










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.4 Joinville Out./Dez. 2011
ORIGINAL RESEARCH ARTICLE
Comparison of MTA Fillapex radiopacity with five root canal sealers
Ana Paula Meirelles VidottoI; Rodrigo Sanches CunhaII; Eduardo Gregatto ZeferinoI; Daniel Guimarães Pedro RochaI; Alexandre Sigrist de MartinI; Carlos Eduardo da Silveira BuenoI
I São Leopoldo Mandic Research Center – Campinas – SP – Brazil
II University of Manitoba – Winnipeg – MB – Canada
ABSTRACT
Introduction: The endodontic sealer is a filling material whose physicochemical properties are mandatory for the achievement of endodontic therapy final goal. An ideal endodontic sealer should have some properties, including radiopacity. Objective: This study compared MTA Fillapex™ radiopacity with the radiopacity of five others endodontic sealers: Endométhasone-N™, AH Plus™, Acroseal™, Epiphany SE™ and RoekoSeal™. Material and methods: Five cylindrical samples of each sealer were used, constructed with the aid of a matrix. On an occlusal film, a sample of each sealer was placed along with an aluminum stepwedge and five radiographic shots were taken. The radiographic images were digitized and each sample's gray scales were compared with each shade of the aluminum stepwedge, by using software. Results: The results, in decreasing order of radiopacity, were: AH Plus™ was statistically the most radiopaque sealer (9.4 mm Al), followed by Epiphany SE™ (7.8 mm Al), MTA Fillapex™ (6.5 mm Al), RoekoSeal™ (5.8 mm Al), Endométhasone-N™ (4.5 mm Al), and Acroseal™, the least statistically radiopaque (3.5 mm Al). Conclusion: It can be concluded that MTA Fillapex™ was the third most radiopaque sealer among all tested sealers. Also, MTA Fillapex™ has the radiopacity degree in agreement with ADA specification No. 57 (1983).
Keywords: obturation; root canal sealer; radiopacity.
Introduction
One of the key points for reaching endodontic treatment success is tridimensional obturation of root canal systems 14. Following proper shaping and cleaning phases, obturation aims to seal root canal system in order to allow a favorable environment for tissue repair as well as to avoid root canal reinfection.
The success of root canal obturation is reached not only by the technique employed, but also by the type of the material chosen for treatment 25. Although endodontic obturation is mainly constituted by gutta-percha, endodontic sealers are used aiming to decrease the gap existing among gutta-percha points themselves and gutta-percha points and root canal walls 13,14. Consequently, endodontic sealers must present some physicochemical properties to qualify them as a good material 10,13,16,18.
According to Grossman (1958) 9, the endodontic sealers, regardless of type, should exhibit some requirements, as follows: biocompatibility, easy insertion into and removal from root canal, viscosity while handling, good adhesion to root canal's walls, satisfactory handling time, promotion of a tridimensional sealing, dimensional stability, good flowing, good radiopacity, lack of color change, insolubility to tissue fluids and saliva, solubility to common solvents when necessary, impermeability, and antimicrobial activity.
ADA specification No. 57 (1983) 1 recommends that endodontic filling material's physical properties be evaluated by flowing, radiopacity, thickness, setting time, dimensional stability, solubility and disintegration tests.
Radiopacity property is important because an endodontic sealer must be radiopaque enough to be differentiated from neighboring anatomical structures (bone and tooth structures) and other dental materials (resin, amalgam, and cements) 7,11,24,28,29,30.
Mineral trioxide aggregate (MTA) is indicated for a series of applications in Endodontics: perforations sealing, pulp capping, pulpotomy, apicification, obturation, biological plug, and retro-filling material 12,31. MTA is basically composed of calcium, silica, and bismuth 29. Bismuth oxide accounts for MTA radiopacity. The new MTA-based endodontic sealer (MTA Fillapex®) composition is similarly to MTA, except from the addition of natural resin and nanoparticulate silica.
In order to use MTA Fillapex® as a new option for endodontic sealer, its physical properties must be confirmed, in agreement with the characteristics cited by Grossman (1958) 9 for the ideal sealer. The aim of this study was to compare the radiopacity of MTA Fillapex® with AH Plus®, RoekoSeal®, Epiphany SE®, Endométhasone-N® and Acroseal® radiopacity.
Material and methods
We used the following endodontic sealers Acroseal® (Septodont, France), AH Plus® (Dentsply, Konstanz, Germany), MTA Fillapex® (Angelus, Londrina, Brazil), Epiphany SE® (SybronEndo, USA), RSA RoekoSeal® (Roeko, Langenau, Germany), and Endométhasone-N® (Septodont, France).
The radiopacity test followed ANSI/ADA specification No. 57 (1983). Each endodontic sealer was manipulated according to the manufacturer's instructions. Following, with aid of a cylindrical matrix (5 mm diameter x 1 mm thickness), five samples of each endodontic sealer were constructed. Samples were kept in a heater, at 37ºC, up to the last sample construction was completed.
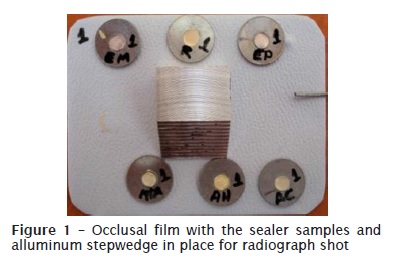
Next, each sealer sample was placed onto an occlusal film (Kodak Insight Speed E, Eastman Kodak Company, Rochester, USA) together with an aluminum 10-step wedge, each step measuring 1 mm height. Radiographs were obtained using the Gendex 765DC x-ray machine (Gendex Dental X-Ray Division, Dentsply International, Des Plaines, USA), at 65 kV, 7 mA, for 0.25 s of exposure time, and object-to-focus distance of 40 cm. Five radiographic shots were executed. One sample of each endodontic sealer and the aluminum stepwedge was placed onto the radiograph film (figure 1).
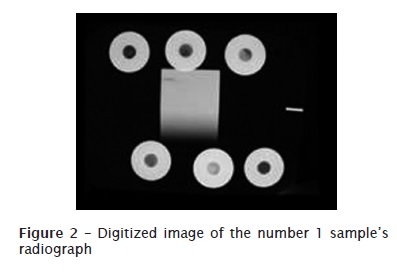
Radiograph developing/processing was performed with an automatic device (Gendex GXP, Gendex Corporation, Des Plaines, USA). The radiographs were digitized in a digital camera (Canon 50D, Canon Inc, Tokyo, Japan). The photographs were obtained in macro mode (15 megapixel resolution) and a black paper covered all the light-box border surrounding the radiograph so that no light could alter the radiograph. The camera was kept at a standardized distance to allow that only the radiograph surrounded by the black border appeared on the photograph (figure 2).
After images' digitization, areas with the same diameter of each sample and aluminum steps were compared and measured in a gray scale (0 to 255) by Adobe Photoshop version 7.0.1 software.
Data were analysed and the obtained numbers related to the gray-scale values were transformed into mm of aluminum (mm Al). Statistical analysis was performed by ANOVA by using each sealer mm Al mean.
Results
One-way ANOVA and linear regression analysis confirmed the expectations regarding to the aluminum scale with different densities from 8 to 1 mm. We verified a radiopacity decreasing while the scale density decreased. The equation observed by the linear regression analysis evidenced that the radiopacity increase was significant with the density increase (table I).
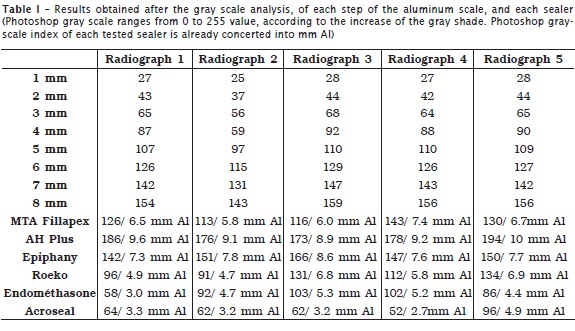
All tested sealers presented an mm-Al value above ADA requirements. ADA requirements demand that the radiopacity minimum must be above 3 mm of the aluminum stepwedge.
AH Plus® showed a mean of 9.4 mm Al significantly higher than all other sealers. Epiphany SE® exhibited a mean of 7.8 mm Al significantly smaller than AH Plus® and significantly higher than all other sealers. MTA Fillapex® and RoekoSeal® presented means of 6.5 mm Al and 5.8 mm Al, respectively, without statistically significant difference between each other; however, these values were smaller than AH Plus® and Epiphany SE®, but significantly higher than Endométhasone-N® (4.5 mm Al) and Acroseal® (3.5 mm Al). Endométhasone-N® showed a significantly higher mean than Acroseal®. This latter exhibited a significantly smaller mean than all the others.
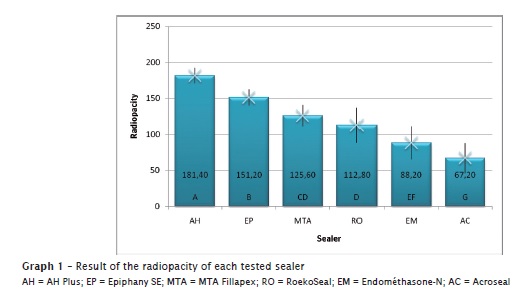
In a decreasing order of radiopacity, AH Plus® (9.4 mm Al) was the most radiopaque sealer, followed by Epiphany SE® (7.8 mm Al), MTA Fillapex® (6.5 mm Al), RoekoSeal® (5.8 mm Al), Endométhasone-N® (4.5 mm Al), and Acroseal® (3.5 mm Al) (graph 1).
Discussion
Radiopacity degree is mandatory for controlling root canal filling. A radiopaque filling material is important for its differentiation from tooth and periradicular anatomical structures, so that possible overfilling and lateral root canal filling can be controlled. Although there are specifications demanding only a minimum radiopacity limit, the extreme contrast of a material may lead to the false impression of a dense and homogenous filling 16.
Some clinical factors should be taken into account when deciding on the level of radiopacity. Bone, periodontal ligament, and dentin radiopacity presents different mm Al equivalencies. A sealer showing radiopacity above 3 mm Al is considered ideal for differentiation from, for example, lateral root canal obturation, over-filling, or anatomical structures 24.
In this study's radiopacity test, the endodontic sealers most employed in the Brazilian market were used: zinc oxide and eugenol-based sealer (Endométhasone-N®), silicon-based sealer (RoekoSeal®), calcium-hydroxide-based sealer (Acroseal®), resin-based sealer (AH Plus®), methacrylate resin-based sealer (Epiphany SE®), MTA-based sealer (MTA Fillapex®). This latter was recently launched into the Brazilian market.
Several radiopacity studies have used the aluminum stepwedge comparison with different samples 7,8,29, in agreement with this study's methodology.
In our study, we used a conventional radiograph, because literature has demonstrated that there were no differences in results when either digital or conventional image is employed 2,3,5,17. Digital or conventional radiograph analysis methodology 21,22 can be assessed by photodensitometry 20,23 and radiograph digitization for posterior computer analysis. Tagger and Katz (2003) 27 applied this methodology to analyze endodontic sealer radiopacity by using standardized samples radiographed along with an aluminum stepwedge. In this method, the radiographs are digitized, and the samples compared with the aluminum stepwedge radiopacity through computer software. The evolution of the comparison with the digital radiograph's image by applying an image analysis software makes simpler and easier the reproduction of the materials radiopacity 7,26.
Baksi et al. (2008) 3 conducted a radiopacity study in which the sealer's radiopacity was compared as well as the methodology using digital and conventional radiograph. They found that Acroseal® was the least radiopaque sealer, in agreement with our results. Additionally, these authors concluded that there was no statistically significant difference between digital and conventional methods and both were valid for determining the smallest difference of a material's radiodensity distribution, showing either a higher or a smaller density.
According to graph 1, all sealers met ADA minimum requirements. The results demonstrated that AH Plus® and Epiphany SE® exhibited radiopacity greater than the other sealers. This result is similar to those found by other authors, in literature 4,19,26,28,30, where AH Plus® showed the highest radiopacity in comparison with silicon-based, calcium hydroxide-based and zinc oxide and eugenol-based sealers.
Concerning to calcium hydroxide-based sealers, our results are in agreement with literature. These sealers are generally the least radiopaque sealers, in comparative studies 3,6,15. In our study, Acroseal® presented the smallest radiopacity.
MTA-based sealer (MTA Fillapex) exhibited a satisfactory radiopacity value (6.5 mm Al), similar to that found by Tanomaru et al. (2009) 29 with CPM Sealer® (6.3 mm Al), also a MTA-sealer.
Conclusion
According to the methodology used and the analysis of the results, it can be concluded that:
• MTA Fillapex® sealer shows the third highest radiopacity in comparison with the other tested sealers;
• MTA Fillapex® sealer has a radiopacity degree in agreement with ADA specification No. 57.
References
1. American Dental Association. Specification n. 57 for Endodontic filling materials; 1983. [ Links ]
2. Baksi BG, Eyuboglu TF, Sen BH, Erdilek N. The effect of three different sealers on the radiopacity of the root filling in simulated canal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:138-41.
3. Baksi BG, Sen BH, Eyboglu TF. Differences in aluminum equivalent values of endodontic sealers: conventional versus digital radiography. J Endod. 2008 Sep;34(9):1101-4.
4. Bodrumlu E, Sumer AP, Gungor K. Radiopacity of a new root canal sealer, epiphany. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:59-61.
5. Figueiredo JAP, Vidor MM, Oliveira FF, Filippini HF, Gomes MS. Avaliação da radiopacidade dos cimentos Sealapex e Sealer 26, com adição de iodofórmio, através de imagem digitalizada. Rev Fac Odontol Univ Fed Rio Grande do Sul. 1997 Dec;38(2):11-8.
6. Desai A, Chandler N. Calcium hydroxide-based root canal sealer: review. J Endod. 2009 Apr;35(4):475-80.
7. Duarte MAH, Ordinola-Zapata R, Bernardes RA, Bramante CM, Bernardineli N, Garcia RB et al. Influence of calcium hydroxide association on the physical properties of AH Plus. J Endod. 2010 Jun;36(6):1048-50.
8. Gorduysun M, Avcu N. Evaluation of radiopacity of different root canal sealers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108:135-40.
9. Grossman LI. An improved root canal cement. J Am Dent Assoc. 1958 Mar;56(3):381-5.
10. Leonardi DP, Batisti JC, Klimiont DT, Tomazinho PH, Baratto-Filho F, Haragushiku GA et al. Avaliação in vitro da ação antimicrobiana de alguns cimentos endodônticos. RSBO. 2009;6(4):368-73.
11. McComb D, Smith DC. Comparison of physical properties of polycarboxilate-based and conventional root canal sealer. J Endod. 1976 Aug;2(8):228-35.
12. Mente J, Hage N, Peffferle T, Koch MJ, Geletneke B, Dreuhaupt J et al. Treatment outcome of mineral trioxide aggregate: repair of root perforation. J Endod. 2010 Feb;36(2):208-13.
13. Moraes SH, Zytkievitz E, Ribeiro JC, Heck AR, Aragão EM. Cimentos endodônticos: tempo de presa e escoamento de dois cimentos obturadores de canais radiculares. RGO. 1989 Nov-Dec;37(6):455-9.
14. Negm MM, Lilley JD. A study of the viscosity and working time of resin-based root canal sealers. J Endod. 1985 Oct;11(10):442-5.
15. Oliveira RL, Oliveira-Filho RS, Gomes HC, Franco MF, Enokihara MMSS, Duarte MAH. Influence of calcium hydroxide in addition on its biocompatibility. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Jan;109(1):e50-4.
16. Orstavik D. Material used for root canal obturation: technical, biological and clinical testing. Endodontic Topics. 2005;12:25-8.
17. Petry AEA, Salles AA, Kilian L, Vidor MM, Figueiredo JAP. Evaluation of endodontic sealer radiopacity using digitized imaging equipment. Braz Dent J. 1997;2(1):24-8.
18. Reiss-Araújo C, Araújo SS, Baratto-Filho F, Reiss LC, Fidel SR. Comparação da infiltração apical entre os cimentos obturadores AH Plus, Sealapex, Seales 26 e Endofill por meio de diafanização. RSBO. 2009;6(1):21-8.
19. Resende LM, Rached-Junior FJA, Versiani MA, Souza-Gabriel AE, Miranda CES, Silva-Souza YTC et al. A comparative study of physicochemical properties of AH Plus, Epiphany and Epiphany SE root canal sealers. International Endod Journal. 2009;42:785-93.
20. Salazar Silva JR, Antoniazzi JH, Lage Marques JL. Propriedades físicas dos cimentos endodônticos Endobalsam e N-Rickert. Rev Odontol Univ São Paulo. 1996;10(2):121-8.
21. Savioli RN, Silva RG, Vansare LP. Determinação da relação pó/líquido e do tempo de endurecimento de alguns cimentos endodônticos que contêm óxido de zinco/eugenol. Odontol Uni São Francisco. 1999;17:57-62.
22. Scelza MFZ, Costa RF, Oliveira AR. Avaliação comparativa da radiopacidade de cinco cimentos endodônticos. RPG Rev Pós-Grad. 2001;8(2):125-8.
23. Silva RG, Savioli RN, Cruz Filho AM, Pécora JD. Estudo da estabilidade dimensional, solubilidade e desintegração e radiopacidade de alguns cimentos obturadores dos canais radiculares do tipo Grossman. Rev ABO Nac. 1994 Feb-Mar;2(1):40-3.
24. Shah PMM, Chong BS, Sidhu SK, Ford TRP. Radiopacity of root-end filling materials. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81:476-9.
25. Sydney GB, Ferreira M, Deonizio MDA, Leonardi DP, Batista A. Análise do perfil de escoamento de seis cimentos endodônticos. RGO. 2009 Jan-Mar;57(1):7-11.
26. Tadesmir T, Yesilyurt C, Yildirim T, Er K. Evaluation of the radiopacity of new root canal paste/sealers by digital radiography. J Endod. 2008 Nov;34(11):1388-90.
27. Tagger M, Katz A. Radiopacity of endodontic sealers: development of a new method for direct measurement. J Endod. 2003 Nov;29(11):751-5.
28. Tanomaru-Filho M, Silva RSF, Tanomaru JMG, Leonardo MR, Silva LAB. Avaliação do selamento apical de obturações de canais radiculares com diferentes cimentos endodônticos. J Bras Endod. 2004;5(17):146-9.
29. Tanomaru JMG, Duarte MH, Gonçalves M, Tanomaru-Filho M. Radiopacity evaluation of root canal sealer containing calcium hydroxide and MTA. Braz Oral Res. 2009;23(2):119-23.
30. Tanomaru-Filho M, Jorge EG, Tanomaru JMG, Gonçalves M. Radiopacity evaluation of new root canal filling materials by digitalization of images. J Endod. 2007 Mar;35(3):249-51.
31. Yilmaz HZ, Kalender A, Cengiz E. Use of mineral trioxide aggregate in treatment of invasive cervical resorption: a case report. J Endod. 2010 Jan;36(1):160-3.
 Correspondence:
Correspondence:
Ana Paula Meirelles Vidotto
Avenida Santa Isabel, n.º 241
CEP 13084-755 – Campinas – SP – Brasil
E-mail: ana_vidotto@hotmail.com
Received for publication: February 4, 2011
Accepted for publication: March 30, 2011
