










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.1 Joinville Jan./Mar. 2012
ORIGINAL RESEARCH ARTICLE
Child abuse: perception and management of the Brazilian endodontists
Estela Maris Losso I ; Glaucia Marengo I; Maria Carolina El Sarraf I ; Flares Baratto-Filho I
I Positivo University– Curitiba – PR - Brasil
ABSTRACT
Introduction: In Brazil, dentists have a legal, moral, and ethical obligation to notify competent authorities of suspected cases of maltreatment. Studies conducted in several countries reported the difficulties of dentists in the diagnosis, documentation, and reporting of suspected abuse cases to authorities. Objective: The aim of this study was to investigate the perception, diagnosis and attitudes of Brazilian endodontists towards child abuse. Material and methods: Data were collected from 56 questionnaires, considering a total of 248 sent by mail (response rate = 23%) to the endodontists (female = 73%). Results: Forty-one percent (n = 23) of the professionals answered that they were able to identify cases of abuse, while 59% (n = 33) answered that they were unable. Considering their graduation years, 93% (n = 52) stated that they had received little information on this issue, and only 5% (n = 3) attended seminars on this subject during the year before the questionnaire's application. Although 61% (n = 34) of the professionals affirmed that suspicious cases must be reported, only 30% (n = 17) knew to whom. Eighteen percent (n = 10) of the endodontists reported they had already treated suspicious cases, although only 3.5% (n = 2) reported the case to the authorities. The most cited signs of abuse were: body bruises (48%; n = 27), change in behavior (48%; n = 27) and burn marks (12.5%; n = 7). Lesions presented in the face, mouth, and teeth were reported by 27% (n = 15) of the professionals. There were no statistically differences regarding the number of notifications in relation to either the number of years since graduation or the workplace. Conclusion: It was concluded that it is necessary to improve endodontists' formation concerning to child abuse identification, in order to modify their behavior, therefore, increasing the number of suspicious cases' notifications.
Keywords: child abuse; child neglect; dental education; identification; reporting.
Introduction
Violence is an increasingly worldwide concern. Unfortunately, children and teenagers are part of this reality. On one hand, Brazilian Ministry of Health (2005) revealed that about 200,000 children and teenagers stated that they had undergone physical aggression 5. On the other hand, these data may not represent the real situation, because according to World Health Organization, only one in 20 cases is notified to the responsible agencies 3.
Child neglect, physical and even sexual aggression can be identified at the dental office, because 50% to 67% of the physical lesions resulting of child and teenage abuse occurs in the face and oral cavity 8,16,17. Consequently, the dentist is the health-area professional who is very likely to see a child or teenager victim of abuse, first; accordingly, the dentist should be able to recognize a case of child/teenager abuse 17.
Studies performed in several countries have reported dentists' difficulty in diagnosing, documenting, and notifying suspicious cases to the qualified authorities; consequently, there is a sub-notification of the suspicious cases 7,12,14,23. Studies undertaken in some Brazilian cities also revealed the general and pediatric dentists' necessity of more information due to the sub-notification of suspicious cases 2,9,10,20. These studies' respondents reported that they did not know how to document the case and that they were uncertain about its diagnosis. Although this subject is considered important, most of the professionals still ignore the correct attitude towards suspicious cases of abuse 3,10,14,22.
In 2007, the city of Curitiba (State of Paraná, Brazil) had 1,700,000 inhabitants, and presented 3,471 suspicious cases of child/teenager abuse. In the following year, 5,003 cases were notified; 4,735 child/teenager abuse cases were suspected or confirmed in 2009. Also, data of 2009 revealed that 88% of the cases occurred within the family, comprising: 66% of neglect; 15% of physical aggression; 10% of sexual aggression; 6.9% of psychological abuse; and 1% of abandonment. The most notified ages were from 5 to 14 years-old, although violence cases from prenatal to 18 years-old were recorded 15. The Brazilian dentist, as a citizen, has the legal, ethical, and moral responsibility of notifying suspicious cases of abuse to the competent authorities, based on the Federal Constitution and on the Child and Adolescent Rights 5.
Routinely, endodontists may be the most searched professional for performing emergency treatment. Therefore, they must recognize the suspicious cases of abuse, once physical aggression may cause dental trauma. John et al. 12 studying the professional's experience in relation to child abuse, reported that endodontists, among other professionals, had performed sub-notifications of suspicious cases and had had difficulty in diagnosing such cases. The aim of this study was to assess the diagnosis, perception, and management towards child abuse of the endodontists of the City of Curitiba, State of Parana, Brazil.
Material and methods
Questionnaires were sent to all Endodontists subscribed as specialists at the Regional Dentistry Council of the State of Paraná (CRO-PR), until May, 2009 (n = 248), located at the City of Curitiba, Paraná, Brazil.
The questionnaire consisted of 17 questions (16 structured and one semi-structured). The survey instrument was developed and revised to eliminate duplication or distorted responses. In a pilot study, the items of the questionnaire showed good reliability, with live interview (kappa = 1.0) and in test-retest design (kappa = 0.77-1.0).
The structured questions assessed the profile of professionals, such as age, gender, year of graduation, place of work (private, public clinic, and university professor), average number of children examined per week, child abuse education received during undergraduate studies and in the past year, and self-evaluation regarding the ability to diagnose suspected cases of maltreatment. In this phase, the questionnaire also included a question about whether the dentist is aware that he is legally obligated to report suspected cases of abuse against children and adolescents, which institution should be notified, and whether he had examined any children with suspected abuse and reported it. The dentist was also asked about what action should be taken in cases of child abuse. The semi-structured question was related to diagnosis, and the professional had to indicate three signs of child abuse that he knew. It was taken into consideration exactly what was mentioned by the professionals. Included in this category were situations which indicated changes in behavior.
The questionnaires and consent form were mailed to the professionals, together with stamped and addressed envelopes so that the questionnaires could be returned to the researchers. Those who returned a completed questionnaire were considered consenting because sending a consent form for signature would identify the participant, which could reduce the likelihood of their participation. Limit date was established for questionnaire return. The study was approved by the Ethical Committee in Research of the Positive University, Paraná, Brazil (protocol number #004/2009). All data were tabulated and recorded in an Excel database. Fischer's exact test was applied for statistical analysis.
Results
Out of the 248 questionnaires sent, 56 were returned (23%). Female participants corresponded to 73%. There were no statistically significant differences regarding to the number of notifications when the variables "time since graduation" (p = 0.68) or "workplace" (p = 0.88) were analysed.
Table I and II show the number of professionals according to the variables "time since graduation" and "workplace" (public, private, private and public, university professors). Concerning to the variable "time since graduation", most of the sample presented more than 13 years since graduation. Fifty percent of the professionals work at private offices.
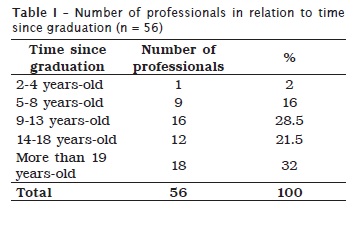
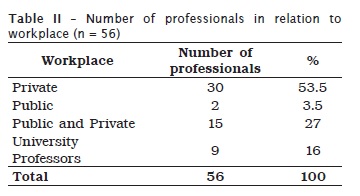
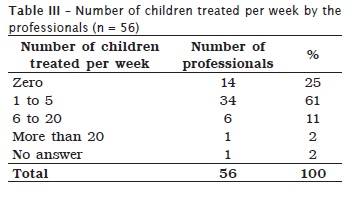
Table III presents the number of children treated per week by the professionals. Most of them treated up to 5 children per week; only one professional treated more than 20 children per week. This shows the great variability of treatments performed by this professional group.
When answering the question about whether they considered that the information about child abuse provided in their graduation years was insufficient, 52 (93%) professionals stated that they had little information. On the other hand, only 1 professional attended a seminar on this subject in the previous year. Concerning to the capacity of identifying suspicious cases of abuse, 23 (41%) professionals affirmed that they were able to recognize, while 33 (59%) were not.
Although 34 (61%) professionals declared that to report child abuse cases is demanded, only 17 (30%) knew to whom they should notify. Despite the fact that 10 (18%) professionals had reported suspicious cases of abuse, only 2 (3.5%) notified it to the competent authorities.
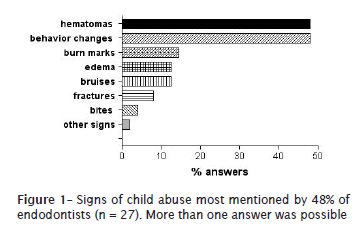
Figure 1 represents the child abuse signs most cited by the Endodontists. Hematomas (48%; n = 27) and behavior changes (48%; n = 27) where the most signs reported. Eight (14%) professionals did not answer this question
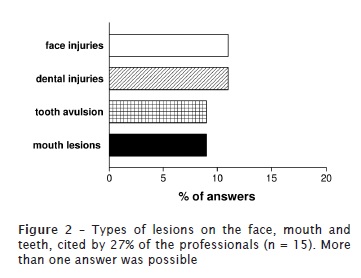
Figure 2 represents the orofacial lesions caused by abuse cited by the professionals. Only 27% (n = 5) of the professionals reported lesions in this area. The most cited lesion was "lesion in the face".
Discussion
The worldwide difficulty of obtaining statistical and epidemiological information on child abuse may reflect the lack of notification of the suspicious cases. Lack of information regarding both to the diagnosis and knowledge of the obligation of notifying suspected cases, probably resulted in their sub-notification. This study's results met this situation, because only 2 out of 10 suspected cases were notified. The same situation was verified in Scotland, where a study reported that 21% of the dentists treated suspected cases and did not report them to the competent authorities 6. This is also confirmed by the results of studies carried out in other Brazilian areas and other countries 2,4,7,12,13,14,18,19,21. The cases' sub-notification may be explained by the fact that only 41% of the professionals felt they were capable of recognizing suspected cases. Besides the diagnosis, other factors may contribute for the cases' sub-notification: fear of violence against the child, fear of retaliation by the family, and legal issues 2,4,7,13,14,18,19,22,23.
Thirty percent of the participants knew to which institution they should notify the suspicious cases. This result was lower than an Australian study result, where the delation is not mandatory in all states, in which 49% of the participants knew to which institution would receive the delation 12.
Most of this study's professionals affirmed they did not receive sufficient information on child/teenager abuse during their graduation years. Literature confirmed dentists' necessity of receiving more information on this issue in order to diagnose and manage child abuse cases, properly 2,6,13,23,12,18.
The dentist may recognize possible abuse signs if the child or teenager presents facial, dental, or soft tissue lesions, at the appointments, without any coherent explanation compatible with the clinical finding. Head, neck, face, and mouth are the most injured areas in physical aggression cases 8. Conversely, the lesions most cited by the participants of this study were body bruises and behavior changes. In this study, only 27% of the professionals cited the lesions in head, neck, face, and mouth as suspected of abuse. Similarly, John et al. reported that 99% and 37% of 102 endodontists cited body and oral lesions, respectively, as the most found lesions. Also, the fact that eight professionals did not answer this question reinforces the importance of divulging this issue to dentists. A startling fact is that neglect and physical aggression corresponded to 81% (3,835) of the cases notified in the City of Curitiba, in 2009. In these situations, the dentist can be the first professional to see the children 15. As defined by the American Academy of Pediatric Dentistry 1, dental neglect is the "willful failure of parent or guardian to seek and follow through with treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection". Neglect of oral origin must be investigated in order to verify if it is a result of lack of knowledge or abandonment. The latter is characterized by the delay in seeking for emergence treatment in cases of dental trauma and pain due to pulp origin. Therefore, it is demanded that the endodontist and the auxiliary team recognize abuse signs or at least suspect of its possibility, searching for solutions. Also, it is necessary that the dentists know how to proceed, properly, regarding to legal procedures to be taken in these situations 15.
References
1. AAPC. American Academy of Pediatrics. American Academy of Pediatric Dentistry Council on Clinical Affairs. Guideline on oral and dental aspects of child abuse and neglect. Pediatr. 1999;104:348-50.
2. Andrade LK, Colares V, Cabral HM. Avaliação da conduta dos odontopediatras de Recife com relação ao abuso infantil. Rev Odonto Ciênc. 2005;20:231-6.
3. Associação Brasileira Multiprofissional de Proteção à Infância e à Adolescência (Abrapia). Maus-tratos contra crianças e adolescentes: proteção e prevenção. Guia de orientação para profissionais da saúde. 2. ed. 1997.
4. Bankole OO, Denloye OO, Adeyemi AT. Child abuse and dentistry: a study of knowledge and attitudes among Nigerian dentists. Afr J Med Med Sci. 2008;37:125-34.
5. Brasil. Lei n.º 8069, de 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. [cited 2011 Nov 2]. Available from: URL: http://www.planalto.gov.br/ccivil/LEIS/L8069.htm.
6. Cairns AM, Mok JY, Welbury RR. Injuries to the head, face, mouth and neck in physically abused children in a community setting. Int J Paed Dent. 2005;15:310-8.
7. Cairns AM, Mok JY, Welbury RR. The dental practitioner and child protection in Scotland. Br Dent J. 2005;199:517-20.
8. Cavalcanti AL. Prevalence and characteristics of injuries to the head and orofacial region in physically abused children and adolescents a retrospective study in a city of the Northeast of Brazil. Dent Traumatol. 2010;26:149-53.
9. Granville-Garcia AF, Menezes VA, Silva PFR M. Maus-tratos infantis: percepção e responsabilidade do cirurgião-dentista. Rev Odonto Ciênc. 2008;23:35-9.
10. Granville-Garcia AF, Silva MJF, Menezes VA. Maus-tratos a crianças de adolescentes: um estudo em São Bento do Una, PE, Brasil. Pesq Bras Odontoped Clín Integr. 2008;8:301-7.
11. Harris JC, Elcock C, Sidebotham PD, Welbury RR. Safeguarding children in dentistry: 1. Child protection training, experience and practice of dental professionals with an interest in paediatric dentistry. Br Dent J. 2009;206:409-14.
12. John V, Messer LB, Arora R, Fung S, Hatzis E, Nguen T et al. Child abuse and dentistry: a study of knowledge and attitudes among dentists in Victoria, Australia. Aust Dent J. 1999;44:259-67.
13. Lazenbatt A, Freeman R. Recognizing and reporting child physical abuse: a survey of primary healthcare professionals. J Adv Nurs. 2006;56:227-36.
14. Manea S, Favero GA, Stellini E, Romoli L, Mazzucato M, Facchin P. Dentists' perceptions, attitudes, knowledge, and experience about child abuse and neglect in northeast Italy. J Clin Ped Dent. 2007;32:19-25.
15. Muraro HMS. Relatório da rede de proteção à criança e ao adolescente em situação de risco para a violência, Curitiba, 2009 [cited 2010 Oct 18]. Available from: URL:http://sitesms.curitiba.pr.gov.br/saude/areastematicas/saude_crianca/RELATORIOPERFILREDE2009.pdf.
16. Naidoo S. A profile of the oro-facial injuries in child physical abuse at a children's hospital. Child Abuse Negl. 2000;24:521-34.
17. Nuzzolese E, Lepore MM, Montagna F, Marcario V, De Rosa S, Solarino B et al. Child abuse and dental neglect: the dental team's role in identification and prevention. Int J Hygiene. 2009;7:96-101.
18. Owais AI, Qudeimat MA, Qodceih S. Dentists' involvement in identification and reporting of child physical abuse: Jordan as a case study. Int J Paed Dent. 2009;19:291-6.
19. Russell M, Lazenbatt A, Freeman R, Marcenes W. Child physical abuse: health professionals' perceptions, diagnosis and responses. Br J Community Nurs. 2004;9:291-7.
20. Santos JF, Nunes KS, Cavalcanti AL, Silva EC. Maus-tratos infantis: conhecimento e atitudes de odontopediatras de Uberlândia e Araguari, Minas Gerais. Pesq Bras Odontop Clín Integr. 2006;6(3):273-9.
21. Silveira JLC, Mayrink S, Oliveira Neto OB. Maus-tratos na infância e adolescência: casuística, conhecimento e prática de cirurgiões-dentistas de Blumenau (SC). Pesq Bras Odontop Clín Integr. 2005;5:119-26.
22. Thomas JE, Straffon L, Inglehart MR, Habil P. Knowledge and professional experiences concerning child abuse: an analysis of provider and student responses. Pediatr Dent. 2006;28:438-44.
23. Uldum B, Christensen HN, Welbury R, Poulsen S. Danish dentists' and dental hygienists' knowledge of and experience with suspicion of child abuse or neglect. Int J Paed Dent. 2010;20:361-5.
 Correspondence:
Correspondence:
Estela Maris Losso
Universidade Positivo
Rua Pedro Viriato Parigot de Souza, n.º 5.300 – Campo Comprido
CEP 81280-330 – Curitiba - PR - Brasil
E-mail: emlosso@up.edu.br
Received for publication: December 10, 2010
Accepted for publication: June 24, 2011
