










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.8 no.4 Joinville Out./Dez. 2011
ORIGINAL RESEARCH ARTICLE
Prevalence of dental trauma among children treated in the Pediatric Dentistry Clinic of the State University of Amazonas
Andrea Melo Moutinho da CostaI; Savana MaiaI; Gabriel Lucas de Cardoso da CruzI; Regina Maria Puppin RontaniII
I State University of Amazonas – Manaus – AM – Brazil
II State University of Campinas, Pediatric Dentistry Department – Campinas – SP – Brazil
ABSTRACT
Introduction: Dental trauma is an acute energy transmission to the tooth and to the supporting structures that may result in fracture, tooth dislocation, breaking or crushing of supporting tissues. Objective: This retrospective study aimed to evaluate dental trauma prevalence among children treated in the Pediatric Dentistry Clinic of the State University of Amazonas (short UEA) from July 2005 to June 2009. Material and methods: The sample used in the analysis consisted of 171 children treated in the Pediatric Dentistry Clinic of the State University of Amazonas (short UEA), Manaus – Amazonas – Brazil. Results: Dental trauma prevalence among these children was 29.8%. No statistically significant association was found regarding to gender. Conclusion: The prevalence of dental trauma among children treated in the Pediatric Dentistry Clinic of the State University of Amazonas was in average 29.8%, which is agreement with other studies.
Keywords: epidemiology; dental trauma; tooth fractures.
Introduction
Dental trauma is described in literature as a lesion of variable extension, intensity, and severity caused by forces acting on tooth due to accidents and/or beatings 3,15.
Oral/tooth trauma is a serious health problem which can result in pain, loss of function and aesthetics, and psychological problems, both for children and their parents. Traumatic injuries affect mainly children, with its incidence peak at 2 to 4 years and at 8 to 10 years of age, with greater prevalence for males than females 3.
Concerning to its aethiology in primary dentition, dental traumas occur mainly due to falls against hard objects when the child begins to walk by her/himself, between 18 and 30 months. The child home is the place where dental trauma frequently takes place, regardless of gender. In permanent dentition, this traumatic injury occurs due to fights and full contact physical activities 5,6.
Some predisposing anatomical factors increase the susceptibility to dental injuries, among which is Angle Class II malocclusion, increased overjet (greater than 4 mm), open bite, short or hypotonic upper lip and oral breathing patients 15. A study 12 observed that in patients presenting overjet greater than 4 mm, trauma frequency ranged from 19.4% to 29.4%; in additional to this aethiology is tooth structure impairment of adult patients due to large number and extension of restorations. Other factors predisposing to dental trauma are carious lesions, endodontically treated teeth, and accidents/fights in sports activities 12,19.
Epidemiology and predictability of traumatic lesions in sports activities, as well as the emergency treatment of these lesions in athletes also constitutes another type of increased investigation 3,5. Concerning to the degree of complication, the damage extension varies from a small fracture line to more complex situations (e .g. vertical fractures) which result in tooth loss or even the complete tooth avulsion from its socket. It has been reported that approximately 2 million teeth are avulsionated at every year, many of them because of sports activities, estimating that an occurrence of one avulsionated teeth per each 200 school children 19. Additionally to sports activities, games, falls, and strokes are also common causes of tooth trauma frequently occurring at schools 3,19.
Dental trauma involves a variety of factors and their knowledge is mandatory for promoting an effective prevention. The dentist should be aware of the factors related to trauma (e.g. the age most frequently affected, how and where the trauma occurred, the most common type of injuries, and the most affect teeth) both to adopt an adequate therapeutic management in cases of emergency treatment and to guide the child's parents about the measures to be taken at the trauma moment, mainly in cases of tooth avulsion 23.
The immediate searching for specialized treatment is fundamental to obtain an early diagnosis, as well as the elaboration of a proper treatment planning and a good prognosis. However, it is observed that when trauma is not associated to pain, bleeding, displacement, or tooth loss there is some delay in seeking for specialized treatment, which may lead to the appearance of posterior complications as pulp necrosis, root canal obliteration, root resorption, bone loss, and even tooth loss. Consequently, prevalence studies on trauma cases favor the direction of the researches, the design of educative campaigns, and the adequate therapeutic management, in order to orient the prevention and management of these emergency situations 23.
This study aimed to perform an epidemiological study on tooth traumas and to evaluate trauma prevalence and incidence among children treated in the Pediatric Dentistry Clinic of the State University of Amazonas, from July 2005 to June 2009.
Material and methods
Material
One hundred and seventy-one dental charts of the discipline of Pediatric Dentistry of the State University of Amazonas were analyzed from July 2005 to June of 2009. Inclusion criteria comprised the patients treated in the aforementioned period and whose dental charts were properly filled in. Exclusion criteria included patients treated in different time periods and dental charts incorrectly filled in.
Method
After the approval of the Ethical Committee in Research of the State University of Amazonas (protocol No. 107/09), data collection was initiated according to inclusion criteria. Dental charts had information on gender, age, where and how the trauma had occurred, the tooth involved, and the time elapsed between trauma incidence and the searching for treatment. Dental charts were filled in by undergraduate students, under guidance of the Professors of the discipline of Pediatric Dentistry. World Health Organization classification modified by Andreasen and Andreasen 4 was used to determine the types of oral/tooth trauma: enamel fracture; enamel/dentin fracture without pulp involvement; enamel/dentin fracture with pulp involvement; root fracture; crown-root fracture with or without pulp involvement; concussion/subluxation; intrusive luxation; extrusive luxation; lateral luxation; and avulsion.
Statistical analysis
Data were presented in graphs and tables, in which simple absolute and relative frequencies were calculated. In trauma prevalence analysis, we still calculated the confidence intervals at 95% level (CI95%). Gender association in relation to trauma prevalence was analyzed by chi-square test and Pearson's correlation. We used Epi-Info version 3.5.1 software for Windows, which is developed and freely distributed (www.cdc.org/epiinfo); level of significance was set at 5%.
Results
We analyzed 171 dental charts filed in the discipline of Pediatric Dentistry of the State University of Amazonas, in which was verified that only 29.8% of the patients showed some type of tooth trauma and 70.2% did not present any type of tooth trauma.
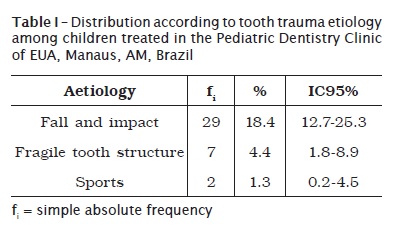
Table I exhibits that fall and impact was the most frequent cause of trauma (18.4%), followed by caries (4.4%), and sports accidents (1.3%).
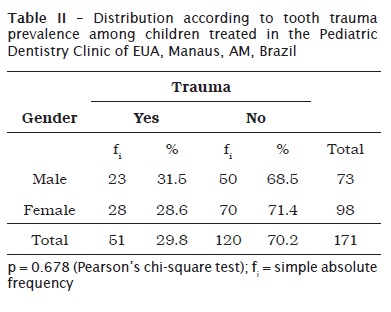
The distribution according to gender was 42.7% of males and 57.3% of females. No statistically significant association was found for tooth trauma in relation to gender (p = 0.678) of the studied children, at the level of significance of 5% (table II).
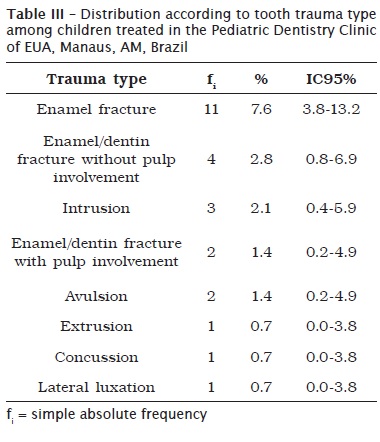
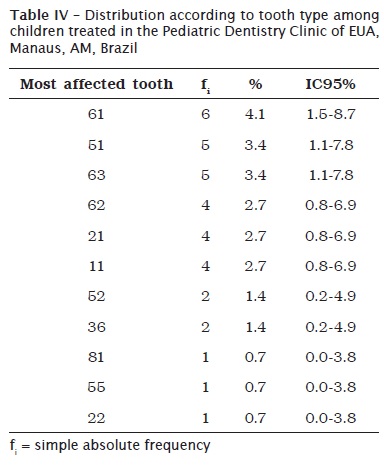
Tables III and IV shows the distribution according to trauma type and the most affected tooth among the studied children. It can be seen in table III that enamel fracture was the most common trauma type, followed by enamel/dentin fracture without pulp involvement, intrusion, avulsion, enamel/dentin fracture with pulp involvement, concussion, luxation, and extrusion. In table IV, we observed that upper anterior teeth were the most affected teeth; left primary central incisor (#61) was the most affected, followed by tooth #51, #63, #62, #21, #11, #52 and #36. The least affected teeth were tooth #81, #55, and #22.
Discussion
In this present study conducted in the Pediatric Dentistry Clinic of the State University of Amazonas we verified that tooth trauma prevalence was 29.8%. Such result corroborates the study of Navabazam and Farahani (2010) 17 evaluating tooth trauma prevalence and factors related to it in children with age between 9 and 14 years, whose results showed a prevalence of 27.5%. Notwithstanding, some studies presented higher 13,23 or lower 16 frequencies of tooth trauma prevalence.
According to this present study, fall and impact was the most frequent causes of trauma (18.4%), followed by fragile tooth structure (4.4%) and sports (1.3%) (table I); such results are in agreement with other studies 2,13,23. Sousa et al. (2008) 23 evaluated tooth trauma among children treated in the discipline of Pediatric Dentistry of Federal University of Ceara and verified that the most common cause of trauma was falls (63.5%). In the study of Granville-Garcia et al. (2006) 13 was found a prevalence of 92%, and the study of Altun et al. (2009) 2 found a prevalence of 40.3% of this trauma type.
Concerning to trauma incidence in relation to gender, 42.7% were males and 57.3% females. There was no statistically significant association, which is in agreement with most of the studies reporting no statistically significant differences between genders regarding to traumatic lesions in primary tooth 4,5,17,21. However, other studies pointed out different results, such as that conducted by Llarena del Rosario et al. (1992) 14, which showed that 61.8% of the children exhibiting tooth trauma were males.
Among tooth trauma types, the most frequent lesion was enamel fracture (7.6%) (table III), followed by enamel/dentin fracture without pulp involvement (2.8%), intrusion (2.1%), enamel/dentin fracture with pulp involvement (1.4%), avulsion (1.4%), extrusion (0.7%), concussion (0.7%), and lateral luxation (0.7%). This result is in agreement with most of the studies, such as the study of Altun et al. (2009) 2, which used a very expressive sample of 4,956 children (2,553 boys and 2,403 girls) aging from 6 to 12 years. The authors employed World Health Organization classification modified by Andreasen and Andreasen 4, and found that the most common lesion was enamel fracture (44.6%), followed by enamel/dentin fracture without pulp involvement (19%) 2. On the other hand, Tolentino et al. (2008) 25 found an avulsion prevalence of 33.3%, followed by lateral luxation (17%), crown fracture (15.5%), with or without pulp exposure, and lateral extrusion (12.4%).
In our study, the most affected tooth was upper central incisors (#61 and #51, 4.1% and 3.4%, respectively), followed by tooth #63 (3.4%), #62, #21, #11 (2.7% each), #52, #36 (1.4% each), #22, #55, #81 (0.7% each) (table IV). These results are in agreement with all studies, including the research of Granville-Garcia et al. (2006) 13, who conducted a transversal, analytic study with retrospective components through parents' questionnaire. The authors examined 2,651 children of public and private institutions (daycare centers and preschools), from 1 to 5 years of age, during the second semester of 2002, in Recife, Pernambuco, Brazil. The authors found that the most affected tooth was #61 (52.4%), followed by #51 (44.9%), which corroborate the results found by this present study as well as other researches1,3,5,7,8,10,11,16,18,20,22,24,26.
Upper central incisors are the teeth most affected by trauma due to their vulnerable position at tooth arch and because these teeth are generally protruded due to an inappropriate lip sealing 9. Upper central incisors are normally more protruded than lower central incisors and tend to be the first teeth receiving a direct impact 17.
Conclusion
According to the obtained data, it can be concluded that:
• trauma prevalence among children treated in Pediatric Dentistry Clinic of EUA was 29.8%, which was moderate according to literature;
• fall and impact was the most frequent trauma causes (18.4%);
• no statistically significant association was found in tooth trauma prevalence regarding to gender (p = 0.678);
• the most common type of tooth trauma was enamel fracture (7.6%);
• upper central incisors were the teeth most affected by trauma.
Acknowledgments
The authors thank to the Foundation of Support to Research of the State of Amazonas (short Fapeam) for scholarship grant.
References
1. Alencar CRB, Cavalcanti AL, Bezerra PKM. Perda precoce de dentes decíduos: etiologia, epidemiologia e conseqüências ortodônticas. Publ UEPG Ci Biol Saúde. 2007 Mar-Jun;13(1/2):29-37. [ Links ]
2. Altun C, Ozen B, Esenlik E, Guven G, Gürbüz T, Acikel C et al. Traumatic injuries to permanent teeth in Turkish children, Ankara. Dent Traumatol. 2009 Jun;25(3):309-13.
3. Andreasen JO, Andreasen FM, Bakland LK, Flores MT. Manual de traumatismo dental. Porto Alegre: Artmed; 2000.
4. Andreasen JO, Andreasen FM. Texto e atlas colorido de traumatismo dental. 3. ed. Porto Alegre: Artmed; 2001. p. 151-80.
5. Andreasen JO. Etiology and pathogenesis of dental injuries. A clinical study of 1298 cases. Scand J Dent Res. 1970;78(4):329-42.
6. Barbarato PR, Peres MA. Perdas dentárias em adolescentes brasileiros e fatores associados: estudo de base populacional. Rev Saúde Pública. 2009;43(1):13-25.
7. Bastone EB, Freer TJ, Mcnamara JR. Epidemiology of dental trauma: a review of the literature. Aust Dent J. 2000 Mar;45(1):2-9.
8. Cardoso M, Carvalho Rocha MJ. Traumatized primary teeth in children assisted at the Federal University of Santa Catarina, Brazil. Dent Traumatol. 2002 Jun;18(3):129-33.
9. Corrêa MSNP. Odontopediatria na primeira infância. 1. ed. São Paulo: Santos; 2005. p. 848.
10. Cortes MI, Marcenes W, Sheimam A. Prevalence and correlates of traumatic injuries to the permanent teeth of schoolchildren aged 9-14 years in Belo Horizonte, Brazil. Dent Traumatol. 2001 Feb;17(1):22-6.
11. Flores MT. Traumatic injuries in the primary dentition. Dent Traumatol. 2002 Dec;18(6):287-98.
12. Forsberg CM, Tedestam G. Etiological and predisposing factors related to traumatic injuries to permanent teeth. Swed Dent J. 1993;7(6):183-90.
13. Granville-Garcia AF, Menezes VA, Lira PIC. Prevalência e fatores sociodemográficos associados ao traumatismo dentário em pré-escolares. Odontologia Clín-Científ. 2006 Jan-Mar;5(1):57-64.
14. Llarena del Rosario ME, Acosta Alfaro VM, Garcia-Godoy F. Traumatic injuries to primary teeth in Mexico city children. Endod Dent Traumatol. 1992 Oct;8(5):213-4.
15. Losso EM, Tavares MCR, Bertoli FMP, Baratto-Filho F. Traumatismo dentoalveolar na dentição decídua. RSBO. 2011 Jan-Mar;8(1):e1-20.
16. Moura LFAD, Ferreira DLA, Melo CP, Sady MCLM, Moura MS, Mendes RF et al. Prevalência de injúrias traumáticas em crianças assistidas na Clínica Odontológica Infantil da Universidade Federal do Piauí, Brasil. Pesq Bras Odontoped Clín Integr. 2008 Sep-Dec;8(3):341-5.
17. Navabazam A, Farahani SS. Prevalence of traumatic injuries to maxillary permanent teeth in 9- to 14-year-old school children in Yazd, Iran. Dent Traumatol. 2010 Apr;26(2):154-7.
18. Nogueira AJS. Perdas precoces de dentes decíduos e suas conseqüências para dentição futura – elaboração de propostas preventivas. Rev ABO Nac. 1998;6(4):228-33.
19. Padilla R, Balikov S. Sports dentistry: coming of age in the ‘90s. J Calif Dent Assoc. 1993 Apr;21(4):27-37.
20. Sandalli N, Cildir S, Guler N. Clinical investigation of traumatic injuries in Yeditepe University, Turkey during the last 3 years. Dent Traumatol. 2005 Aug;21(4):188-94.
21. Şaroğlu I, Sönmez H. The prevalence of traumatic injuries treated in the pedodontic clinic of Ankara University, Turkey, during 18 months. Dent Traumatol. 2002 Dec;18(6):299-303.
22. Simões FG, Leonardi DP, Baratto-Filho F, Ferreira EL, Fariniuk LF, Sayão SMA. Fatores etiológicos relacionados ao traumatismo alvéolo-dentário de pacientes atendidos no pronto-socorro odontológico do Hospital Universitário Cajuru. RSBO. 2004;1(1):50-5.
23. Sousa DL, Moreira Neto JJS, Gondim JO, Bezerra Filho JG. Prevalência de trauma dental em crianças atendidas na Universidade Federal do Ceará. Rev Odonto Ciênc. 2008 Oct-Dec;23(4):355-9.
24. Souza Filho FJ, Soares AJ, Gomes BPFA, Zaia AA, Ferraz CCR, Almeida JFA. Avaliação das injúrias dentárias observadas no Centro de Trauma Dental da Faculdade de Odontologia de Piracicaba – Unicamp. RFO UPF. 2009 May-Aug;14(2):111-6.
25. Tolentino LS, Camarini ET, Tolentino ES, Iwaki Filho L, Endo MS, Pavan AJ. Traumatismo dentoalveolar: análise dos casos atendidos no serviço de residência em cirurgia e traumatologia bucomaxilofacial da Universidade Estadual de Maringá no período de 2004 a 2006. Rev Odontol Unesp. 2008;37(1):53-7.
26. Wilson CF. Management of trauma to primary and developing teeth. Dent Clin North Am. 1995 Jan;39(1):133-67.
 Correspondence:
Correspondence:
Andrea Melo Moutinho da Costa
Universidade do Estado do Amazonas – Odontologia
Rua Carvalho Leal, 1.777 – Cachoeirinha
CEP 69050-520 – Manaus – AM – Brasil
E-mail: andrea_moutinho@hotmail.com
Received for publication: April 4, 2011
Accepted for publication: June 1st, 2011
