










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.4 Joinville Out./Dez. 2011
ORIGINAL RESEARCH ARTICLE
Study of position and eruption of lower third molars in adolescents
Eduardo Machado VilelaI; Paula Amorim VitoiII
I Department of Dentistry, Positivo University – Curitiba – PR – Brazil
II Buccomaxillofacial Surgery and Traumatology Service of the "Hospital Cidade Jardim" – Goiania – GO – Brazil
ABSTRACT
Introduction: The occurrence of retained lower third molars (3M) is common. A careful analysis is necessary for proper clinical management and the radiographic examination is fundamental. The use of panoramic radiographs is extremely important for the analysis and classification of 3M position, allowing the diagnosis and the establishment of the treatment planning for the removal of these teeth. Objective: The aim of this study was to evaluate the changes in position and eruption state of lower 3M during a period of 3.6 years, as well as to identify factors that may be related with early diagnosis of dental retention of these teeth in adolescent patients. Material and methods: One hundred and one initial (T1) and final (T2) panoramic radiographs from patients treating at the university's orthodontic clinics were analyzed. The distribution of 195 lower 3Ms was evaluated taking into account personal data, collected from clinical records. The data obtained in relation to the positioning of the teeth were based on the ratings of Winter and Pell & Gregory. Results: The results showed that vertical position was the most prevalent and the C level and class II positions were predominant. The changes occurring in 3M position during the study interval were not statistically significant. Conclusion: After the final evaluation (T2) it was concluded that unpredictable changes in lower 3Ms position and eruption may occur. The variables race (P = 0.03) and anterior border of the mandibular ramus (P = 0.007) seem to have influence on the level of eruption, also suggesting influence on this tooth retention within dental arches over the years.
Keywords: third molar; tooth eruption; retention.
Introduction
The stomatognathic system as well as other organic systems underwent several modifications during human beings' evolution. Consequently, alterations in all this system's components, particularly the teeth, occurred. There has been a reduction in dental arches' length and in tooth amount, culminating in the almost disappearing of fourth molars (currently seen as supernumerary teeth); bicuspid and third molar anodontia; and tooth retentions, which are even more frequently. Additionally to the phylogenetic causes, systemic and local factors of the person itself may account for tooth retention. Concerning to systemic factors, the diseases interfering in human body development, such as: rickets, hormonal dysfunction, congenital syphilis, tuberculosis, progeria, achondroplasia, mongolism, cleidocranial dysostosis, among others play an important role. Local causes are represented by mechanical obstructions, such as lack of space, eruption path, tissue degenerations, tooth anomalies itself (root dilaceration and macrodontia, for example), among others 24.
The denomination "unerupted tooth" is given to a tooth totally covered by bone and/or mucous tissue, which can be only visualized through auxiliary tools of diagnosis, such as radiographs and tomographies, despite of either being at physiologic eruption process or undergoing any physical obstruction that interferes in its eruption 22.
A tooth is so-called "retained" when it reaches the normal period of eruption and it stays partial or totally closed within the bone with or without maintaining tooth pericoronary sac integrity. This retention may be presented in two forms: tooth completely involved by bone (intrabony retention); tooth partial or completely covered by gingival mucosa (subgingival retention). Still, it may be partially retained with the disruption of tooth pericoronary sac (semi-retained). In addition to bony and soft-tissue retentions, the tooth also can be either impacted – with intimate relation with the neighboring teeth – or embedded – without contact with the neighboring teeth. Also, the tooth can be retained physiologically due to pathological alteration (bone thickness increasing), lack of space to erupt, and/or neoplasias 6,12.
The most frequently retained teeth are 3Ms (90%), with higher prevalence in mandible (60%) than maxilla (30%), followed by upper canine teeth (5%), lower bicuspids and supernumerary teeth (5%).
Upper and lower 3Ms are the last teeth to erupt, regardless race and gender, and normally do not erupt at occlusal plane until mandibular growth is complete 14,19,26. Third molar crown formation begins around 9 to 10 years of age and may be seen in panoramic radiograph, in about 90% of the cases, at 11 years of age. Its eruption period is very variable, initiating at 16 years of age. However, it more frequently erupts between 18 and 20 years of age 14.
The highest retention incidence of 3Ms, especially those located in mandible, results in a large number of studies because of their position variations, higher surgical treatment challenges, and their more frequent association to pathologies 5,7,22,24.
If retained teeth are left within the alveolar ridge, it is likely that one or more problems occur and the patient may present a higher incidence of local tissue morbidity, such as bone and neighboring tooth loss and potential lesion to the surrounding vital structures 16. Among the complications, the most important and common are pericoronaritis and the formation of odontogenic cists and tumors arising from dental follicle. Therefore, it is important the evaluation of the state of third molars, to prevent the aforementioned and other complications, such as periodontal disease, dental caries, root resorption, and mandibular fractures 1,2,14.
Among the auxiliary tools for the visualization and diagnosis of retained third molars, panoramic radiograph plays a fundamental role in the observation of all maxilomandibular complex structures. By using this technique, one can not only diagnose these teeth, but also perform an accurate treatment planning for each type of angulation and position of these teeth 6. Panoramic radiograph also employs only one pellicle, during a short time period, and with short biological exposure to radiation, and is of great value for an early interpretation or screening test 9.
Also, panoramic radiographs are becoming increasingly viable for dentists and they help in the evaluation of third molar development. This radiograph type enables a general view of dental arches' structures, facilitating the analysis and classification of third molar positions 10,11,18,21.
Aiming to make treatment planning easy, some classification systems have arisen to allow the anticipation of possible disorders and the prediction of some modifications during the operative act. Such classifications were based on the radiographic analysis, and most of times they use panoramic radiographs, by which is possible to visualize properly the second molar's long axis as a parameter. Winter's classification evaluates the retained 3M long axis in relation to second molar long axis, in the following positions: vertical, mesio-angular, disto-angular, horizontal, inverse, buccal/lingual obliquity (transverse) 6,10,22,24. Pell and Gregory's classification considers the bone deepness in which the retained 3M is found (A, B, C positions) and the space existing between the second molar's distal surface and the ramus of the mandible (class I, II, III) 10,14,22.
Concerning to tooth retention, it is necessary to execute a correct diagnosis, aiming to perform the surgical procedure, unless there would be specific contraindications to this treatment 23.
Tsai 23 conducted a retrospective study using panoramic radiographs of 52 patients (72 male and 80 female) to assess the eruption and the retention of lower 3M. Differences between non-retention and retention groups were analysed and the variables describing spaces between the anterior portion of the mandibular ramus and the lower second molar distal surface as well as the tooth sizes seemed to be the main contributing factors to the differences observed by the author.
Niedzielska et al. 15 investigated 64 patients, what measurements on panoramic radiographs could facilitate the prognosis of lower 3M position in dental arch. The authors observed that the measurements of the retromolar space and the third molar's angulation in relation to the mandible basis and to second molar may help the prognosis.
Considering the aforementioned discussion and the possible use of the panoramic radiograph as an auxiliary tool for visualizing the morphological and positioning characteristics of lower 3M, this study aimed to assess the changes occurring in the position and eruption of lower 3M as well as to identify the factors that may be related to the early diagnosis of this tooth retention in adolescents, by using patient's radiographic images and clinical features obtained through orthodontic documentation.
Material and methods
Panoramic radiographs of 101 patients who undergone orthodontic treatment at the Clinics of Specialization in Orthodontics (School of Dentistry, Federal University of Juiz de Fora) and at the Clinics of Dentofacial Correction (Clidef) were employed. We used the panoramic radiographs of the beginning of the orthodontic treatment (T1), as part of the initial orthodontic documentation required for both the orthodontic diagnosis and treatment, and after a treatment period of 3.6 years (T2).
On one hand, inclusion criteria comprised 6,18:
• both genders;
• age ranging from 12 to 26 years (we did not include children under 12 years-old because it is difficult to perform measurements on the third molar bud, at this early age);
• presence of at least one lower 3M, erupted or not;
• presence or absence of bicuspids. On the other hand, exclusion criteria were composed of 3,4,17:
• patients presenting any dentofacial deformity;
• patients presenting congenital or syndromic diseases;
• absence of lower second molar.
Data regarding to patients' clinical features were obtained from the orthodontic documentations and registered on standardized tables.
The panoramic radiographs were analysed by one single examiner properly calibrated, on a standard light-box, in a darkened room.
Initial panoramic radiographs were analysed according to the degree of angulation of Winter's classification. According to Pell and Gregory, the anterior border of the ramus of the mandible was evaluated, relating it to 3M's mesiodistal diameter; also, the level of eruption (position) was assessed by comparing 3M occlusal surface height regarding to the cervical surface of the adjacent second molar.
After 3.6 year follow-up, other radiographs were obtained and evaluated similarly to the initial radiographs.
For Winter's classification 3M positions were evaluated in relation to the adjacent second molar's long axis. By using a protractor, the angle formed between the aforementioned long axes was measured. We considered 23:
• Disto-angular teeth with angles from -30º to -5º;
• Vertical teeth with angles from -5º to 5º;
• Mesio-angular teeth with angles from 5º to 55º;
• Horizontal teeth with angles from 55º to 105º. We did not considered in this study the buccal/lingual obliquity (transverse), because we would need an occlusal radiograph to confirm this position. For Pell and Gregory's classification, we verified the A, B, and C positions as well as class I, II, and III, as follows:
• Position in relation to the occlusal plane: − A: 3M occlusal surface is above or at the level of the second molar's occlusal surface; − B: 3M occlusal surface is between the cervical and occlusal surface of the second molar; − C: 3M occlusal surface is below the second molar's cervical surface.
• Position in relation to the anterior border of the ramus of the mandible: − Class I: the distance between the second molar's distal surface and the anterior border of the ramus of the mandible is greater than 3M mesiodistal diameter; − Class II: the distance between the second molar's distal surface and the anterior border of the ramus of the mandible is smaller than 3M mesiodistal diameter; − Class III: there is no space between the second molar's distal surface and the anterior border of the ramus of the mandible.
The differences between the radiographic obtained at the treatment beginning (T1) and after 3.6 years (T2) were analysed.
This present study was approved by the Ethical Committee in Research on Human Beings of Federal University of Juiz de Fora, in May 15, 2010, protocol number #125/2010.
Results
Two hundred and two panoramic radiographs were analysed, of which 101 before orthodontic treatment (T1) and 101 after a time period of about 3.6 years (T2). The studied found 195 lower 3M of patients aging from 12 to 26 years (T1 mean age: 13.72 years; T2 mean age: 17.35 years).
During this period, 23 (11.87%) of the 195 lower 3M present in the initial radiographic documentation were extracted.
Of the remaining 172 lower 3M, 163 and 148 were totally or partially unerupted at T1 and T2, respectively.
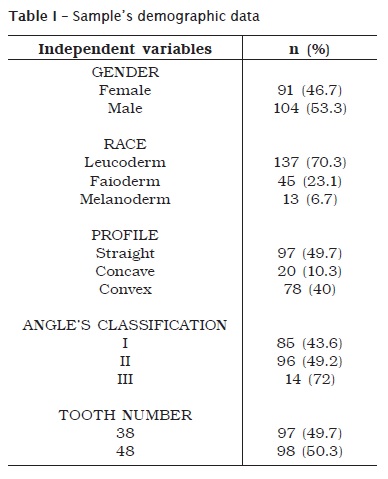
Table I shows the distribution of the 195 lower 3M in relation to the variables: gender, race, profile, Angle's classification and number of teeth.
Tables II and III respectively show the changes occurring in angulation (P > 0.05) and in relation to the anterior border of the ramus of the mandible (P > 0.05) of lower 3M during 3.6 year time period of observation by McNemar-Bowker test.
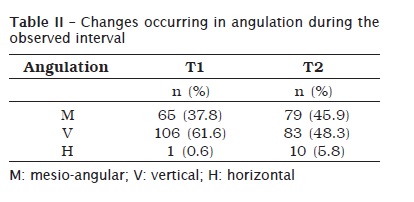
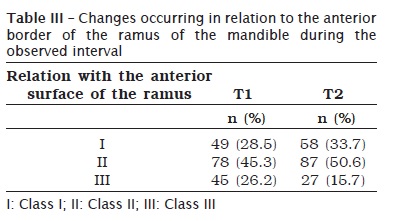
Table IV presents the distribution of the level of final eruption (T2) according to the variables gender (P > 0.05) and race (P = 0.03) obtained by Pearson Chi-Square test.
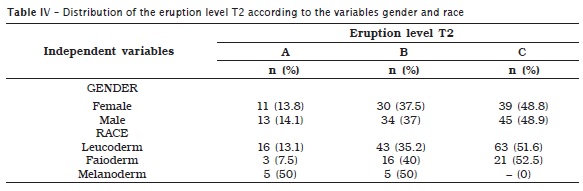
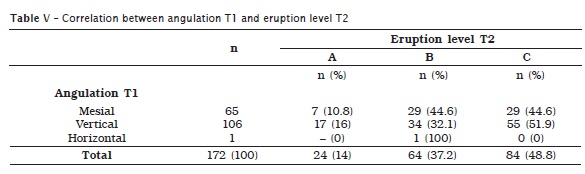
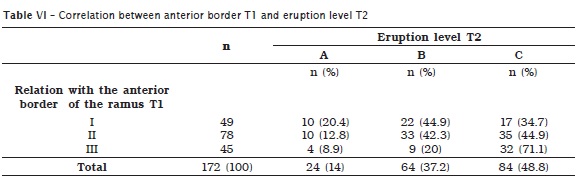
Table V and VI, respectively, indicate the radiographic angulation features initially obtained (P > 0.05) and the relationship with the anterior border of the ramus of the mandible (P = 0.007) with final eruption level (T2) of lower 3M, obtained by Pearson Chi-Square test.
Discussion
According to Mollaoglu et al. 13 and Santos and Quesada 22, the chronology of permanent tooth eruption shows that the last tooth group to erupt is 3Ms. Therefore, in association to arch length incompatibility, it is the tooth group most frequently retained. Sandhu and Kaur 20 reported that lower 3Ms account for about 98% of tooth retention. These authors emphasized that due to an increase of incidence of unerupted 3M and their association to numerous complications, early evaluation of 3M tooth bud as well as the prognosis of its eruption is necessary for a better patient's treatment planning.
This study's methodology of choice comprised the retrospective assessment of radiographic images and clinical features of patients orthodontically treated during 3.6 year period, as well as other studies 3,4,8,15,20,28,29. Sant'Ana et al. 21 and Yazdani et al. 31 emphasized that although panoramic radiographs have been largely employed to determine lower 3M positions, they show limitations and possible distortions. Notwithstanding, this distortion represents a negligible value for 3M diagnosis and surgical planning.
Of 172 lower 3M classified according to Winter at T1, we observed the vertical position as the most prevalent POSITION followed by mesio-angular and horizontal. This occurrence order was maintained during T2 analysis. Considering such outcomes, Sandhu and Kaur 20 observed in 72 retained lower 3M that 50% were at vertical position, 33.3% at mesio-angular position, and 17% at disto-angular. Moreira et al. 14 also presented similar results: 45.22% of the teeth were at vertical position, followed by 29.57% at mesio-angular position. Santos and Quesada 22 conducted a study in which 46.6% of the analysed lower 3M were at vertical position, 43.8% at mesio-angular position, 9% at horizontal position, and 0.6% at disto-angular position. Contrastingly, Marinho et al. 10 verified that the mesio-angular position was the most frequent (33%), followed by vertical position (27%). Quek et al. 17 found in a study with 1,000 panoramic radiographs that mesio-angular position was the most prevalent, corresponding to 60%. Sandhu and Kaur 19 analysed 100 radiographs and also found the mesio-angular position (49%) as the most frequent, followed by vertical (42%) and disto-angular (9%). Similarly, Dias-Ribeiro et al. 6, Lopes et al. 9, Santos Júnior et al. 24 and Venta et al. 30 reported the mesio-angular position as the most prevalent. In our study, 65 (37.8%) 3M presented angulation changes, and 107 (62.2%) maintained the initial angulation, during the follow-up period of 3.6 years. Angulations changes from T1 to T2 were not statistically significant. Sandhu and Kaur 20 observed that 15% of lower 3M changed angulation during a follow-up period of 4 years. According to Venta et al. 30 the percentage of 3M with angulation changes was 76% during a follow-up period from 20 and 32 years of age.
According to Pell and Gregory classification (relation to the anterior border of the ramus of the mandible), class II was the most frequently found in 172 lower 3M evaluated at T1, followed by class I and III. A similar frequency order was maintained during T2 analysis. Corroborating these results, Marinho et al. 10 evaluated 464 lower 3M, of which 84% (389 teeth), 11% (52 teeth) and 5% (23 teeth) were classified as class II, I, and III, respectively. These results meet those found by Santos and Quesada 22, in which the occurrence descending order was class I, II, and III. Santos et al. 23 observed the class III (46.6%) as the most frequent position followed by class I (37.5%) and II (15.9%). Moreira et al. 14 reported a prevalence of 72.5% of class III, 15.7% and 11.8% of class I and II, respectively. In our study, 79 (45.9%) 3M showed classification changes in relation to the anterior border of the ramus and 93 (54.1%) maintained the initial classification after the follow-up period of 3.6 years. However, these changes were not statistically significant.
During the follow-up period of 3.6 years, 24 (13.9%) 3M erupted at the occlusal plane (level A), and 148 (86%) were totally or partially unerupted (level C and B respectively). Also, 39% of the evaluated teeth showed changes in the eruption levels after the final assessment and 61% maintained the initial position. In the study of Venta et al. 30, the eruption state also presented alteration in about 44% of the teeth analysed.
Concerning to the eruption level (A, B, and C) according to Pell and Gregory's classification, patient's gender did not influenced the prevalence of 3M eruptions. Corroborating this result, Sousa Filho et al. 25 did not found a statistically significant relationship between gender and eruption level of these teeth. However, Marinho et al. 10 reported a slight predominance of male (52%). Santos et al. 23 and Toledo et al. 26 observed a prevalence of retained 3M in female with 77.3% and 56.5%, respectively. In our study, the variable race revealed statistically significant in the classification of the eruption level of these teeth. The occurrence decreasing order in leucoderm and faioderm was C, B, and A. In melanoderm patients, the most frequent positions were A and B (50% each). We did not found totally erupted 3M (C position) in this study in melanoderm patients. Race was not included as a variable in the methodologies of the studies verified by us.
Of 49 3M initially classified as class I, 39 (79.6%) was kept partial or totally unerupted (B level: 44.9%; C level: 34.7%) and 20.4% (10 teeth) totally erupted at occlusal plane (A level). Of 78 3M initially classified as class II, 67 (87.2%) was kept unerupted (B level 42,3%; C level: 44,9%) and 12.8% (10 teeth) totally erupted at occlusal plane (A level). And of 45 3M initially classified as class I, 41 (91.1%) was kept unerupted (B level: 20%; C level: 71,1%) and 8.9% (4 teeth) completely erupted at occlusal plane. Complete eruption (level A) occurred predominantly in patients initially classified as class I, where there is enough space for this event takes place, followed of those previously classified as class II and III, respectively.
Although the importance of 3M extraction is recognized in preventing possible complications, our study could not determine the dentist's conduct regarding the indication or even extraction of retained or impacted 3M (86%) found at T2.
Conclusion
The results of our study showed that vertical, class II, and C level positions were the most prevalent. During the study period we found changes in lower third molar positions although without statistically significant differences, maintaining the positions initially found at T1. At T2, we concluded that unpredictable changes in position and angulation of lower 3Ms can occur.
Although this study could not determine the early diagnosis of lower third molar retention, it was possible to infer that tooth retention occurs with smaller frequency in melanoderm patients showing class I 3M. Therefore, the variables race and anterior border of the ramus of mandible seemed to influence on the eruption level and the retention of these teeth within arch, over the time.
References
1. Adeyemo WL. Do pathologies associated with impacted lower third molars justify prophylactic removal? A critical review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endo. 2006 Aug;102(4):448-51. [ Links ]
2. Akarslan ZZ, Kocabay C. Assessment of the associated symptoms, pathologies, positions and angulations of bilateral occurring mandibular third molars: is there any similarity? Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Sep;108(3):26-32.
3. Artun J, Thalib L, Robert Little M. Third molar angulation during and after treatment of adolescent orthodontic patients. European Journal of Orthodontics. 2005 Jul;27:590-6.
4. Behbehani F, Artun J, Thalib L. Prediction of mandibular third molar impaction in adolescent orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics. 2006 Jul;130:47-54.
5. Castella P, Albright Jr RH, Straja S, Tuncay OC. Prediction of mandibular third molar impaction in the orthodontic patient from a panoramic radiograph. Clin Orthod Res. 1998 Aug;1:37-43.
6. Dias-Ribeiro E, Lima-Júnior JL, Barbosa JL, Haagsma IB, Lucena LBS, Marzola C. Avaliação das posições de terceiros molares retidos em relação à classificação de Winter. Rev Odont Unesp. 2008;37(3):203-9.
7. Golovcencu L, Anistoroaei D. Considerations regarding a prediction method for third mandibular molar eruption. Rev Med Chir Soc Med Nat Iasi. 2007 Oct-Dec;111(4):1052-5.
8. Hattab FN. Positional changes and eruption of impacted mandibular third molars in young adults. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997 Dec;84(6):604-8.
9. Lopes PM, Sales MAO, Freitas CF, Panella J. Estudo radiográfico da posição e da situação dos terceiros molares no complexo maxilo-mandibular, por meio de ortopantomografias. 2004 [cited 2010 Aug 5]. Available from: URL:http://www.patologiaoral.com.br/texto64.asp.
10. Marinho SA, Verli FD, Amenábar JM, Brücker MR. Avaliação da posição dos terceiros molares inferiores retidos em radiografias panorâmicas. Robrac. 2005;14(37):65-8.
11. Martinez AM, Caballero AD, Duran SS. La radiografia panoramica una herramienta para identificar los factores que determinan la erupcion de los terceros molares mandibulares asintomáticos – reporte de una investigacion. Acta Odontológica Venezolana. 2005;43(3) [cited 2010 Aug 1]. Available from: URL:http://www.actaodontologica.com/ediciones/2005/3/radiografia_panoramica.asp.
12. Marzola C. Retenção dental. 2. ed. São Paulo: Pancast; 1995. 338 p.
13. Mollaoglu N, Cetiner S, Gungor K. Patterns of third molar impaction in a group of volunteers in Turkey. Clin Oral Invest. 2001 Nov;6(2):109-13.
14. Moreira BF, Picorelli NMS, Visconti Filho RF, Paula MVQ, Chaoubah A, Maior BSS. Avaliação radiográfica dos terceiros molares em alunos da graduação da Faculdade de Odontologia da UFJF. HU. 2007 Jul-Sep;33(3):63-8.
15. Niedzielska IA, Drugacz J, Kus N, Kreska J. Panoramic radiographic predictors of mandibular third molar eruption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Aug;102(2):154-8.
16. Peterson LJ. Cirurgia oral e maxilofacial contemporânea. 4. ed. Rio de Janeiro: Elsevier; 2005. p. 197-210.
17. Quek SL, Tay CK, Tay KH, Toh SL, Lim KC. Pattern of third molar impaction in a Singapore Chinese population: a retrospective radiographic survey. Int J Oral Maxilllofac Surg. 2003;32(5):548-52.
18. Quiróz OJ, Palma A. The mandibular third molar: a method for predicting its eruption. Orthodontic Cyber Journal. 1999 [cited 2010 Jul 20]. Available from: URL:http://orthocj.com/1999/02/the-mandibular-third-molar-a-method-for-predicting-its-eruption/.
19. Sandhu S, Kaur T. Radiographic evaluation of the status of third molars in the asian-indian students. J Oral Maxillofac Surg. 2005;63(5):640-5.
20. Sandhu S, Kaur T. Radiographic study of the positional changes and eruption of impacted third molars in young adults of an asian indian population. J Oral Maxillofac Surg. 2008;66(8):1617-24.
21. Sant'Ana LF, Giglio FP, Ferreira Jr O, Sant'ana E, Capelozza AL. Clinical evaluation of the effects of radiographic distortion on the position and classification of mandibular third molars. Dentomaxillofac Radiol. 2005 Mar;34(2):96-101.
22. Santos DR, Quesada GAT. Prevalência de terceiros molares e suas respectivas posições segundo as classificações de Winter e de Pell e Gregory. Rev Cir Traumatol Buco-Maxilo-Fac. 2009 Jan-Mar;9(1):83-92.
23. Santos L, Dechiche NL, Ulbrich LM, Guariza O. Análise radiográfica da prevalência de terceiros molares retidos efetuada na clínica de odontologia do Centro Universitário Positivo. RSBO. 2006;3(1):18-23.
24. Santos Júnior PV, Marson JO, Toyama RV, Santos JRC. Terceiros molares inclusos mandibulares: incidência de suas inclinações, segundo classificação de Winter: levantamento radiográfico de 700 casos. RGO. 2007 Apr-Jun;55(2):143-7.
25. Sousa Filho G, Amorim Júnior AA, Lins CCSA, Silva Neto JC. Evaluation of dental eruption of third molars in the length of mandible. Int J Morphol. 2009;27(4):1319-23.
26. Toledo GL, Álvarez-Capelloza AL, Marzola C, Toledo-Filho JL, Capelari MM, Barbosa JL et al. Estudo da prevalência de dentes retidos através de radiografias panorâmicas digitais no município de Curitiba, Paraná, Brasil [trabalho de conclusão de curso (Especialização em CTBMF)]. Curitiba: Colégio Brasileiro de CTBMF e CFO; 2008.
27. Tsai HH. Factors associated with mandibular third molar eruption and impaction. J Clin Pediatr Dent. 2005;30(2):109-13.
28. Venta I, Murtomaa H, Turtola L, Meurman J, Ylipaavalniemi P. Clinical follow-up study of third molar eruption from ages 20 to 26 years. Oral Surg Oral Med Oral Pathol. 1991;72(2):150-3.
29. Venta I, Schou S. Accuracy of the third molar eruption predictor in predicting eruption. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001 Jun;91(6):638-42.
30. Venta I, Turtola L, Ylipaavalniemi P. Radiographic follow-up of impacted third molars from age 20 to 32 years. Int J Oral Maxillofac Surg. 2001;30(1):54-7.
31. Yazdani J, Esmaeili F, Johari M. Comparison of the inclination of unerupted mandibular third molar on panoramic radiography and casts made after surgical incision. J Dent Res Dent Clin Dent Prospect. 2009;3(3):94-7.
 Correspondence:
Correspondence:
Paula Amorim Vitoi
Rua Orozimbo Rocha, n.º 446 – Centro
CEP 36680-000 – São João Nepomuceno – MG – Brasil
E-mail: paulavitoi@yahoo.com.br
Received for publication: January 24, 2011
Accepted for publication: March 18, 2011
