J Endod. 2006;32(6):524-6.
42. Yoshioka T, Kobayashi C, Suda H. Detection rate of root canal orifices with a microscope. J Endod. 2002;28(6):452-3.
 Correspondence:
Correspondence:
Johannes Ebert
Dental Clinic 1 – Operative Dentistry and Periodontology, Glueckstr. 11,
91054 – Erlangen – Germany
E-mail: ebert@dent.uni-erlangen.de
Received for publication: March 28, 2011
Accepted for publication: April 15, 2011
