










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Original Research Article
Filling of simulated lateral canals using different obturation techniques: analysis through IDA digital radiograph system
Clarissa Teles Rodrigues I; Renata Pardini Hussne II; Celso Kenji Nishiyama II; Fernanda Gomes de Moraes I
II Hospital for the Rehabilitation of the Craniofacial Anomalies, University de São Paulo – Bauru – SP – Brazil.
ABSTRACT
Introduction: Lateral canals are part of the rootcanal system and may be relatedto periodontal-endodontic diseases. The filling techniques that employ thermoplasticized gutta-percha have demonstrated better results in filling lateral canals. Objective: The aim of this study was to evaluate, through digital radiographs, three techniques of root canal obturation (Lateral Condensation, Obtura II System, Taggers Hybrid) regarding to the ability of filling artificial lateral canals. Material and methods: 30 extracted human lower premolars were used in this study. The crowns were removed and artificial laterals canals were prepared on the coronal, medium and apical thirds of the roots by using a reamer made of a K 10 file. The root canals were instrumented and obturated by the following techniques: Lateral Condensation, Obtura II System, and Taggers Hybrid. The teeth were radiographed with IDA digital radiograph system and the filling of the lateral canals was evaluated by scores for further statistical analysis. Results: No significant difference was found in the filling of lateral canals between Lateral Condensation and Obtura II, but a significant difference was found among these two and Taggers Hybrid technique. Conclusion: Taggers Hybrid technique promoted the highest numbers of obturated lateral canals. In the three groups, the root thirds presenting greater number of filled lateral canals were coronal and middle, regardless of the obturation technique employed.
Keywords: Endodontics; gutta-percha; root canal obturation.
Introduction
The deep knowledge on pulp cavity morphology is very worthy for the execution of the endodontic treatment 19. Lateral canals are part of root canal system within the teeth 23. They come from the main root canal towards the periodontal ligament and frequently are located perpendicularly to the main canal, with a slight inclination towards the apex 1,14,15. These canals were observed by De Deus (1975) 1 in 27.4% of the teeth studied and they were located more frequently at the apical region.
The presence of lateral canals is not always noticed, but some of them may be detected in radiographs if they are more thickened 27. Lateral canals play a fundamental role in the endodontic treatment because they may contain remnants of infected or necrotic pulp tissue and bacterias 27. Moreover, since they communicate with the periodontium, they are important in periodontal-endodontic problems 1. Such necrotic remnants and bacterias are difficult to remove by only using conventional endodontic instrumentation, and therefore, the tridimensional filling of the root canal is particularly important 10,22.
The obturation techniques employing thermoplastification were introduced to improve the homogeneity and adaptation of gutta-percha on tooth surface 26. The current researches have reported that techniques using thermoplasticized gutta-percha demonstrated the best results in the filling of lateral canals and apical ramifications when compared to lateral condensation technique 3,8,20.
Cold lateral condensation of gutta-percha has been the most used filling technique in Endodontics, because of its ease and simple handling, efficiency, and ability of controlling the obturation extension 4,9. However, this technique demands a longer chair time, presents an inhomogeneous filling mass with poor adaptation to the canal walls and irregularities, and not even fills the accessory canals 2,13.
Among some of gutta-percha thermoplastification techniques, it can be cited Obtura II system, which comprises a device similar to pistol that enables the introduction of the thermoplasticized gutta-percha into root canal through silver needles of different diameters. The injectable thermoplastification technique has as advantages: effective apical sealing, ease handling, small number of steps, and smaller chair time. Notwithstanding, the greatest disadvantage of this technique is the high temperature (160°C) required for the proper fluidity of gutta-percha 11,28.
Other technique is Taggers Hybrid, in which the gutta-percha is thermoplasticized and compacted into root canal through motor-driven compactors. McSpadden, in 1978, idealized a technique for root canal filling so-called thermo-mechanical condensation of gutta-percha, in which a compactor similar to an inverted Hedströem instrument was mechanically driven into root canal generating heat by attrition between the instrument and gutta-percha, resulting in its plasticization and compactation towards apical and lateral direction 14,15. The advantages of this technique are: reduction in obturation time and operators fatigue, greater filling of the canal irregularities and greater capacity of the filling of root canal system by gutta-percha 12,16. Aiming to minimize the adverse effects of the technique originally proposed by McSpadden such as the high incidence of overfilling, Tagger, in 1984, proposed the hybrid obturation technique in which cold lateral compactation of gutta-percha is performed in the apical third associated with the thermo-mechanical compactation in the 2/3 coronal thirds of the canal 15.
In Endodontics, one of the methods to verify the quality of root canal obturation is the periapical radiograph 5,6. The digital radiograph is an advancement in image diagnosis because it incorporates informatics technology in the capturing, interpretation, and archiving of radiographic examinations 18. Additionally, it discards the use of the conventional film, generating smaller amount of toxic residues to the environment because these films are composed of silver, need the lead plate, and still employ chemical solutions for their processing 7. The Advanced Digital Image System (IDA) is composed of a intraoral sensor which captures the image through the radiation emission by the x-ray device. The Docking Station transmits the image to the computer through a USB cable, and the image is instantly exhibited on the computer screen. With the aid of Pro Image software, this image can be manipulated to adjust its brightness and contrast and to use reverse contrast (positive/negative), zoom and color of specific areas (color representation of the radiograph).
The aim of this study was to compare through digital radiographs (IDA system) the ability of lateral condensation, Obtura II and Taggers Hybrid techniques in filling lateral canals artificially created in roots of extracted human teeth.
Material and methods
This study was approved by the Ethical Committee in Research of HRAC/USP, under protocol # 48/2011-SVAPEPE-CEP.
Thirty single-rooted extracted human lower premolars were used in this study. Firstly, they had their crowns removed to standardize the length of the roots from 14 to 17 millimeters.
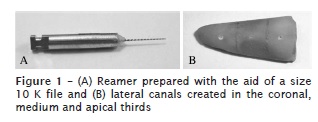
The lateral canals were created with the aid of reamer made of cutting 2.5 mm of the active point of a size 10 K file (Maillefer, Ballaigues, Switzerland). Next, this instrument was inserted in a high-speed bur adapter with the aid of chemically-cured acrylic resin leaving 5 mm of the instruments tip free to enable that the instrument be used as a rotary instrument (figure 1A).
By using this reamer, three perforations were made on one of the proximal surfaces of each root, perpendicularly to the main root canal axis, therefore obtaining the artificial lateral canals, strategically located in the apical, medium and coronal thirds (figure 1B).
Odontometry was accomplished by inserting a size 10 K file into root canal until its tip was observed in the apical foramen. After the adjustment of a marker on the dentinal wall adjacent to the root canal opening, the instrument was removed and the distance between the tip and the marker was measured. Working length was set at 1 mm short of this measurement.
The canals were firstly instrumented by size 2 to 5 Gates-Glidden burs (Maillefer, Ballaigues, Switzerland) in the medium and coronal thirds. In apical third, instrumentation was accomplished by hand K instrument, through crown-down technique. Memory instrument was a size 40 file. After the construction of the apical stop, instrumentation was progressed toward coronal third by increasing the size every 1 mm, up to size 60 instrument.
A copious irrigation was performed with 1% sodium hypochlorite (Myaco do Brazil Ind. e Com.), with the aid of a 5 cc Luer Look syringe and 27-Gauge cannula. After instrumentation, EDTA (Biodinâmica, Ibiporã, PR, Brazil) was applied and agitated by using the memory instrument for 3 minutes. Following, the canals were irrigated with saline solution and dried with size 40 absorbent paper points (Dentsply, Petrópolis, RJ, Brazil).
Obturation was accomplished with Endofill (Dentsply, Petrópolis, RJ, Brazil), for all groups, prepared according to the manufacturers instructions. The roots were randomly divided into 3 groups (n = 10), according to the obturation technique to be used.
Group I: active lateral condensation
In this technique, the master gutta-percha cone was taken up to the working length and seated by the controlled biological technique. The master cone was left seated and the accessory cones were introduced into the canal with the aid of a size 30 K file (Maillefer, Ballaigues, Switzerland), which were inserted with the sealer toward the canals wall and then counterclockwisely removed to create room for the next accessory point. This procedure was repeated until the insertion of new accessory cones was not possible. After the obturation completion, the excess of filling material was removed with the aid of a size 2 heated Paivas condenser and the vertical condensation was executed.
Group II: Obtura II system (Obtura Spartan, Fenton, MO, USA), according to the manufacturers instructions
The endodontic sealer was applied onto the root canal's walls with the aid of a size 30 Kerr type instrument. The Obtura handpiece was then inserted into root canal up to the contact of the needle with the root canal's wall. The plasticized gutta-percha was passively injected with the aid of a 23-Gauge needle, into root canal, avoiding pressure on the needle. The needle's tip should reach between 3 and 5 mm short of the working length. After the filling of the apical third, the first condenser was inserted and slow forward and backward condensation movements were executed in the tooth long axis to condense the material in this area. The handpiece was again inserted and the aforementioned steps repeated in the medium and coronal thirds. Three cold Paiva's condensers of different sizes were used to accommodate the soften mass to promote a better adaptation of the gutta-percha to the root canal's walls in each third of the canal.
Group III: Taggers Hybrid technique
Size 40 master gutta-percha cone was involved in endodontic sealer and inserted into root canal by controlled biological technique. With the aid of a size 30 K file, close to the master gutta-percha cone, from two to three accessory points (Dentsply, Petrópolis, RJ, Brazil) were inserted. The excess of the cones were cut. Next, a size 55 McSpadden condenser (Maillefer, Ballaigues, Switzerland) was coupled to a low-speed contra-angle handpiece and introduced passively into root canal. The penetration of the condenser inside root canal was obtained with the aid of a rubber marker 4 mm short of the working length. With the condenser inside the root canal, next to the gutta-percha cones, it was driven by forward and backward movements up to reach working length, staying in that position for about 1 second. The condenser was removed from root canal with the motor still driven with gentle pressure on one side of the canals wall. Following, the vertical condensation of the plasticized gutta-percha was performed through Paivas condensers to obtain a better adaptation to the dentinal wall.
After the obturation of all samples, radiographic shots were performed through IDA – Advanced Digital Image (Dabi Atlante, Ribeirão Preto, SP, Brazil) to assess the filling of the artificial lateral canals.
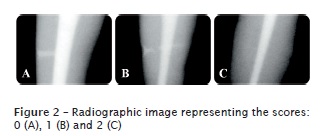
The digital radiographic images were analyzed by three blinded examiners previously calibrated to control the scores regarding to the filling of the lateral canals, three images of the lateral canals were sent to the examiners who should assign scores from 0 to 2:
Score 0 = complete filling (figure 2A);
Score 1 = half filling and/or presence of blisters (figure 2B);
Score 2 = empty lateral canal, without evidences of the penetration of the material (figure 2C).
The data obtained after the assessment of the radiographic images were submitted to statistical analysis by Kappa test, aiming to verify the inter-examiners agreement, and Kruskal-Wallis test, with level of significance of 0.05, to analyze the scores. Kruskal-Wallis was chosen because this is a subjective analysis and it is non-parametric test which compares two or more groups.
Results
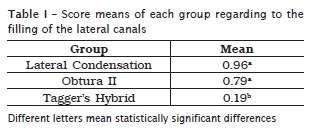
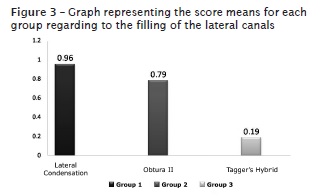
Kappa test value was 0.78, demonstrating a substantial agreement among examiners. Table I shows the means of each group according to the scores assigned to the filling of the lateral canals. There was no statistically significant difference (p > 0.05) between entre lateral condensation and Obtura II groups, but there was a statistically significant difference (p < 0.05) among these groups and Tagger's Hybrid group (figure 3).
Table II displays the score means regarding to the filling of the lateral canals according to thirds for each group.

Concerning to the filling of the lateral canals by third, there was no statistically significant difference (p > 0.05) among groups regarding to the filling of the coronal third. In medium third, there was no statistically significant difference (p > 0.05) between lateral condensation and entre Obtura II groups and between Obtura II and Taggers Hybrid, however, there was a statistically significant difference (p < 0.05) between lateral condensation and Taggers Hybrid groups in the filling of the lateral canals in this third. There was no statistically significant difference (p > 0.05) in the filling of the lateral canals in apical third between lateral condensation and Obtura II groups, however, there was a statistically significant difference (p < 0.05) between lateral condensation and Taggers Hybrid groups and Obtura II and Taggers Hybrid groups.
Discussion
The results found in this study demonstrated the best performance of the techniques employing thermoplasticized gutta-percha in the filling of lateral canals, which is in agreement with previous studies, such as Raymundo et al. 20, DuLac et al. 3, Goldberg et al. 8, Morgental et al. 17, Reader et al. 21.
The filling technique which showed the highest number of lateral canals filled in this study was Taggers Hybrid. The compression exerted by the McSpadden condenser during obturation in this technique results in the impulsion of the material against the canals walls, and consequently, the material is pushed toward the lateral canals.
Obtura II had a smaller performance than Taggers Hybrid group, resulting in few lateral canals filled with gutta-percha. This could have occurred due to the fast cooling of thermoplasticized gutta-percha after its introduction into root canal, as described by Donley et al. 2.
The filling technique which presented the smallest number of lateral canals filled in this study was lateral condensation. In these cases, probably, the lateral canals were filled only by the
endodontic cement instead of gutta-percha, which also occurred in the studies of DuLac et al. 3 and Reader et al. 21.
Concerning to root canals thirds, there was no statistically significant difference among groups in the coronal third, while medium and apical thirds showed significant differences. Goldberg et al. 8 did not found statistically significant difference by comparing the filling of the lateral canals in the different root canals thirds. On the other hand, Venturi et al. 24, by evaluating the natural ramifications, demonstrated that there was a greater difficult in filling the ramifications located at the apical third, because they are narrower and more tortuous than those located close to tooth crown.
The use of digitized radiograph in this study was of great importance, because the image manipulation such as the magnification of the areas containing lateral canals, allowed the best observation of the presence of blisters or failures in the filling mass.
Conclusion
Considering the methodology employed and the results of this study, it can be conclude that:
the technique which best filled the artificial lateral canals was Taggers Hybrid;
there was no statistically significant difference in the filling of lateral canals between lateral condensation and Obtura II system groups;
coronal and medium thirds were the most filled thirds regardless of the technique employed.
Acknowledegments
We thank to J. Morita, especially to Grace Bastianelli, DDS for lending the Obtura II system; to Dabi Atlante, especially to Agnaldo for the availability of the use of the IDA system of digital radiograph; and to Dentsply, especially to Sany Dagmar for the donation of part of the material used in this study.
References
1. De Deus QD. Frequency, location, and direction of lateral, secondary, and accessory canals. J Endod. 1975 Nov;1(11):361-6. [ Links ]
2. Donley DL, Weller RN, Kulild JC, Jurcak JJ. In vitro intracanal temperatures produced by low- and high-temperature thermoplasticized injectable Gutta-percha. J Endod. 1991 Jul;17(7):307-9.
3. DuLac KA, Nielsen CJ, Tomazic TJ, Ferrillo Jr. PJ, Hatton JF. Comparison of the obturation of lateral canals by six techniques. J Endod. 1999 May;25(5):376-80.
4. Estrela C. Ciência endodôntica. São Paulo: Artes Médicas; 2004.
5. Ferraz EG, Fracassi LD, Marques AMC, Albergaria SJ, Sarmento VA. Avaliação da qualidade de duas técnicas de obturação do canal radicular por meio de radiografia digitalizada. RFO. 2009 May-Aug;14(2):126-31.
6. Ferreira HLJ, Paula MVQ, Guimarães SMR. Avaliação radiográfica de obturações de canais radiculares. Rev Odonto Ciênc. 2007 Oct-Dec;22(58):340-5.
7. Fracassi LD, Ferraz EG, Albergaria SJ, Sarmento VA. Comparação radiográfica do preenchimento do canal radicular de dentes obturados por diferentes técnicas endodônticas. RGO. 2010 Apr-Jun;58(2):173-9.
8. Goldberg F, Artaza LP, De Silvio A. Effectiveness of different obturation techniques in the filling of simulated lateral canals. J Endod. 2001 May;27(5):362-4.
9. Gound TG, Riehm RJ, Makkawy HA, Oldgaard EC. A description of an alternative method of lateral condensation and a comparison of the ability to obturate canals using mechanical or traditional lateral condensation. J Endod. 2000 Dec;26(12):756-9.
10. Gurgel-Filho ED, Feitosa JP, Gomes BP, Ferraz CC, Souza-Filho FJ, Teixeira FB. Assessment of different gutta-percha brands during the filling of simulated lateral canals. Int Endod J. 2006 Feb;39(2):113-8.
11. Hata G, Kawazoe S, Toda T, Weine FS. Sealing ability of thermoplasticized gutta-percha fill thecniques as assessed by a new method of determining apical leakage. J Endod. 1995 Apr;21(4):167-72.
12. Ingle JI, Bakland LK. Endodontics. 4. ed. Baltimore: Willians & Wilkins; 1994.
13. Jurcak JJ, Weller RN, Kulild JC, Donley DL. In vitro intracanal temperatures produced during warm lateral condensation of Gutta-percha. J Endod. 1992 Jan;18(1):1-3.
14. Leonardo MR. Endodontia: tratamento de canais radiculares. São Paulo: Artes Médicas; 2005.
15. Lopes HP, Siqueira Jr JF. Endodontia: biologia e técnica. Rio de Janeiro: Guanabara Koogan; 2004.
16. Maniglia-Ferreira C, Almeida-Gomes F, Guimarães NLSL, Ximenes TA, Canuto NSCP, Vitoriano MM. Análise da capacidade de preenchimento de canais radiculares com guta-percha promovida por três diferentes técnicas de obturação de canais radiculares. RSBO. 2011 Jan-Mar;8(1):19-26.
17. Morgental RD, Zanatta LRN, Rahde NM. Avaliação da obturação de canais laterais e secundários artificiais com diferentes técnicas obturadoras. Rev Odonto Ciênc. 2008 Jul-Sep;23(3):273-7.
18. Parks ET, Williamson GF. Digital radiograph: an overview. J Contemp Dent Pract. 2002 Nov;3(4):23-39.
19. Ramos CAS, Bramante CM. Endodontia: fundamentos biológicos e clínicos. São Paulo: Santos; 2001.
20. Raymundo A, Portela CP, Leonardi DP, Baratto-Filho F. Análise radiográfica do preenchimento de canais laterais por quatro diferentes técnicas de obturação. RSBO. 2005 Nov;2(2):22-7.
21. Reader CM, Himel VT, Germain LP, Hoen MM. Effect of three obturation techniques on the filling of lateral canals and the main canal. J Endod. 1993 Aug;19(8):404-8.
22. Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967 Nov;11:723-44.
23. Seltzer S, Bender IB, Smith J, Freedman I, Nazimov H. Endodontic failures – an analysis based on clinical, roentgenographic, and histologic findings. I. Oral Surg Oral Med Oral Pathol. 1967 Apr;23(4):500-16.
24. Venturi M, Di Lenarda R, Prati C, Breschi L. An in vitro model to investigate filling of lateral canals. J Endod. 2005 Dec;31(12):877-81.
25. Weine FS. The enigma of the lateral canal. Dent Clin North Am. 1984 Oct;28(4):833-52.
26. Weller RN, Kimbrough WF, Anderson RW. A comparison of thermoplastic obturation techniques: adaptation to the canal walls. J Endod. 1997 Nov;23(11):703-6.
27. Xu G, Zhang Z. Filling of the lateral canal: report of two cases. Oral Surg. 1984 Aug;58(2):221-4.
28. Yee FS, Marlin J, Krakow AA, Gron P. Three-dimensional obturation of the root canal using injection-molded, thermoplasticized dental gutta-percha. J Endod. 1977 May;3(5):168-74.
 Correspondence:
Correspondence:
Clarissa Teles Rodrigues
Rua Manoel Januário de Andrade, n.º 308 – Recreio
CEP 45020-540 – Vitória da Conquista – BA – Brasil
E-mail:clarit@uol.com.br
Received for publication: November 10, 2011.
Accepted for publication: January 09, 2012.
