










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.1 Joinville Jan./Mar. 2012
ORIGINAL RESEARCH ARTICLE
Evaluation of chlorhexidine effects on periodontium healing after gingivoplasty surgery
Carlos Augusto Nassar I ; Ana Paula Bitencourt II ; Patricia Oehlmeyer Nassar I
I School of Dentistry, Center of Biological and Health Sciences, State University of West of Paraná, campus of Cascavel – Cascavel – PR – Brazil
II DDS – Cascavel – PR – Brazil
ABSTRACT
Introduction and objective: The aim of this study was to evaluate, in vivo, the effect of 0.12% chlorhexidine on the healing of gingival tissues undergoing gingivoplasty. Material and methods: The clinical assessment was checked by plaque and gingival indexes and by periodontal probing depth. After the basic procedures of periodontal therapy, 12 patients underwent gingivoplasty technique. All patients used chlorhexidine mouthrinsing for 7 or 14 days postoperatively. Results: Postoperative indexes measured at 14 and 30 days after surgery showed significant improvements in all parameters. Conclusion: The use of chlorhexidine resulted in statistically significant responses, reducing the plaque and gingival indexes of tissues undergoing gingivoplasty surgery. There is no need of extending chlorhexidine for more than 7 days.
Keywords: chlorhexidine; gingivoplasty; periodontal disease.
Introduction
Currently, the search for dental treatment has increased due to aesthetical reasons. This fact may be related to a greater information demand through either magazines or television shows, which have incentivized the search for beauty treatments and also due to the personal impact in social life. Consequently, several patients have increasingly been concerned in harmonizing their tooth-gingiva relationship, seeking for techniques that solve their necessities of a beautiful smile 16.
Periodontics may help to promote a more aesthetical smile, altering the tooth/periodontium relationship through gingivectomy as well as by recovering the physiologic gingival morphology through gingivoplasty. Gingivoplasty is a procedure similar to gingivectomy but with a different goal. While gingivectomy is executed to eliminate periodontal pockets including gingival recontouring as part of the technique, gingivoplasty is the gingival recontouring to create physiologic gingival architecture only, in the absence of periodontal pockets 15.
In post-surgical situations is extremely difficult to maintain an adequate plaque control, because of the healing tissues' sensibility and fragility 12. Therefore, the use of antimicrobial agents as adjuvants or substitutes to mechanical control is necessary 17 to prevent microorganisms' recolonization on tooth surface. Among mouthwashes, chlorhexidine is one of the most powerful and carefully studied agents, highly effective, and generally used as gold standard for other mouthwash tests 6,21. Chlorhexidine is presented in the form of several salts, such as: gluconate, digluconate, acetate, and hydrochloride; digluconate is the most indicated one because it exhibits greater solubility in water and at a physiologic pH is dissociated, releasing the cationic component 17. Chlorhexidine, which chemically is a biguanide, has a greater antiplaque effect than other microbial agents because of its great capacity of adsorption to tooth and mucosa's surfaces 11.
Studies have demonstrated that chlorhexidine rinses can destroy about 80 to 90% of the salivary bacteria 12,17. This is because the great chlorhexidine affinity to gram-positive and gram-negative bacteria, probably due to chlorhexidine's cationic molecule (positive) to the bacteria's anionic cellular wall (negative). This adsorption provokes an osmotic imbalance between the bacterial cytoplasm and the external medium, causing an increase of the bacterial membrane permeability. Consequently, this enables the leaking or denaturation by chlorhexidine penetration, leading to bacterial lysis. When used at high concentrations, chlorhexidine is bactericide, however, at low concentration, is bacteriostatic. At 0.2% and 0.12% concentrations, it presents the same bactericidal action on the sensitive microorganisms 17.
Although dental market exhibits chlorhexidine mouthwashes at 2% concentration, the use of 0.12% concentration products are the most indicated, because, at this concentration the side-effects of the most concentrated solutions are decreased, therefore, maintaining the efficacy against the microorganisms 13. Consequently, 0.12% concentration of 15 ml mouthrinses has been largely employed 18,20 for 1 minute.
The aim of this study was to evaluate the influence of daily 0.12% chlorhexidine mouthrinses, at short periods, on both plaque control and periodontal healing during following-up appointments of patients who had been submitted to gingivoplasty technique.
Material and methods
This study's participants were selected from those who sought the University's Dentistry Clinic of the Discipline of Periodontics (n = 30). Twelve patients were selected, aging from 18 to 50 years-old (eight men and four women). Inclusion criteria comprised non contributory systemic disease; at least 12 sites with probing depth above 5 mm (in the anterior teeth), with bleeding to probing and gingival inflammation at clinical examination, without loss of attachment level, but with necessity of gingivoplasty surgeries previously determined and clinically diagnosed. Exclusion criteria comprised negative history of antimicrobial and anti-inflammatory (steroids or non steroids) use in the last six and three months prior to the study, respectively; no pregnancy; negative history of contraceptive use, or any other hormone; negative history of tobacco use or definitive interruption of its use for at least 5 years; negative history of periodontal treatment in the last 12 months. This study was approved by the Ethical Committee in Research, under protocol number #534/2008. All participants sign a free and clarified consent form and received its copy. The teeth were normally positioned within upper and lower arches and their clinical examination was executed at labial, lingual/palatal, mesial and distal surfaces. Patients should presented at least all anterior teeth and bicuspids, both in upper and lower arches because all surgeries would be performed in anterior teeth, regardless of tooth arch.
Initial clinical examination was carried out by one single examiner previously trained, by using a Williams periodontal probe (#23), determining:
1. Silness & Löe plaque index 19;
2. Silness & Löe gingival index 10;
3. Probing depth: distance from the gingival sulcus bottom to the gingival margin at six points: mesial-labial, labial, distal-labial, distal-lingual/palatal, lingual/palatal, and mesial/lingual-palatal of each tooth to be examined.
After initial clinical examination and laboratorial assessment, patients were randomly divided into two groups (n = 6), according to table I.

Therefore, each group received basic periodontal treatment and instructions for proper plaque mechanical control. Chlorhexidine mouthrinse (Periogard® – Colgate-Palmolive Indústria e Comércio Ltd. – São Bernardo do Campo, SP, Brazil) was used for all patients just after the surgery, for one minute, twice a day, 30 minutes after toothbrushing, during the study's periods (seven or 14 days). All patients received surgical cement on the surgery site immediately after the procedure as well as the prescription of painkillers for three days aiming patient's post-operative comfort.
Patients were evaluated for a total period of 30 days. Post-operative clinical examinations of the plaque and gingival indexes were executed at 0, 14, and 30 days; post-operative clinical examination probing depth was performed at 0 and 30 days 15. At all following-up periods, the patients were again instructed regarding to oral hygiene.
Data were analyzed and evaluated by ANOVA and Tukey tests (p < 0.01) after they had been rigorously analyzed and within the normality curve.
Results
Figures 1, 2, 3, and 4 show the initial and clinical healing images of patients treated by gingivoplasty surgery and chlorhexidine use (7 or 14 days).




Table II shows the percentage means of the plaque index at the evaluation periods in all groups, according to table I. Initially, the groups showed differences regarding to the index of visible plaque. At the second week, a significantly reduction of the visible plaque index was seen in both groups; group 2 presented the highest reduction mean, just after the surgical cement removal.
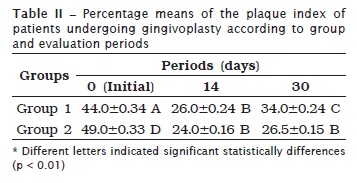
Table III shows the percentage mean of the gingival index at the evaluated periods for both groups. At day 0, both groups presented different values of gingival bleeding. During the following gingival index evaluations, the percentage means showed an equivalent decreasing at all this study's periods, as seen in table III. Both groups demonstrated a statistically significant reduction in gingival bleeding. This tendency was confirmed at the intermediary post-operative period and better demonstrated in group 2, probably because group 2 patient's mechanical plaque control had begun prior to group 1.
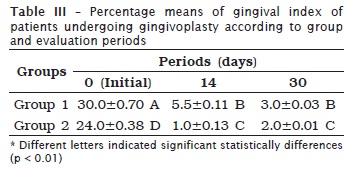
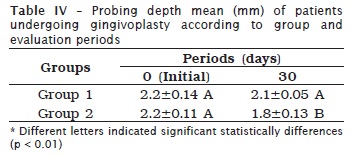
Table IV shows probing depth means (mm) at all the evaluated periods of both groups. At the first evaluation (prior to gingivoplasty), both groups were statistically matched regarding to probing depth mean. At treatment ending, there was a statistically significant reduction in probing depth in group 2, demonstrating the surgery's proper indication, despite of the fact that the value be of little significance when clinically analysed.
Discussion
Aesthetical demanding in dental practice is a reality that is not limited by restorative treatments. The establishment of a physiologic gingival pattern, characterized by a beveled and properly sculpted margin, is essential for periodontal health maintenance and contributes for oral health improvement. This gingival pattern can be obtained through gingivectomy and gingivoplasty surgeries 1.
When surgery due to aesthetical correction of low or asymmetric smiles is needed, good planning is fundamental aiming to alter the aesthetical components to reach success, both for the clinician and patient. For this purpose, it is important to observe the technique's proper indication and post-operative period, to reach the aesthetical success faster. Therefore, this study was conducted to search the careful use of chlorhexidine.
The initial response after gingivectomy/gingivoplasty is the formation of a protector surface clot; the underlying tissue becomes acutely inflamed, with some necrosis. The clot is then replaced by a connective tissue. After up to 24 hours, there is an increase of new connective tissue cells, just beneath the surface layer of inflammation and necrosis. The connective tissue grows towards coronal surface, creating a new free gingival margin and sulcus. The epithelial activity at the margins reaches its peak at 24 to 36 hours. The new epithelial cells come from the basal and spinous layers of the epithelium from the wound margin, migrating towards the wound on a fibrin layer that, later, is reabsorbed and replaced by a layer of connective tissue. Epithelial cells advance in a disorganized movement, with the cells being fixed to the substrate by hemidesmosomes and a new basal lamina. After five to 14 days, the epithelization of the surface is completed. The vasodilatation and vascularity begin to decrease after the fourth day of healing and seem to be almost normal up to the sixteenth day. Complete healing of conjunctive tissue takes about seven weeks 2. Several studies agree that adjunctive dental biofilm chemical controlling, in several situations, is mandatory and is one of the main indications during periodontal post-surgery period 2,4,8,14.
Chlorhexidine exhibits a substantivity of about 12 hours and exerts an initial bactericide action immediately after mouthrinsing, combined with a longer bacteriostatic action 17. In each 10 ml mouthrinse, 30% of chlorhexidine is retained in oral cavity and is slowly released to promote a longer bactericide effect for a period of 24 hours 11. It is this retention capacity (substantivity or residual effect) that gives to chlorhexidine a great advantage against the other existing antimicrobials, instead of its other characteristic related to the bactericide activity 9,12. For such reason, chlorhexidine was used in this study.
Despite of these beneficial effects, chlorhexidine use in oral mouthrinsing has showed several local side-effects. These effects are: brownish stains in teeth, some restorative materials and the tongue's back; taste perturbation in which the salt flavor seems to be preferentially affected and the foods and beverages' taste becomes softener; oral mucosa erosion and bilateral or unilateral tumefaction of parotid, which is a extremely rare and unexplained occurrence; stimulus of supragingival formation of calculus in longer usages 5,7,9, although other authors did not observed this same adverse effect in shorter observation periods 3,22. Therefore, these side effects may compromise patients' aesthetic and physical, mental and social well-being after chlorhexidine use. Consequently, the smallest time period of chlorhexidine use can facilitate its efficacy and decrease its undesirable effects; this is corroborated by this study through the analysed periodontal parameters, as demonstrated in tables II and III.
Another disadvantage of chlorhexidine is that it can be deactivated by normally ingredients within tooth paste's formulations, such as sodium lauryl sulphate and sodium monofluorophosphate. Accordingly, it is recommended that chlorhexidine-based mouthrinses be executed 30 minutes after toothbrushing or that dentifrices with these ingredients should not be used 9,15.
The improvement in periodontal parameters demonstrated in this study, with greater emphasis on probing depth reduction (table IV), probably because of a shorter chlorhexidine use period and its onset prior to a more rigorous plaque mechanical control, once the intermediary period in both groups demonstrated a significant tendency towards the plaque and gingival index reduction. This significant tendency was sustained at the final period for both groups.
Conclusion
Literature is extensive and impressive with regard to chlorhexidine action on bacterial plaque control. Considering this study's results and methodology, it can e concluded that chlorhexidine use through daily mouthrinses resulted in statistically significant responses, because it reduced the plaque and gingival indexes of tissues submitted to gingivoplasty. Its use does not demand more than seven days.
References
1. Almeida ALPF, Greghi SLA, Resende DRB. Gingivoplasty: remodeling the gingival tissue to improve oral esthetics. J Bras Clín Estét Odontol. 1999;3(16):75-80. [ Links ]
2. Brauner MT. Controle químico da placa. Estudo comparativo entre a clorexidina e a alexidina. Revista APCD. 1982;36(6):594-604.
3. Cancro LP, Paulovich DB, Klein K, Picozzi A. Effects of a chlorhexidine gluconate mouthrinse on dental plaque and calculus. J Periodontol. 1972;43(11):687-91.
4. Chibinski ACR, Grando K, Fanchin PT, Campagnoli E, Santos FA, Wambier DS. Descontaminação de escovas dentais utilizadas por crianças portadoras de necessidades especiais: análise microbiológica. RSBO. 2011 Jun;8(2):145-52.
5. Ciancio SG. Chemical agents: plaque control, calculus reduction and treatment of dentinal hypersensitivity. Periodontol 2000. 1995;8:75-86.
6. Gjermo P, Baastad KL, Rölla G. The plaque inhibiting capacity of antibacterial compounds. J Periodontal Res. 1970;5(2):102-9.
7. Grossman E, Meckel AH, Isaacs RL, Ferretti GA, Sturzenberger OP, Bollmer BW et al. A clinical comparison of antibacterial mouthrinses: effects of chlorhexidine, phenolics, and sanguinarine on dental plaque and gingivitis. J Periodontol. 1989;60(8):435-40.
8. Gunsolley JC. A meta-analysis of six-month studies of antiplaque and antigingivitis agents. J Am Dent Assoc. 2006;137(12):1649-57.
9. Lindhe J, Karring T, Lang NP. Tratado de periodontia clínica e implantologia oral. 4. ed. Rio de Janeiro: Guanabara Koogan; 2005. p. 450-77.
10. Löe H, Silness J. Periodontal disease in pregnancy. I – Prevalence and severity. Acta Odontol Scand. 1963;21:533-51.
11. Löe H, Schiott CR. The effect of mouthrinses and topical application of chlorhexidine on the development of dental plaque and gingivitis in man. J Periodontal Res. 1970;5(2):79-83.
12. Lopes JCA, Duarte, CA, DeMicheli G. O uso da clorexidina no pós-operatório periodontal: revisão de literatura. RPG. 1997;4(1):28-33.
13. Mendes MMSG, Zenóbio EG, Pereira OL. Agentes químicos para o controle da placa bacteriana. Fortaleza: Periodontia. 1995;5(2):253-6.
14. Navarro MFL, Côrtes DF. Avaliação e tratamento do paciente com relação ao risco de cárie. Maxi-Odonto:Dentística. 1995;1(1):1-38.
15. Newman MG, Takei HH, Klokkevold PR, Carranza FA. Periodontia clínica. 10. ed. Rio de Janeiro: Elsevier; 2007. p. 909-17.
16. Rosetti EP, Sampaio LM, Zuza EP. Correção de assimetria dentogengival com finalidade estética: relato de caso. RGO. 2006;54(4):384-7.
17. Rösing CK, Zanatta FB. Clorexidina: mecanismo de ação e evidênicas atuais de sua eficácia no contexto do biofolme supragengival. Scientific-A. 2007;1(2):35-43.
18. Segreto VA, Collins EM, Beiswanger BB, De La Rosa M, Isaacs RL, Lang NP et al. A comparison of mouthrinses containing two concentrations of chlorhexidine. J Periodontol Res. 1986;21(16):23-32.
19. Silness J, Löe H. II – Correlation between oral hygiene and periodontal condition. Acta Odontol Scand. 1964;22:121-35.
20. Smith RG, Moran J, Addy M, Doherty F, Newcombe RG. Comparative staining in vitro and plaque inhibitory properties in vivo of 0.12% and 0.2% chlorhexidine mouthrinses. J Clin Periodontol. 1995;22(8):613-7.
21. Torres CRG, Kubo CH, Anido AA, Rodrigues JR. Agentes antimicrobianos e seu potencial de uso na Odontologia. Pós-Grad Rev Fac Odontol São José dos Campos. 2000;3(2):43-52.
22. Zucco DL, Rossi B, Lopes CMC, França PHC, Schubert EW. Efeito da clorexidina em gel ou dentifrício nos níveis salivares de estreptococos do grupo mutans em crianças do Distrito do Saí (São Francisco do Sul, SC, Brasil). RSBO. 2010 Mar;7(1):27-34.
 Correspondence:
Correspondence:
Carlos Augusto Nassar
Rua Pernambuco, n.º 593, apto. 504 – Centro
CEP 85810-020 – Cascavel – PR – Brasil
E-mail: canassar@yahoo.com
Received for publication: May 9, 2011
Accepted for publication: August 19, 2011
