










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.2 Joinville Abr./Jun. 2012
Case Report Article
Surgical approach and the use of cryotherapy in a keratocystic odontogenic tumor after 12 months of decompression
Carlos Eduardo Fontana I ; Carolina Davoli Macedo Ibanéz II ; Felipe Davini I ; Alexandre Sigrist De Martin I ; Cláudia Fernandes de Magalhães Silveira I ; Daniel Guimarães Pedro Rocha I; Carlos Eduardo da Silveira Bueno I
I Department of Endodontics, São Leopoldo Mandic Post-graduation Center – Campinas – SP – Brazil.
II Private practice – São Paulo – SP – Brazil.
ABSTRACT
Introduction: The knowledge of the complex anatomy of maxillary molars and location of extra canals are essential for diagnosis and endodontic treatment success. Objective: The purpose of this study was to report a clinical case showing a varying number of palatal roots in a second maxillary molar with the aid of operating microscope (OM). Case report: A four-rooted maxillary permanent second molar with 2 separated palatal canals undergone endodontic therapy. After endodontic access, examination of the chamber floor using an operating microscope revealed two distinct palatal canals orifices. A radiograph was taken after the working lengths of each canal were estimated by means of an electronic apex locator which clearly identified the four roots with independent four canals. The canals were instrumented with ProTaper rotatory instruments under irrigation with 5% sodium hypochlorite, obturated with Pulp Canal Sealer® and continue wave technique. After completion of root canal treatment, the tooth was restored with composite resin. Results: After endodontic access, the presence of two different palatal canals was found in a second maxillary molar, resulting from a variation in the number of palatal roots of this tooth. Conclusion: The high magnification and clear illumination quality provided by the dental operating microscope increase endodontic treatment success of the variations in the internal anatomy of the tooth.
Keywords: internal anatomy; endodontic treatment; maxillary second molar; dental operating microscope.
Introduction
The knowledge of the internal anatomy of root canal system and its possible variations is related to the parameters of endodontic therapy execution, directly affecting the treatment prognosis 2,3,5,13,19.
Maxillary molars are teeth presenting a great number of anomalies regarding to internal anatomy and, therefore, root canals. Most of the studies on maxillary molar anatomy evaluate first molars and their mesial-buccal roots, which may contain two canals (MB-1 and MB-2) 8,9,14,18. MB-1 and MB-2 canals may end totally separated or together within one foramen. Few studies report maxillary second molars. Some report the presence of two palatal canals, other four roots with two separated palatal roots 7,11,17. Slowey 16 was the first author to report the endodontic treatment in a maxillary second molar with two independent palatal roots. Stone and Stroner 17 examined more than 500 extracted maxillary molars and found an incidence below 2% of the presence of more than one palatal canal in these teeth. Von Weiland and Wendt 20 described a clinical case of persistent pain which was only solved after the location and treatment of an extra canal in the palatal root. The same occurred with De Almeida-Gomes et al. 5 who observed during the endodontic retreatment of a maxillary second molar the presence of a second opening orifice close to the previously found palatal canal. Libfeld and Rotstein 10 conducted a radiograph study with approximately 1,200 teeth and reported that the incidence of maxillary second molars presenting four roots were only 0.4% of the cases. According to the studies of Christie et al. 3 , the frequency of two palatal canals were higher than that commonly reported, and therefore they mentioned the importance of a careful analysis of the pulp chamber at the moment of endodontic access. Despite of the low incidence of two palatal canals, Pasternak Júnior et al. 13 presented a more uncommon case: a maxillary second molar with three palatal canals.
Hartwell and Bellizzi 9 evaluated 176 maxillary second molars and found that only 9.6% with two palatal canals, however they did not reported the incidence of a fourth root in this tooth.
Peikoff et al. 14 analyzed 520 second molars and found that only 1.4% of the cases showed four roots of which two were palatal roots.
The aim of this study was to report the endodontic treatment of a maxillary second molar with four roots and two separated palatal canals.
Case report
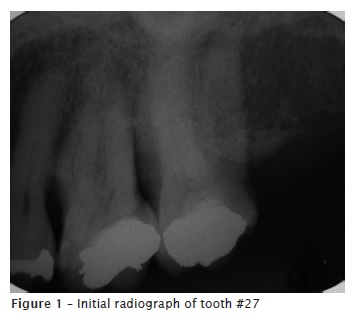
Patient M.S.G., 42 years-old, male, leucoderm, presenting good health, sought for treatment with chief complaint of pain in the upper left region of the face, which had started few days ago. On clinical evaluation, we observed that the tooth #27 showed a large restoration with marginal leakage. Pulp vitality test was performed and the tooth responded positively, which was suggestive of irreversible pulpitis. On radiographic examination, a large restoration with an extensive caries lesion at distal surface was seen, which possibly accounted for the inflammatory process together with the pain reported by the patient (figure 1).
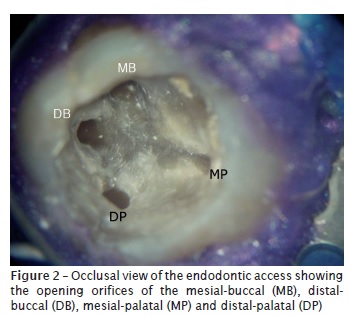
Therefore, patient undergone local anesthesia with 4% articaine with epinephrine 1:100.000 (Articaíne DFL, Indústria e Comércio Ltda., Rio de Janeiro – RJ, Brazil), to be submitted to the endodontic access. After absolute isolation, with the aid of a dental operating microscope (Alliance, São Paulo, Brazil) the endodontic access was refined and the main canals were found. At 16X magnification, mesial-buccal-palatal canal (MB-2) was attempted to be negotiated by small size files. This fourth canal which is mostly seen close to the mesio-buccal canal was not observed; however, a small blood spot was observed very closer to and towards the palatal canal previously located. Accordingly, through TRA-24 ultrasound (Dental Trinks, São Paulo, Brazil), a controlled wearing was performed in this area where a second opening orifice was found at the palatal area (figure 2). At that first moment, this extra canal seemed to be independent of the palatal canal.
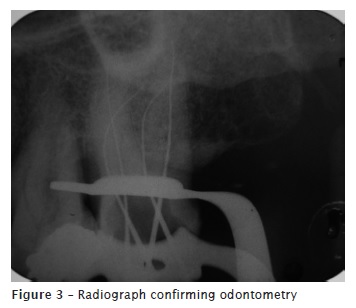
Root canals were prepared by nickel-titanium rotary files (ProTaper system, Dentsply/Maillefer, Ballaigues, Switzerland), through crown-down technique, with 5% sodium hypochlorite irrigation (Fórmula & Ação, São Paulo, Brazil) at every file change. Cervical and medium thirds of the four canals were cleaned and shaped, and next, odontometry was performed with the aid of an electronic apex locator (Mini Root ZX, J. Morita, Tokyo, Japan). A radiograph was taken not only to confirm the working lengths obtained in odontometry, but also to observe the path of the palatal canals. This radiograph revealed two independent palatal roots, and consequently, two separated palatal canals which had not been previously seen (figure 3).
The instrumentation of all root canals was concluded and foraminal patency was executed. Prior to the obturation procedures, 17% EDTA solution (Fórmula & Ação, São Paulo, Brazil) was agitated for 3 minutes with ultrasound device within canals and a new irrigation with hypochlorite carried out to remove EDTA. Canals were irrigated with saline solution and properly dried with Capilary Tips (Ultradent, USA) and paper points (Dentsply/Maillefer, Ballaigues, Switzerland) at sizes compatible with those of root canals.
Obturation was performed following the principles of continuous wave technique, with Pulp Canal Sealer® (Pulp Canal Sealer EWT®, Kerr France, Paris, France).
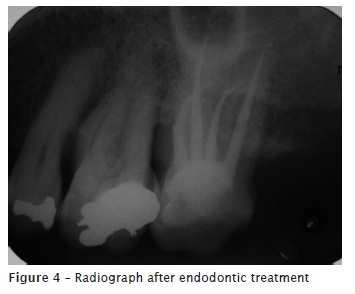
Then, the tooth was sealed with Cimpat (Còlthene/Whaledent, USA) and composite resin (P60; 3M Dental Products, St Paul, USA); a final radiographic shot was carried out (figure 4). After 24 h, patient did not report any simptomatology.
Discussion
The knowledge and domain on the internal anatomy are of extremely important for the clinician intending to execute endodontic treatments, because this can directly influence the success of the cases. All canals, comprising the regular and the extra ones, should be properly localized, accessed, cleaned and shaped to receive the most hermetic obturation as possible for all root canal extension up to the foramen 13,14. Therefore, the ability in locating the canals together with the visual magnification provided by operating microscopy colaborated with a favorable prognosis of the endodontic treatment success 1,7.
Maxillary molars are teeth displaying a great possibility of anatomical variation, not only of the number of canals, but also of their configuration 12,18,19. The variation most cited in literature is the large incidence of a second canal in mesial-buccal root (MB-2), even if MB-2 does not enable total instrumentation. On the other hand, the occurrence of two palatal canals is very rare 10,11,13.
The careful observation of the pulp chamber floor of these teeth at the moment of the endodontic access is mandatory to the identification of possible extra canals 20. Therefore, this step and the following ones must be executed with extremely cautious.
Literature reports a small possibility that maxillary second molars present two palatal canals and four independent roots 6,20,21.
The radiograph of the maxillas the molar area make difficult to determine the configuration of this tooth, mainly the number of palatal roots; notwithstanding, the initial anatomical interpretation of these teeth undergoing endodontic therapy is very important 7,17.
The clinical case reported here showed a maxillary second molar with medium curvature of the buccal roots. All root canals were instrumented with nickel-titanium rotary instruments. Rotary instruments have been well indicated for these situations because of their property of flexibility and maintenance of the root canal center as well as good shaping, even in cases of root dilaceration, diminishing the risk of elbows and perforations 15.
When possible to be observed, a variation in tooth crown morphology may reveal an unusual internal anatomy which should be taken into account 4,7,8.
Conclusion
A careful examination of the pulp chamber is mandatory to detect the opening orifices of extra canals. Therefore, the knowledge of root canal anatomy and its variations together with visual magnification through operating microscope may facilitate the endodontic treatment of these cases.
References
1. Aggarwal V, Singla M, Logani A, Shah N. Endodontic management of a maxillary first molar with two palatal canals with the aid of spiral computed tomography: a case report. J Endod. 2009;35(1):137-9. [ Links ]
2. Baratto-Filho F, Fariniuk LF, Ferreira EL, Pecora JD, Cruz-Filho AM, Sousa-Neto MD. Clinical and macroscopic study of maxillary molars with two palatal roots. Int Endod J. 2002;35(9):796-801.
3. Christie WH, Peikoff MD, Fogel HM. Maxillary molars with two palatal roots: a retrospective clinical study. J Endod. 1991;17(2):80-4.
4. Cunha RS, Davini F, Fontana CE, Miguita KB, Bueno CES. O conceito microsonics: primeiro molar superior com cinco canais – relato de caso. RSBO. 2011 Apr-Jun;8(2):231-5.
5. De Almeida-Gomes F, Maniglia-Ferreira C, dos Santos RA. Two palatal root canals in a maxillary second molar. Aust Endod J. 2007 Aug;33(2):82-3.
6. Deveaux E. Maxillary second molar with two palatal roots. J Endod. 1999;25(8):571-3.
7. Fahid A, Taintor JF. Maxillary second molar with three buccal roots. J Endod. 1988;14(4):181-3.
8. Feix LM, Boijink D, Ferreira R, Wagner RH, Barletta FB. Microscópio operatório na Endodontia: magnificação visual e luminosidade. RSBO. 2010 Sep;7(3):340-8.
9. Hartwell G, Bellizzi R. Clinical investigation of in vivo endodontically treated mandibular and maxillary molars. J Endod. 1982;8(12):555-7.
10. Libfeld H, Rotstein I. Incidence of four-rooted maxillary second molars: literature review and radiographic survey of 1,200 teeth. J Endod. 1989;15(13):129-31.
11. Malagnino V, Gallottini L, Passariello P. Some unusual clinical cases on root anatomy of permanent maxillary molars. J Endod. 1997;23(2):127-8.
12. Paganini GA, Tróia Júnior MG, Oliveira P, Valdrighi HC, Tarrafa VF. Taurodontismo. RGO. 2005;53(2):117-9.
13. Pasternak Júnior B, Teixeira CS, Silva RG, Vansan LP, Sousa Neto MD. Treatment of a second maxillary molar with a six canals. Aust Endod J. 2007 Apr;33(1):42-5.
14. Peikoff MD, Christie WH, Fogel HM. The maxillary second molar: variations in the number of roots and canals. Int Endod J. 1996 Nov;29(6):365-9.
15. Santos KSA, Saraiva e Silva L, Gomes FB, Santos RA. Preparo dos canais com instrumentos rotatórios: sistema Protaper, Pow-R e Profile – avaliação da forma de canais radiculares pós-preparo. RGO. 2004;52(1):52-4.
16. Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg. 1974;37(5):762-72.
17. Stone LH, Stroner WF. Maxillary molars demonstrating more than one palatal root canal. Oral Surg. 1981;51(6):649-52.
18. Thompson BH. Endodontic therapy of an unusual maxillary second molar. J Endod. 1988;14(3):143-6.
19. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984;58(5):589-99.
20. Von Weiland M, Wendt A. Akute retrograde Pulpitis bei veirwurzeligem Molar. Stomatol DDR. 1988;38(11):784-5.
21. Wong M. Maxillary first molar with three palatal canals. J Endod. 1991;17(6):298-9.
 Correspondence:
Correspondence:
Carlos Eduardo Fontana
Avenida 02, n.º 1.220
CEP 13500-411 – Rio Claro – SP – Brasil
E-mail:ceffontana@hotmail.com
Received for publication: October 10, 2011.
Accepted for publication: November 11, 2011.
