










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.2 Joinville Abr./Jun. 2012
Case Report Article
An unusual case of oral leiomyoma mimicking a gingival epulis
Gurukiran Kaur I ; Sunitha Carnelio II ; Gabriel Rodrigues III
I Department of Oral and Maxillofacial Pathology, Gian Sagar Dental College – Rajpura – Punjab – India.
II Department of Oral and Maxillofacial Pathology, Manipal College of Dental Sciences, Manipal University – Manipal – Karnataka – India.
III Department of Surgery, Kasturba Medical College, Manipal University – Manipal – Karnataka – India.
ABSTRACT
Introduction: Leiomyoma, the commonest benign tumor of the uterus is a rare occurrence in the oral cavity and when present mimics various other soft tissue tumors of the oral cavity and lead to a diagnostic dilemma to the clinician. Objective and case report:The low incidence of this lesion, the unusual location, and its histomorphological pattern of presentation which needs to be differentiated from other spindle cell lesions posing a diagnostic challenge makes the report of this case worthy in a 32-year-old male, with a soft tissue swelling of the right lower gingiva which appeared to be an epulis but finally turned out to be a leiomyoma. Conclusion: Histopathology is the only means by which a diagnosis can be arrived at and at times might require special stains for a definitive diagnosis.
Keywords: leiomyoma; epulis; immunohistochemistry; excision.
Introduction
Leiomyomas are benign smooth muscle tumors that are relatively common, especially in the uterus (about 95%) followed by the gastrointestinal tract and skin 2. These tumors represent only 0.4% of all soft tissue lesions in the oral cavity and present as slow-growing, asymptomatic submucosal masses, the common sites being the tongue, hard palate and buccal mucosa 9. The aim of the present study is to report an unusual case of oral leiomyoma mimicking a gingival epulis and demonstrate the importance of the immunohistochemical results in determining the final diagnosis.
Case report
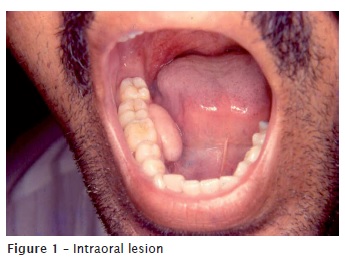
A 32-year-old male, with an unremarkable medical history of substance abuse presented with an asymptomatic swelling of the right lower jaw of one month duration. Intraoral exam revealed an exophytic, nodular, sessile swelling, freely movable over the right lower gingiva in the region of premolar-molar region (figure 1). Radiographic examination did not show any changes in the associated bone. The mass was excised under local anesthesia as a single firm 1.5 x 2 cm soft tissue mass. Macroscopically the tumor was grayish white, firm and appeared encapsulated.
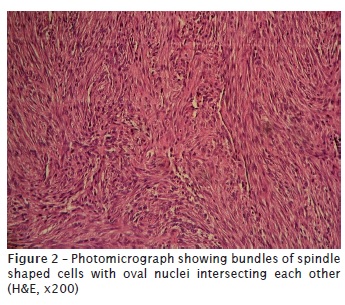
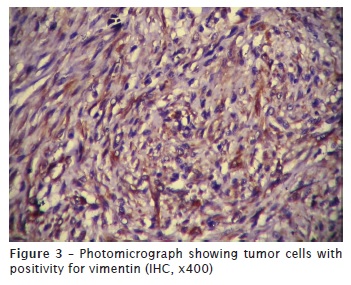
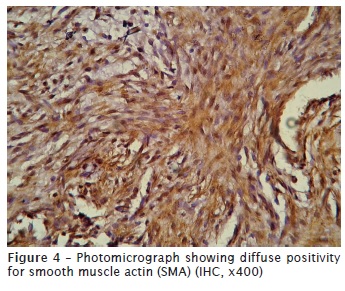
Microscopically, it was a well circumscribed tumor constituting of spindle shaped cells (figure 2), which had elongated blunt ended nuclei. The fascicles of these tumor cells were arranged in whorls and intersecting each other. No mitotic figures or necrosis were seen. For further diagnostic confirmation, Massons trichrome, a special histochemical stain was used and an immunohistochemical (IHC) study revealed a positive expression of vimentin (figure 3) and smooth muscle actin (SMA) within the tumor cells (figure 4), whereas expression of cytokeratin, desmin and S-100 was negative. These histomorphologic features and the IHC profile lead to the diagnosis of an oral leiomyoma. On follow-up, no signs of any recurrence were observed 6 months after the excision of the lesion.
Discussion and conclusion
Leiomyoma is a benign tumor of smooth muscle. The source of smooth muscle in the oral cavity is either the arterial tunica media as suggested by Stout (1937) 8, or the ductus lingualis. Those associated with the tongue are seen to arise from the smooth muscle in the region of the circumvallate papillae 1. Oral leiomyoma was first reported in 1884 and since then less than 150 cases have been published 1,9. The World Health Organization (WHO) distinguishes three types of leiomyomas: leiomyoma (solid), angiomyoma (vascular leiomyoma) and epitheloid leiomyoma (leioblastoma) 9.
Oral leiomyoma is more frequent in men than in women, as in our patient, with a 1.43:1 ratio and a peak age incidence between 40-49 years 7. Majority of the cases reported indicated an asymptomatic slow growing mass, firm to touch and the color depending on their depth and vascularity. Though these lesions are asymptomatic masses, few of them have been reported to be painful or tender, lead to difficulty in chewing or swallowing and loose teeth 9. They are not very big tumors, with an average size between 1-2 cm and with a history of less than a year 6, as in our patient. A differential diagnosis of fibrous histiocytoma, neurilemmoma or leiomyosarcoma should be considered which can be ruled out by histopathology and special stains 5. Masons trichrome and Van Geisons stains are specific for muscle cells and collagen fibers whereas Mallorys Phosphotungstic Acid (PTAH) and positive IHC marker desmin may aid to differentiate leiomyoma from other spindle cell tumors such as myofibroblastoma 4. Lack of histiocytes and multinucleated giant cells differentiates it from fibrous histocytoma while cytokeratin negativity differentiates it from a synovial tumor 3. Further, our case was S-100 negative which made us to differentiate it from neurilemmoma. Complete surgical resection is the treatment of choice with a very low recurrence rate if complete resection is achieved 7.
References
1. Allon I, Aballo S, Dayan D, Vered M. Lipomatous tumors of the oral mucosa: histomorphological, histochemical and immunohistochemical features. Acta Histochem. 2011 Mar 2. [Epub ahead of print]. [ Links ]
2. Baden E, Doyle JL, Lederman DA. Leiomyoma of the oral cavity: a light microscopic and immunohistochemical study with review of the literature from 1884 to 1992. Eur J Cancer B Oral Oncol. 1994;30B(1):1-7.
3. Brooks JK, Nikitakis NG, Goodman NJ, Levy BA. Clinicopathologic characterization of oral angioleiomyomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94(2):221-7.
4. Go JH. Benign peripheral nerve sheath tumor of the tongue. Yonsei Med J. 2002;43(5):678-80.
5. Jeffcoat BT, Pitman KT, Brown AS, Baliga M. Schwannoma of the oral tongue. Laryngoscope. 2010;120 Suppl 4:S154.
6. Liang H, Frederiksen NL, Binnie WH, Cheng YS. Intraosseous oral leiomyoma: systematic review and report of one case. Dentomaxillofac Radiol. 2003;32(5):285-90.
7. Luaces-Rey R, Lorenzo-Franco F, Gomez-Oliveira G, Patino-Seijas B, Guitian D, Lopez-Cedrun Cembranos JL. Oral leiomyoma in retromolar trigone. A case report. Med Oral Pathol Oral Cir Bucal. 2007;12(1);E53-5.
8. Stout AP. Solitary cutaneous and subcutaneous leiomyoma. Am J Cancer. 1937;29:435-69.
9. Wertheimer-Hatch L, Hatch GF 3rd, HatchB SKF, Davis GB, Blanchard DK, Foster RS Jr et al. Tumors of the oral cavity and pharynx. World J Surg. 2000;24(4):395-400.
 Correspondence:
Correspondence:
Sunitha Carnelio
Associate Professor
Department of Oral and Maxillofacial Pathology – Manipal College of Dental Sciences
Manipal – Karnataka – India
E-mail:sunithacarnelio@yahoo.co.uk
Received for publication: June 03, 2011.
Accepted for publication: September 15, 2011.
