










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.2 Joinville Abr./Jun. 2012
Original Research Article
Cutting ability of nickel-titanium rotary systems ProTaper, Mtwo and K3
Sergio Herrero Moraes I; Marcelo Gonçalves I; Mário Tanomaru Filho I; Idomeo Bonetti Filho I
I São Paulo State University Júlio de Mesquita Filho – Araraquara – SP – Brazil.
ABSTRACT
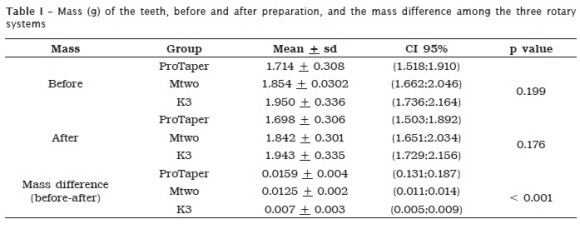
Introduction: Nickel-titanium rotatory systems should remove dentin during the root canal preparation to promote the enlargement and tapered shape with continuously narrowing towards the apex. Objective: The aim of this study was to analyze the cutting ability of three NiTi rotatory systems (n = 12): ProTaper (group 1), Mtwo (group 2), and K3 (group 3). Material and methods: Thirty six maxillary molar teeth were weighted on an analytical balance before and after the rotatory preparation of the mesio-buccal root canal. Data was statistically analyzed by ANOVA and Tukeys test with a significance level of 5%. Results: The results revealed the following mass differences (g) before and after the root canal preparation: ProTaper (group 1 – 0.0159 ± 0.004), Mtwo (group 2 – 0.0125 ± 0.002), and K3 (group 3 – 0.007 ± 0.003). Conclusion: ProTaper showed the highest cutting ability among the three tested nickel-titanium rotatory systems followed by Mtwo and K3.
Keywords: Endodontics; instruments; root canal preparation.
Introduction
Among the properties of NiTi Rotary system, their flexibility, cutting ability, resistance to fracture and elastic memory have been highlighted 3,4,11,22,17,32,34.
The cutting ability of endodontic instruments has been evaluated in wet bovine bone because of the instruments cutting depth, with either linear filling movements 18,15,35, at traction movements with controlling of force, pressure, amplitude and number of movements 1,39, or with ¼-turn clockwise rotation 10. The cutting depth of the instrument has also been evaluated in polymethylmethacrylate blocks and artificial root canals made of epoxy resin 1,16,29,24,30 and Plexiglass plate 10. The cutting ability was measured based on the removal of the Plexiglass mass weighed in analytical balance 10. Schäfer and Lau 23 compared the cutting efficacy of NiTi instruments in curved canals of extracted teeth. Carvalho-Souza et al. 6 evaluated by using Gates Glidden rotary instruments and ProTaper, the thick of the remnant dentin in mandibular molars extracted and included in rein blocks, before and after their preparation.
Computed tomography has also been used to evaluate tridimensionally root canal preparation once it enables the observation of root canal shape, volume increasing and center and the cutting ability of the instrument 8,24,27,33. The efficacy of the cutting efficacy of NiTi instruments is analyzed by the cuts of the cervical, medium and apical thirds of natural or artificial teeth, measured before and after root canal preparation.
The aim of this study was to analyze the cutting ability of three NiTi rotary systems: ProTaper, Mtwo and K3.
Material and methods
To conduct this study, 36 maxillary molar human teeth coming from the tooth bank of the Araraquara School of Dentistry (São Paulo State University – short Unesp) were used. This study was approved by the Ethical Committee in Research. The teeth were stored in 0. 1% thymol solution for 30 days. Next, they were washed in tap water to eliminate this solution for 2 hours. Following, radiographic shots were taken through portable x-ray device (Heliodent, Siemens, São Paulo, SP, Brazil – 60 kV, 10 mA) to verify root canal internal anatomy and the curvature degree of the mesio-buccal root. Apical curvature was determined by using the method of Schneider 26, with the aid of the software Image J (www.rsb.info.nih.gov/ij). Inclusion criteria comprised teeth presenting apical curvature from 20º to 40º at mesial-distal direction. Caries lesions, metallic restorations and distal-buccal roots were removed. The surgical access of the teeth was accomplished through diamond burs #1012, #2082 (KG Sorensen, Cotia, São Paulo, SP, Brazil), mounted in handpiece at high speed and long carbide round bur (28 mm; size #2) (Dentsply-Maillefer, Petrópolis, RJ, Brazil), mounted in handpiece at low speed. Mesial-buccal canal was negotiated and the patency was verified through a K file size #10. The teeth were weighed in analytical balance (Bioprecisa, São Paulo, SP, Brazil) and embedded in condensation silicone impression material (Vigodent, Rio de Janeiro, RJ, Brazil), mounted in acrylic platform, adapted from the method of Southard et al. 29, to standardize the position of the teeth during root canal preparation. The teeth were divided into three groups of 12 teeth each with mesial-distal curvatures in mesial-buccal root from 20º to 29º (6 teeth) and from 30º to 40º (6 teeth).
In the three groups, working length was established with a K file size #10 until root canal patency, confirmed through periapical radiographs The NiTi rotary systems evaluated in this study were: group 1: ProTaper – Universal (Dentsply-Maillefer, Ballaigues, Switzerland); group 2: Mtwo (VDW, Bayerwaldstr-München, Germany); and group 3: K3 (Sybron-Endo, Orange, CA, USA). In all teeth, before the preparation, at every instrument change and at the preparation ending, root canal were irrigated with 1% sodium hypochlorite with the aid of a 3 ml plastic syringe and 30 Gauge needle and Endo-Eze tip (Ultradent, Salt Lake City, USA), up to 2 mm shorter of the apical foramen. At the ending of the preparation, a capillary tip plastic needle (Ultradent, Salt Lake City, USA) with 0.014 inch caliper, coupled to a metallic cannula and to the suction unit (Dabi Atlante, Ribeirão Preto, SP, Brazil) of the dental chair with pump suction, was introduced up to the apical third for the aspiration of possible dentin debris and residual irrigant. Apical preparation diameter and the velocity, torque and time elapsed for preparation for each root canal were standardized, respectively in 0.30 mm, 250 rpm, 1.6 Ncm and 30 seconds. For root canal preparation, the X-Smart motor (Dentsply-Maillefer, Ballaigues, Switzerland) was employed. ProTaper instrument sizes S1, S2, F1, F2, F3; Mtwo instrument sizes 10/04, 15/05, 20/06, 25/06 30/05; and K3 instrument sizes 25/08, 15/04, 20/04, 25/06, 30/04 were used. In ProTaper and Mtwo systems, all instruments were introduced up to the apical foramen (patency) as working length. In K3 system, the instrument size 25/08 was used to access the cervical third and the other instruments were used up to the apical foramen. The instruments were inserted with linear back-and-forth movements without apical pressure up to reach the apical foramen. When the instrument found some resistance, the self-reverse mechanism of the device was automatically driven. In this case, new back-and-forth movements were initiated up to reach the apical foramen. Each instrument was used four times. All groups were prepared by the same examiner. After root canal preparation and irrigation, all canals were dried with 0.30 mm paper points. Next, the teeth were removed from the silicone block and again weighed on the analytical balance. The aim was to analyze the cutting ability of the instruments through the mass loss (grams) after root canal preparation. Data was evaluated by one-way ANOVA and Tukey test for multiple comparisons with level of significance of 0.05.
Results
The results of the cutting ability of each instrument through the mass assessment before and after root canal preparation (initial mass minus final mass) as well as the comparison among them are seen in table I. The results indicated mass difference before and after preparation of each system. During canal preparations, only one fracture occurred: Mtwo system size #20 during its fourth use.
Discussion
For Schäfer and Vlassis (2004) 25, artificial root canals embedded in epoxy resin blocks neither reflect the behavior of root canal of the human tooth nor the dentin structure nor its removal. Nevertheless, in human tooth, because of the great variety of the internal and external anatomy, the age of the patient when losing the tooth, presence of restorations and caries lesions, it is very difficult to standardize the studys groups. However, this is one advantage of epoxy resin artificial root canal, in which it is possible to standardize the diameter, length and curvatures. Sonntag et al. (2007) 28, in a same study, associated extracted human teeth and epoxy-resin root canals. The results of epoxy-resin canals were higher than those with human teeth, just because of the possibility in standardizing the canals regarding to the curvature, length and diameter.
In this present study, the cutting ability of ProTaper, Mtwo and K3 rotary instruments were analyzed through the mass loss of the tooth during root canal preparation. The parameter employed was the analytical balance, weighing the tooth before and after the preparation. Velocity, torque and time of the instruments were standardized. Root canal preparations were executed by the same examiner; force and pressure were not calibrated. To avoid greater variation in rotary instrument insertion, the linear movement was standardized for the three groups. This movement was appropriate because all instruments reached the patency of root canal without difficulty. Other methods, such as cutting depth and canal volume increase, have also been employed to analyze the cutting ability of the instruments 24,28,33. Although human tooth simulates the clinic situation regarding to the material, it may have variations in the calcification and hardness of the substrate, because of the age and substrate site; this same pattern also occurred in bovine tooth. Notwithstanding, methods employing materials different from human teeth does not mimic the clinical condition.
In the three groups analyzed, there was only one instrument fracture, in group 2, (size #20; Mtwo). This tooth showed a curvature of 36.7º in mesial-buccal root, close to the maximum curvature included in this study (40º). The instrument fracture occurred in its fourth use, at apical third and within working length, with fragment of about 2 mm. By using torque below 1.6 N when the instrument found a resistance, the self-reverse device was automatically driven, which may contribute to avoid the fracture of a greater number of instruments. Sonntag et al. 28 recorded a fracture of ProTaper and Mtwo instruments, but none with K3, when these three systems were used in the preparation of mandibular human molars. The instrument fracture may be associated to several factors, such as torque, fatigue, curvature radius and degree, instrument diameter, geometry, number of uses, preparation velocity and torque 20. Yared and Kulkarni 38 tested the torque at 1.3 Ncm, 1.1 Ncm and 0.75 Ncm of five motor devices (Tulsa Dentsply) for NiTi rotary instruments. They concluded that the actual torque was higher than that recorded by the device’s display. Also, these authors affirmed that some fractures in Profile instruments occurred because of the torque discrepancy. The geometry of the cross-cut section, the cutting angle of the blade, the instrument tip, and the tapering have been reported by several authors as determining factors in the cutting ability and resistance to flexion and torsion 3,4,12,14. This study’s instruments differed among each other regarding their geometric shape of the cross-cut section. The ProTaper instrument presents a convex triangular section with three cutting blades, while Mtwo presents a rectangular S-shape section with double cutting angle, and K3 shows a section with two radial planes and one cutting blade, totaling three asymmetrical surfaces. Berutti et al.4 affirmed that Profile presents greater flexibility than ProTaper instrument because of its 30% smaller area. However, after force application, ProTaper demonstrated the best tension distribution when compared with Profile. Uyanik et al. 33 also concluded that ProTaper removed the greatest amount of dentin than HeroShaper, but without significant difference when compared to RaCe system. Kim et al. 13 studied the mechanic reactions of NiTi Profile, Hero Shaper, Mtwo and NRT instruments. The results showed that rectangular cross-section sections, as Mtwo and NRT, created more tension during the preparation simulation with 1 and 2 Ncm, velocity of 240 rpm, and they may find more residual tension and plastic deformation than triangular cross-section instruments. Shen and Haapasalo 27 used the volume loss through computed tomography before and after preparation. These authors reported that is very difficult to evaluate the mass loss of NiTi instruments because of the low power of their cuttings. Accordingly, in this present study, the mass difference, before and after preparation, found in each system was very small. A statistically significant difference was found among ProTaper, Mtwo and K3. Plotino et al. 21 did also not noted statistically significant difference in the amount of dentin removed at the coronal third of the root between ProTaper and Mtwo. One possible explication for the greater amount of dentin removed by the instrument may be attributed by the difference of taper regarding to Mtwo and K3. Wu et al. 36 verified that in 25% of the cases, the instrument are not supposed to touch all root canal walls during preparation. Wu et al. 37 recorded that the single mesial-buccal canal diameter of the maxillary molar at 1 mm shorter of the apex is 0.43 mm; at 5 mm shorter of the apex is 0.96 mm in buccal-palatal direction and 0.22 mm and 0.29 mm in mesial and distal direction, respectively. The findings of these authors may explain the small mass loss of the teeth after the use of the three rotary systems in our study, when compared with studies on bovine bone, dentin discs and epoxy-resin canals. Shen and Haapasalo 27 emphasized that root canal lubrication with the irrigant during preparation make easy the contact between the cutting blade of the instrument and the dentin, decreasing friction. Some studies 5,7,9,19 have shown that NaOCl attacks the organic matrix of the dentin and reduces the microhardness of radicular dentin, making the preparation easier. Shen and Haapasalo 27 found less compression force and more cutting efficacy in these following NiTi rotary systems: Hero Shaper, FlexMaster, K3, Libertor, Alpha and Profile on bovine femur after irrigation with NaOCl compared to a dried canal. Among them, FlexMaster and K3 removed greater volume of bovine bone both in wet and dried canal. The treatment surface of the NiTi instrument (bhorio ion implantation; thermal nitridation process; deposition of titanium nitride by physical vapor; cryogenic, argon and nitrogen treatment) may increase the cutting efficiency of NiTi instrument 2,9,24,40. Shen and Haapasalo 27 well emphasized that the dentin cutting is an essential step during endodontic treatment. It enormously contributes to the removal of infected dentin and promotes a proper tapering to the prepared canal.
Conclusion
Considering the limitations of this study, it can be concluded that the cutting capacity of nickel-titanium rotary systems was descending for the systems: ProTaper, Mtwo, and K3.
References
1. Anderson JV, Corcoran JF, Craig RG. Cutting ability of square versus rhombus cross-sectional endodontic files. J Endod. 1985;11:212-7. [ Links ]
2. Alapoti SB, Brantley WA, Iijima M, Clark WAT, Kovarik L, Buie C et al. Metallurgical characterization of a new nickel-titanium wire for Rotary endodontic instruments. Endod J. 2009;35:1589-93.
3. Bahia MGA, Melo MCC, Buono VTL. Influence of simulated clinical use on the torsional behavior of nichel-titanium rotary endodontic instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:675-80.
4. Berutti E, Chiandussi G, Gaviglio I, Ibba A. Comparative analysis of torsional and bending stresses in two mathematical models of nickel-titanium rotary instruments: ProTaper versus ProFile. J Endod. 2003;29:15-9.
5. Bui TB, Mitchell JC, Baumgartner. Effect of electropolishing Profile nickel-titanium rotary instruments on cyclic fatigue resistance, torsional resistance, and cutting efficiency. J Endod. 2008;34:190-3.
6. Carvalho-Souza B, Costa-Filho JR, Almeida-Gomes FA, Maniglia-Ferreira C, Gurgel-Filho ED, Albuquerque DS. Evaluation of the dentin remaining after flaring using Gates Glidden drills and Protaper rotary files. RSBO. 2011;8:194-9.
7. Elmsallati EA, Wadachi R, Ebrahim AK, Suda H. Debris retention and wear in three different nickel-titanium rotary instruments. Aust Endod J. 2006;32:107-11.
8. Fayyad DM, Elgendy AAE. Cutting efficiency of twisted versus machined nickel-titanium endodontic files. J.Endod. 2011;37:1143-6.
9. Guillot MPC, Badet C, Peli JF, Perez F. Effect of nickel-titanium rotary file techniques on infected root dentin reduction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:254-8.
10. Haïkel Y, Serfaly R, Lwin T-TC, Allermann C. Measurement of the cutting efficiency of endodontic instruments: a new concept. J Endod. 1996;22:651-6.
11. Inan U, Aydin C, Tunca YM. Cyclic fadigue of ProTaper rotary nickel-titanium instruments in artificial canals with 2 different raddi of curvature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104:873-4.
12. Iqbal MK, Firic S, Tulcan J, Karabucak B, Kim S. Comparison of apical transportation between ProFile and ProTaper NiTi rotary instruments. Int Endod J. 2004;37:359-64.
13. Kim HC, Kim HJ, Lee CJ, Kim BM, Park JK, Versluis A. Mechanical response of nickel-titanium instruments with different cross-sectional designs during shaping of simulated curved canals. Int Endod J. 2009;42:593-602.
14. Ktir A, Rosenberg E, Fuss Z. Comparison in vivo of the first tapered and nontapered instruments that bind at apical constriction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:395-8.
15. Miserendino LJ, Moser JB, Heuer MA, Osetek EM. Cutting efficiency of endodontic instruments. Part II: analysis of tip design. J Endod. 1986;12:8-12.
16. Miserendino LJ, Brantley WA, Walia HD, Gerstein H. Cutting efficiency of endodontic hand instruments. Part 4. Comparison of hybrid and traditional instruments designs. J Endod. 1988;14:451-4.
17. Necchi S, Taschieri S, Petrini L, Migliavacca F. Mechanical behavior of nickel-titanium rotary endodontic instruments in simulated clinical conditions: a computational study. Int Endod J. 2008;41:939-49.
18. Newman JG, Brantley WA, Gerstein H. A study of the cutting efficiency of seven brands of endodontic files in linear motion. J Endod. 1983;9:316-22.
19. Passarinho-Neto JG, Marchesan MA, Ferreira RB, Silva RG, Silva-Sousa YTC, Sousa-Neto MD. In vitro evaluation of endodontic debris removal as obtained by rotary instrumentantation coupled with ultrasonic irrigation. Aust Endod J. 2006;32:123-8.
20. Peters OA, Barbakow F. Dynamic torque and apical forces of ProFile .04 rotary instruments during preparation of curved canals. Int Endod J. 2002;379-89.
21. Plotino G, Grande NM, Sorci E, Malagnino VA, Somma F. Influence of a brushing working motion on the fadigue life of NiTi rotary instruments. Int Endod J. 2007;40:45-51.
22. Pruet JP, Clement Dj, Carnes DL. Cyclic fatigue of nickel-titanium endodontic instruments. J Endod. 1997;23:77-85.
23. Schäfer E, Lau R. Comparison of cutting efficiency and instrumentation of curved canals with nickel-titanium and stainless-steel instruments. J Endod. 1999;25:427-30.
24. Schäfer E, Oitzinger M. Cutting efficiency of five different types of rotary nickel-titanium instruments. J Endod. 2008;34:198-200.
25. Schäfer E, Vlassis M. Comparative investigation of two rotary nickel-titanium instruments: ProTaper versus RaCe. Part I: shaping ability in simulated curved canals. Int Endod J. 2004;37:229-38.
26. Schneider SW. A comparison of canal preparation in straight and curved root canal. Oral Surg Oral Med Oral Pathol. 1971;32:271-5.
27. Shen Y, Haapasalo M. Three-dimensional analysis of cutting behavior of nickel-titanium rotary instruments by microcomputed tomography. J Endod. 2008;34:606-10.
28. Sonntag D, Ott M, Kook K, Stachniss V. Root canal preparation with the NiTi systems K3, Mtwo and ProTaper. Aust Endod J. 2007;33:73-81.
29. Southard DW, Oswald RJ, Natkin E. Instrumentation of curved molar root canals with the Roane technique. J Endod. 1987;13:479-89.
30. Tepel J, Schäfer E, Hoppe W. Properties of endodontic hand instruments used in rotary motion. Part I. Cutting efficiency. J Endod. 1995;21:118-21.
31. Tripi TR, Banaccorso A, Condorelli GG. Cyclic fatigue of different nickel-titanium endodontic rotary instruments. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:106-14.
32. Usman N, Baumgartner JC, Marshall JG. Influence of instrument size on root canal debridement. J Endod. 2004;30:110-2.
33. Uyanik MO, Cebreli ZC, Mocan BO, Dagli FT. Comparative evaluation of three nickel-titanium instrumentation systems in human teeth using computed tomography. J Endod. 2006;32:668-71.
34. Walia H, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of nitinol root canal files. J Endod. 1988;14:346-51.
35. Webber J, Moser JB, Heuer MA. A method to determine the cutting efficiency of root canal instruments in linear motion. J Endod. 1980;6:829-34.
36. Wu MK, Roris A, Barkis D, Wesselink PR. Prevalence and extent of long canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endodod. 2000;89:739-43.
37. Wu MK, Barkis D, Roris A, Wesselink PR. Does the first file to bind correspond to the diameter of the root canal in the apical region? Int Endod J. 2002;35:264-7.
38. Yared G, Kulkarni GK. Accuracy of the DTC torque control motor for nickel-titanium rotary instruments. Int Endod J. 2004;37:399-402.
39. Yguel-Henry S, Vannesson H, Stebut JV. High precision, simulated cutting efficiency measurement of endodontic root canal instruments: influence of file configuration and lubrication. J Endod. 1990;16:418-22.
40. Zinelis S, Darabara M, Takase T, Ogane K, Papadimitriou GD. The effect of thermal treatment on the resistance of nickel-titanium rotary files in cyclic fatigue. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;103:843-7.
 Correspondence:
Correspondence:
Sergio Herrero Moraes
Departamento de Odontologia Restauradora
Rua Prefeito Lothário Meissner, n.º 632 – Jardim Botânico
CEP 80210-170 – Curitiba – PR – Brasil
E-mail:herrero@herrero.com.br
Received for publication: June 08, 2011.
Accepted for publication: December 19, 2011.
