










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Original Research Article
Analysis of the instrumentation time and cleaning between manual and rotary techniques in deciduous molars
Sérgio Luiz Pinheiro I; Leniana Santos Neves II; José Carlos Pettorossi Imparato II,III ; Danilo Antônio Duarte IV; Carlos Eduardo da Silveira Bueno V; Rodrigo Sanches Cunha VI
II Department of Pediatric Dentistry, São Leopoldo Mandic School of Dentistry – Campinas – SP – Brazil.
III Department of Pediatric Dentistry, School of Dentistry of University of São Paulo – São Paulo – SP – Brazil.
IV Department of Pediatric Dentistry, School of Dentistry of University of Cruzeiro do Sul – São Paulo – SP – Brazil.
V Department of Endodontics, São Leopoldo Mandic School of Dentistry – Campinas – SP – Brazil.
VI Department of Restorative Dentistry, University of Manitoba – MB – Canada.
ABSTRACT
Introduction: The rotary instrumentation provides shorter instrumentation time with greater comfort for the patient but few studies have been conducted on primary teeth. Objective: his study compared the cleaning ability and instrumentation time between manual and rotary techniques in deciduous molars. Material and methods: a total of 15 molars were selected, submitted to coronal opening and root canal filled with India ink. After 48 hours, the teeth were divided into three groups: G1 – manual instrumentation with K files, G2 – rotary system Endowave, and G3 – rotary system ProTaper. After instrumentation, the teeth were sectioned and three blinded examiners evaluated the root canal cleaning. The mode of scores of examiners was analyzed by the Kruskal-Wallis test. The instrumentation time was recorded and the results were statistically analyzed by ANOVA.Results: the ProTaper system presented shorter instrumentation time compared to manual instrumentation (p = 0.0339). Endowave system did not present statistically significant difference in the instrumentation time compared to the other groups. There were no significant differences between groups concerning the ability of root canal cleaning (p = 0.6188). Conclusion: ProTaper system revealed shorter treatment time and similar cleaning ability compared to the other techniques, thus being indicated for deciduous teeth.
Keywords: Endodontics; instrumentation; tooth; deciduous.
Introduction
The success of endodontic therapy is directly related to the microbial reduction in the root canal system, shaping 2,12,17,23,24,26 and sealing 17,23. Even though manual instrumentation is used for that purpose in deciduous teeth, it presents some limitations concerning root canal cleaning, anatomical fidelity and chair time 3,18,26.
Rotary instrumentation using motor-driven nickel-titanium files (Ni-Ti) is an easy technique that requires a smaller number of instruments 2. Its greater cutting efficacy in dentin reduces the stresses on the files 3, which present variable tapers to allow better cleaning, apical control and obturation. Additionally, their similarity with the root canal morphology allows simple and effective preparation, thereby reducing the occurrence of iatrogenia 7. The Ni-Ti rotary instruments are able to maintain the original root canal shape without creating severe irregularities as zipping, steps and perforations, especially in narrow curved canals 14,28.
The mechanical preparation of deciduous teeth using Ni-Ti rotary files was initially described by Barr 5 who observed effective root canal cleaning in deciduous teeth in a shorter instrumentation time. Among the main advantages of the technique, the authors reported easier cleaning, flexibility of nickel-titanium files, access to the root canal and easy obturation. The disadvantages include the cost of the handpiece and nickel-titanium files and need of training on the technique 5. According to Nagaratna et al. 18, the time required for rotary instrumentation using nickel-titanium files for root canal preparation in deciduous teeth is shorter compared to manual stainless steel Kerr files. When compared to the permanent dentition, the rotary instrumentation is faster in deciduous teeth, probably due to the smaller root canal length. Also, the rotary technique facilitates the application of the obturation paste and minimizes the extrusion of material 5,26.
The rotary instrumentation in permanent teeth also provides reduced chair time, greater comfort for the patient and lower risk compared to the manual instrumentation 2,3,18,19,32. Since this is a recent technique and few studies have been conducted on deciduous teeth 3, this study compared the root canal cleaning ability and instrumentation time from rotary techniques in deciduous molars using the manual technique as a control group.
Methods
This study was revised and approved by the Institutional Review Board of São Leopoldo Mandic Dental School (protocol n. 2009/0056).
The study was conducted on 15 deciduous molars (7 maxillary and 8 mandibular molars) obtained from the Human Teeth Bank of São Leopoldo Mandic Dental School. These teeth were extracted, cleaned and stored in 0.1% thymol solution up to 2 weeks after extraction. The teeth were radiographed using the E-Speed film (Kodak Company – Rochester, NY, USA) and an X-ray device (Astex Equipamentos Radiológicos Ltda., São Paulo, SP, Brazil) with exposure time of 0.75 seconds. The films were manually processed in a portable darkroom (VH Midas Dental Products Ltda., Araraquara, SP, Brazil), being developed (developer: Kodak Company – Rochester, NY, USA) at a temperature of 25ºC for 2 minutes, rinsed in water for 30 seconds, and fixed (fixer: Kodak Company – Rochester, NY, USA) for 3 minutes. After this process, the films were rinsed in tap water for 30 seconds.
The inclusion criteria comprised maximum exfoliation of half of the roots; no trepanation in the furcation area; no root fractures; no pulp nodules or calcifications; root curvature between 20 and 30 degrees according to the method of Schneider 25.
Coronal opening was performed using round diamond burs n. #1013 (Kg Sorensen, Barueri, São Paulo, Brazil) at high speed (Silnet, Dabi Atlante, Ribeirão Preto, SP, Brazil) under air/water cooling, complemented with Endo Z burs (Kg Sorensen, Barueri, São Paulo, Brazil) compatible with the size of the pulp chamber.
The working length was determined by passive insertion of a K file n. #10 in each root canal (Maillefer Instruments, Ballaigues, Switzerland) with a rubber stop. When the file tip was at the level of the apical foramen, the rubber stop was levelled with the respective cusp tip and the length of each root canal was recorded. The working length was obtained by subtracting one millimetre from the total length of the root canals.
The root canals were then dried with suction cannulas (BD – Becton Dickinson Ind. Cirúrgicas Ltda., Rio de Janeiro, RJ, Brazil) and absorbent paper points (Dentsply Indústria e Comércio Ltda., Petrópolis, RJ, Brazil). India ink (Acrilex, Tinta China INK, São Bernardo do Campo, SP, Brazil), previously stored in anaesthetic tubes, was then placed into the root canals using a carpule syringe (Duflex – S.S.White Artigos Dentários Ltda., Rio de Janeiro, RJ, Brazil) and an anaesthetic needle (BD – Becton Dickinson Ind. Cirúrgicas Ltda., Rio de Janeiro, RJ, Brazil). After 48 hours, the teeth were divided into three groups (n = 15 teeth, total of 41 root canals) (table I):
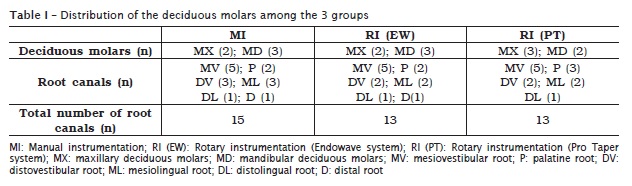
Group 1 (G1) (n = 15 root canals, control group) – manual instrumentation: the root canals were manually prepared using K files (Maillefer Instruments, Ballaigues, Switzerland): a) coronal opening; b) irrigation (performed throughout the preparation); c) location of root canals; d) root canal preparation using K files: utilization of initial instrument (better fit in the root canal) and two sequential instruments. The cleaning process was finalized when no turbidity was observed in the irrigant solution after utilization of the last instrument; e) after irrigation, the root canal was dried by suction using an aspirator and large hypodermic needles, complemented with absorbent paper points.
Group 2 (G2) (n = 13 root canals) – rotary instrumentation: the root canals were prepared using rotary instruments Endowave (Morita, Dietzenbach, Germany), at a speed of 300 rpm and torque of 3 N/cm. First series files were used in increasing order of diameter: 15 (white), 20 (yellow), 25 (red) and 30 (blue) with an anticurvature filing method 17.
Group 3 (G3) (n = 13 root canals) – rotary instrumentation: the root canals were prepared using rotary instruments ProTaper (Dentsply Ltd., Addlestone, Weybridge, UK), using a handpiece and an electric motor X-Smart (Dentsply Ltd., Addlestone, Weybridge, UK), at a speed of 300 rpm and torque of 3N/cm (S1 and S2) and 2N/cm (F1 and F2) with an anticurvature filing method 1.
The root canals were irrigated throughout with 3 ml of saline at each change of instrument (ADV – Tayuyna, Nova Odessa, SP, Brazil) using a Luer Lock syringe (Duflex – S.S. White Artigos Dentários Ltda., Rio de Janeiro, RJ, Brazil). The instrumentation time for each specimen was measured with a digital chronometer (Oregon Scientific, Portland, USA).
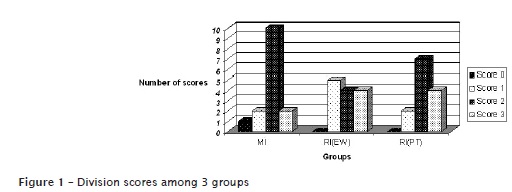
After completion of instrumentation, the teeth were initially transversely sectioned to separate the crown from the roots. Longitudinal sections were then made in buccolingual directions for achievement of two hemisections of each root canal, which were fixated on a paper leaf (Chamex, Luiz Antônio, SP, Brazil) using adhesive tape (Fortkol Indústria de Fitas Adesivas Ltda., Pouso Alegre, MG, Brazil), with the root canal wall turned upward. Then, the specimens were photographed with a digital camera (Sony Cyber-Shot DSC-S730, 7.2 mega pixels – China) at a distance of 30 cm from the specimen, at 3x magnification. The images were analyzed by three blinded examiners according to the following scores 4: 0 – total cleaning; 1 – almost complete dye removal; 2 – partial dye removal; and 3 – no dye removal.
The root canal cleaning was evaluated by scores assigned to the two hemisections of each tooth, which were added up. The mode of scores of the three examiners was analyzed by the Kruskal-Wallis test. The recorded instrumentation time was analyzed by the ANOVA and then by the post-hoc Tukey test. The statistical tests were conducted using the software BioEstat 3.0 (Belém, PA, Brazil, 2003).
Results
Comparison of the root canal cleaning of deciduous molars did not reveal statistically significant difference between groups (p = 0.6188) (table II, figure 1).
Concerning the mean instrumentation time, the Pro Taper system, presented the shorter time, with statistically significant difference compared to manual instrumentation (p = 0.0339). The Endowave system did not present statistically significant difference in the instrumentation time compared to the other groups (table III).


Discussion
The biomechanical root canal preparation is fundamental for endodontic therapy because it allows the removal of vital tissue, necrotic remnants, infected dentin and debris, providing ideal conditions for tissue repair and regeneration 3,17. Scientific evidences have shown that root canal cleaning before obturation is related to high success rates in pulp therapy 2.
The rotary system has been recently introduced for endodontic preparation of deciduous teeth, thus few studies are available on the efficacy of this method 3,27. However, the same principles of root canal cleaning and shaping using rotary instruments in permanent teeth are also followed for deciduous teeth 7. Knowledge on this fact is important because, considering the lack of studies analyzing the preparation and mechanical cleaning of root canals of deciduous molars, the present results will often be compared to studies on permanent teeth.
The present methodology employed an increasing sequence of first series rotary instruments to allow anatomical compatibility between the instrument and the root canal of deciduous molars. No specific operative sequence has been presented in the literature for deciduous teeth, therefore the protocols for permanent teeth are adapted for this purpose. In order to compare the two types of rotary systems (Endowave and ProTaper), four instruments of each manufacturer were used. Saline was applied for irrigation to avoid a possible interaction between the irrigant and the dye, thereby not interfering with the effect of biomechanical preparation on root canal cleaning.
In a previous study, Tan and Messer 29 observed that both the manual and rotary techniques do not allow complete root canal cleaning in permanent teeth. This was also observed in the present study, by the observation of remaining dye on the root canal walls and the mean scores found for the three groups, indicating that no group presented score 0 and therefore no instrumentation technique presented complete cleaning ability. The authors 29 further concluded that the wider apical preparation allows better cleaning of the root canal system, which was confirmed in later studies 2,3.
According to the present results, comparison of the cleaning ability between the manual and rotary instrumentation techniques (Endowave and Pro Taper) did not present statistically significant differences. The literature unanimously states that manual and rotary instrumentation techniques present similar cleaning ability. Thus, previous studies corroborate these results for deciduous molars 26, anterior deciduous teeth 3 and permanent molars 21.
The chair time should also be considered in the endodontic therapy, especially in Paediatric Dentistry. Within this context, several devices and techniques have been developed to make the treatment easier and more effective 20,30.
Comparison of the instrumentation time between the three groups revealed that manual instrumentation presented longer time in relation to the other groups, with significant difference compared to the ProTaper system. This tendency of longer time when manual instruments are used is widely reported in the literature 2,3,9,20-22,26,27,30. The shorter time required in the rotary instrumentation is probably related to the reduced number of instruments 2,28 and greater efficacy of dentin cutting 3, reducing the patient fatigue 18.
In the present study, the difference in the instrumentation time between group 1 (manual instrumentation) and group 2 (Endowave) was not statistically significant. This probably occurred because of the small sample size. Statistical comparison between larger groups would probably reveal this difference. The difficulty to achieve deciduous molars according to the present inclusion criteria led to the small sample size. This increasing difficulty was also observed in previous studies, conducted on even smaller 17,26 or slightly larger samples 30. Despite the limited sample size, it was observed that the rotary instruments tended to present shorter instrumentation time compared to the manual instruments.
The endodontic treatment in children may be challenging and time consuming, especially during root canal preparation, which is one of the most important stages of endodontic therapy. Considering that the rotary instruments provide similar root canal cleaning compared to manual instruments with a shorter instrumentation time, their utilization is well indicated in Paediatric Dentistry, especially when treating children with behaviour management disorders 13,15.
The root canal walls and canals of deciduous molars are usually curved and irregular and may be cleaned with Ni-Ti rotary instruments, similar to the manual instruments 5. However, the former are advantageous due to their flexibility 18,30,31, which allows easy access to all root canals 4, in addition to their cutting efficacy and treatment time 10,11,16, maintaining the original root canal shape, reducing the tendency of apical flaring 4 and enhancing consistent and dense root canal filling 4.
However, the rotary instrumentation also presents disadvantages or limitations related to the high cost of the equipment and Ni-Ti files 6,17, risk of fracture 21,30 and need of operator training 18,19,26.
Considering the benefits and costs of the rotary root canal instrumentation, it may be indicated for utilization in deciduous teeth, enhancing root canal preparation with a shorter treatment time. This increases the comfort for the patient and improves the working conditions for the professional. Notwithstanding, this is a recent technique and further studies are necessary to demonstrate its efficacy, especially in paediatric dentistry.
Conclusion
The ProTaper system was more effective for root canal instrumentation in deciduous molars, presenting shorter treatment time and similar cleaning ability compared to the other techniques.
References
1. Abou-Rass M, Frank AL, Glick DH. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980;101:792-4. [ Links ]
2. Baugh D, Wallace J. The role of apical instrumentation in root canal treatment: a review of the literature. J Endod. 2005;31:333-40.
3. Bahrololoomi Z, Tabrizizadeh M, Salmani L. In vitro comparison of instrumentation time and cleaning capacity between rotary and manual preparation techniques in primary anterior teeth. J Dent Tehran University of Medical Sciences. 2007;4:59-62.
4. Barr B, Barr N. Posterior pulpectomies: using rotary files. Childrens Dentistry, A Partnership. 1999;6:1-3.
5. Barr ES, Kleier DJ, Barr NV. Use of nickel-titanium rotary files for root canal preparation in primary teeth. Pediatr Dent. 1999;21:453-4.
6. Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of manual preflaring and torque on the failure rate of ProTaper rotary instruments. J Endod. 2004;30:228-30.
7. Buchanan LS. The standardized-taper root canal preparation – part 1. Concepts for variably tapered shaping instruments. Int Endod J. 2000;33:516-29.
8. Cerqueira DF, Mello-Moura AC, Santos EM, Guedes-Pinto AC. Cytotoxicity, histopathological, microbiological and clinical aspects of an endodontic iodoform-based paste used in pediatric dentistry: a review. J Clin Pediatr Dent. 2008;32:105-10.
9. Correia SV, Nogueira M, Silva R, Lopes LP, Fernandes FMB. Phase transformations in NiTi endodontic files and fatigue resistance. ESOMAT 2009. Available from: http://www.esomat.org or http://dx.doi.org/10.1051/esomat/200907004.
10. Crespo S, Cortes O, Garcia C, Perez L. Comparison between rotary and manual instrumentation in primary teeth. J Clin Pediatr Dent. 2008;32:295-8.
11. Ferraz CC, Gomes NV, Gomes BP, Zaia AA, Teixeira FB, Souza-Filho FJ. Apical extrusion of debris and irrigants using two hand and three engine-driven instrumentation techniques. Int Endod J. 2001;34:354-8.
12. Grossman L. Endodontic practice. 10. ed. Philadelphia: Lea & Febiger; 1981.
13. Guelzow A, Stamm O, Martus P, Kielbassa AM. Comparative study of six rotary nickel-titanium systems and hand instrumentation for root canal preparation. Int Endod J. 2005;38:743-52.
14. Haga CS. Microscopic measurements of root canal preparations following instrumentation. J Br Endod Soc. 1968;2:41-6.
15. Hulsmann M, Herbst U, Schafers F. Comparative study of root-canal preparation using Lightspeed and Quantec SC rotary NiTi instruments. Int Endod J. 2003;36:748-56.
16. Kummer TR, Calvo MC, Cordeiro MM, de Sousa Vieira R, de Carvalho Rocha MJ. Ex vivo study of manual and rotary instrumentation techniques in human primary teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:e84-92.
17. Marchesan MA, Arruda MP, Silva-Sousa YTC, Saquy PC, Pecora JD, Sousa-Neto MD. Morphometrical analysis of cleaning capacity using nickel-titanium rotary instrumentation associated with irrigating solutions in mesio-distal flattened root canals. J Appl Oral Sci. 2003;11:55-9.
18. Nagaratna PJ, Shashikiran ND, Subbareddy VV. In vitro comparison of NiTi rotary instruments and stainless steel hand instruments in root canal preparations of primary and permanent molar. J Indian Soc Pedod Prev Dent. 2006;24:186-91.
19. Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod. 2004;30:559-67.
20. Pinheiro SL, Bincelli IN, Faria T, Bueno CES, Cunha RS. Comparison between electronic and radiographic method for the determination of root canal length in primary teeth. RSBO. 2012;9:11-6.
21. Rodig T, Hulsmann M, Kahlmeier C. Comparison of root canal preparation with two rotary NiTi instruments: ProFile .04 and GT Rotary. Int Endod J. 2007;40:553-62.
22. Schafer E, Florek H. Efficiency of rotary nickel-titanium K3 instruments compared with stainless steel hand K-Flexofile. Part 1. Shaping ability in simulated curved canals. Int Endod J. 2003;36:199-207.
23. Schafer E, Schulz-Bongert U, Tulus G. Comparison of hand stainless steel and nickel titanium rotary instrumentation: a clinical study. J Endod. 2004;30:432-5.
24. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am. 1974;18:269-96.
25. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971;32:271-5.
26. Silva LA, Leonardo MR, Nelson-Filho P, Tanomaru JM. Comparison of rotary and manual instrumentation techniques on cleaning capacity and instrumentation time in deciduous molars. J Dent Child. 2004;71:45-7.
27. Sonntag D, Delschen S, Stachniss V. Root-canal shaping with manual and rotary Ni-Ti files performed by students. Int Endod J. 2003;36:715-23.
28. Spangberg L. The wonderful world of rotary root canal preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:479.
29. Tan BT, Messer HH. The quality of apical canal preparation using hand and rotary instruments with specific criteria for enlargement based on initial apical file size. J Endod. 2002;28:658-64.
30. Tasdemir T, Aydemir H, Inan U, Unal O. Canal preparation with Hero 642 rotary Ni-Ti instruments compared with stainless steel hand K-file assessed using computed tomography. Int Endod J. 2005;38:402-8.
31. Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod. 1988;14:346-51.
32. Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J. 2008;41:339-44.
 Correspondence:
Correspondence:
Rodrigo Sanches Cunha
D226C – 780 Bannatyne Avenue
Winnipeg, Manitoba – Canada
E-mail:cunhars@cc.umanitoba.ca
Received for publication: February 14, 2012.
Accepted for publication: March 03, 2012.
