










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Original Research Article
Ability of different methods to fill retrograde cavities with MTA
Roberta Bosso I; Rodrigo Colturato Chagas I; Arturo Aranda-GarciaI; Ana Carolina Venção I; Juliane Maria Guerreiro-Tanomaru I; Mario Tanomaru-Filho I
ABSTRACT
Introduction: The Mineral Trioxide Aggregate (MTA) has excellent biological property. However, its consistency makes it difficult to be inserted into retrograde cavities. Objective:To evaluate the ability of different methods to fill retrograde cavities with MTA. Material and methods: Root canals of thirty single-rooted resin teeth were prepared and filled. After the cut of 3 mm short of apical third, retrograde cavities with 3 mm deep were prepared using an ultrasound device and retrotips (CVD, São José dos Campos, SP, Brazil). The retrograde preparation was evaluate by using an operative microscope (D.F. Vasconcellos, São Paulo, SP, Brazil). The teeth were randomly divided into three groups (n = 10), according to the method: 1) condenser (Trinity, São Paulo, SP, Brazil); 2) MTA applicator (Angelus, Londrina, Brazil) + condenser; 3) condenser associated with ultrasound (CVD, São José dos Campos, SP, Brazil). After the filling of retrograde cavities with white MTA (Angelus, Londrina, Brazil), teeth were radiographed using a digital system (Kodak RVG 6000, Rochester, NY, USA). The images were analyzed by UTHSCSA Image Tool 3.0 software. The percentage of filling was calculated by the proportion between the total area of retrograde cavity and the filled area. The radiographic density mean of each third of retrograde cavity filled with MTA was measured by using the histogram tool of the software. The results were submitted to ANOVA and Tukey tests, with 5% of significance. Results: There was no difference in percentage of filling among the groups (p > 0.05) (approximately 85%). By comparing the thirds, the condenser and MTA applicator groups showed higher density for apical and middle third than cervical third (p < 0.05). The ultrasound group presented similar density among the thirds. Conclusion: The filling ability was similar for the studied methods. Ultrasound promoted better distribution of MTA in retrograde cavity, but did not increase the density of material.
Keywords: Mineral Trioxide Aggregate; apicectomy; retrograde filling.
Introduction
Surgical procedure may be necessary in cases of either conventional endodontic treatment failure or when this cannot be performed 5. Among the techniques indicated, retrograde obturation comprises the apicoectomy and the retrograde cavity preparation followed by the insertion of the retrofilling material 15.
To perform the retrograde cavity, the introduction of the ultrasonic tips enables the preparation of a cleaner and deeper cavity more centered at the root canal 2,7,15. The retro-preparation executed through diamond ultrasonic tips 2 has been used because it favors the sealing and marginal adaptation of the retrofilling materials 17. The retrofilling materials are inserted into the retrograde cavity aiming to provide apical sealing and to prevent microorganism penetration, decreasing the leakage of irritating agents in the material/canals wall interface 4 and contributing to periapical repair.
Several retrofilling materials have been studied, such as dental amalgam, zinc oxide and eugenol-based cements (IRM and Super-EBA), Sealer 26 and mineral trioxide aggregate (MTA) 3,10,22. MTA has demonstrated advantages as sealing 26,27, marginal adaptation 29 and possibility of use in the presence of humidity 24. MTA presents excellent biological property 3,16. However, its sandy consistence makes it difficult to handle 8 and insert in retrograde cavities during parendodontic surgeries 11. Methods for MTA insertion have employed condensers and applicator syringes. Notwithstanding, in the clinical situations of retrograde cavity filling by this material, its insertion is difficult because of the location and small size of the cavity 12. The ultrasound may be used to help the insertion of the endodontic cement during root canal obturation aiming to favor root canal filling 1,9,19,28. Therefore, the use of ultrasound could be suggested as an auxiliary tool for MTA insertion in retrograde cavities.
The aim of this study was to assess the filling ability of different methods to fill retrograde cavities with MTA through condensers, MTA applicator, or ultrasound.
Material and methods
Thirty single-rooted resin teeth were used. The teeth had their crowns sectioned, resulting in roots of 15 mm of length. The roots were instrumented through rotary system (Mtwo, VDW, Munich, Germany) up to size #25 (.06) and filled with gutta-percha (Mtwo, VDW, Munich, Germany) and endodontic cement (AH Plus, Dentsply De Trey Gmbh, Konstanz, Germany) through single cone technique. Irrigation was executed through 2.5% sodium hypochlorite. After obturation, the roots were sectioned perpendicularly at their long axis 3 mm short of the apex. Retrograde cavities with 3 mm deep were prepared by retrotips (CVD, São José dos Campos, SP, Brazil) coupled to an ultrasound device with the aid of operative microscope (D.F. Vasconcellos, São Paulo, SP, Brazil). The teeth were randomly divided into three groups (n = 10). All groups were filled with MTA (Angelus, Londrina, PR, Brazil), which was inserted into the retrograde cavity through the different methods, according to the different groups:
1) Condenser – only a condenser was used (Trinity, São Paulo, SP, Brazil);
2) Applicator/condenser – MTA applicator (Angelus, Londrina, PR, Brazil) was used for the insertion of the material, followed by the condenser;
3) Ultrasound – the material was inserted by using the condenser associated with ultrasound device (CVD, São José dos Campos, SP, Brazil) which was placed onto the lateral surface of the condenser (Trinity, São Paulo, SP, Brazil).
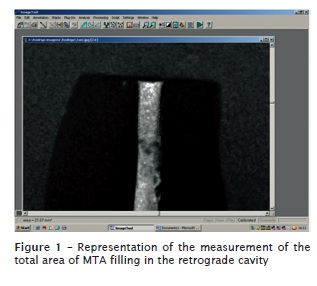
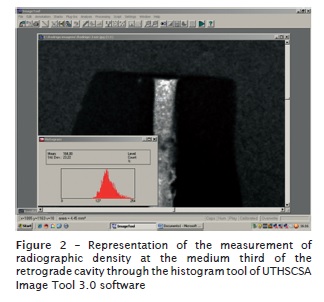
Before and after the filling of retrograde cavities with MTA, the teeth were radiographed by using a digital radiograph system (Kodak RVG 6000, Rochester, NY, USA). To obtain standardized radiographic images, a radiographic positioning device was used and the teeth were inserted into a silicon mold. The images were analyzed through UTHSCSA Image Tool 3.0 software to assess the percentage of filling and the radiographic density of the retrofilling material. The percentage of filling was calculated by the proportion between the total area of the preparation and the total area of filling (figure 1). To evaluate the radiographic density, the retrograde cavity was divided into three thirds (apical, medium and cervical). The radiographic density mean of each third was measured through the histogram tool of the aforementioned software (figure 2). The data obtained were submitted to Anova and Tukey tests, with level of significance of 5%.
Results
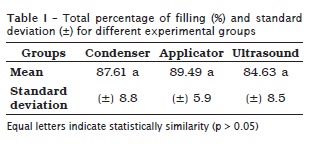
The three insertion techniques showed statistically similar values (p > 005), of about 85%, in the total percentage of MTA filling of retrograde cavities, as seen in table I.
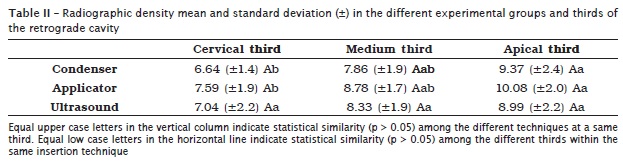
When the radiographic density of MTA was analyzed according to the different techniques at the same third, all methods were not capable of increasing the material density (p > 0.05). However, the evaluation of MTA density at different thirds in the same insertion technique showed that when the condenser and applicator were applied, there was a greater density at apical and medium than cervical third (p < 0.05). However, when ultrasound was used, the density was similar among the three thirds (p > 0.05) (table II).
Discussion
The persistency of microorganism within the root canal system may lead to endodontic treatment failure 13. The retrofilling aims to fill the retrograde cavity by a material with proper properties 12. MTA is a powder composed of thin hydrophilic particles whose curing is achieved in the presence of humidity. The result of the powder hydration is a colloidal gel with pH of 12.5 which solidifies, becoming a rigid structure. This cement has been considered as an ideal retrofilling material because of its low solubility and cytotoxicity and good tissue tolerance, in addition to enable the induction of mineralized tissue formation 25. Notwithstanding, its disadvantage is the difficulty of insertion and filling of the retrograde cavity. Generally, MTA insertion is accomplished through condensers or applicators designed for this purpose. However, the preparation size and retrograde cavity location associated with the physical characteristic of MTA makes its insertion difficult. Aiming to facilitate this material insertion, Lee 12 proposed a new technique comprising the insertion of MTA by small increments, immediately after its handling, which are condensed and polished with the aid of size #3 Hollenback instrument (Hartzell & Sons, Concord, CA). The use of ultrasound to insert the endodontic cement during root canal obturation has been suggested, which may favor the filling and density of the material during the procedure 1, the effectivity of insertion within root canals 9 and the filling of accessory canals 19. The results of this present study demonstrated that the use of ultrasound helped in the distribution of the material for all thirds of the retrograde cavity, but it did not favor a greater density in the filling by MTA, because this latter depends on the consistency of the material, making a higher performance of the condenser impossible.
The evaluation of the retrofilling material filling inside the cavity is of great importance, because an inappropriate filling may result in sealing failure and, consequently, in surgical treatment failure. The results of this study revealed that the three techniques (condenser, applicator and ultrasound) were similar and filled, in average, about 85% of the total area of the retrofilling.
The radiopacity is other essential property of a retrofilling material to allow that it be distinguished from the surrounding anatomical structures, such as bone and dentin 18,20. To measure the radiopacity, the method of obtainment and comparison of radiographic images of the materials, an aluminum scale with increasing values has been employed. The radiographs are digitized and by the material density (pixels) and the radiopacity value (aluminum equivalence) is determined by software 6,21. MTA contains bismuth oxide as radiopacifier. Tanomaru-Filho et al. 23, by analyzing the radiopacity of MTA (Angelus), verified that this is approximately 3.0 mm of aluminum.
The evaluation tool of the density of the radiographic image was employed to differentiate the filling ability of the different methods, once the better the filling the higher the radiographic density of the material. Therefore, the density of the cement filling in the retrograde cavity was evaluated by the histogram tool of UTHSCSA Image Tool 3.0 software. The analysis of the retrograde cavity was divided into three thirds. The different techniques when evaluated at the same third, did not promote an increase in the density of the material. However, the insertion techniques through condenser and applicator promoted a higher density of MTA at apical and medium than cervical third (p < 0.05). Only after the use of the ultrasound, the density was similar among the thirds (p > 0.05), showing that this technique achieved a more homogeneous distribution of MTA within retrograde cavity.
Conclusion
The ability to fill the retrograde cavities with MTA was similar for the three methods studied. The analysis of MTA density indicates that the use of ultrasound provide a greater distribution of MTA within the retrograde cavity. Notwithstanding, ultrasound was not capable of increasing the material density.
References
1. Aguirre AM, El-Deeb ME, Aguirre R. The effect of ultrasonics on sealer distribution and sealing of root canals. J Endod. 1997 Dec;23(12):759-64. [ Links ]
2. Bernardes RA, Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR et al. Evaluation of apical cavity preparation with a new type of ultrasonic diamond tip. J Endod. 2007 Apr;33(4):484-7.
3. Fernandez-Yanez SA, Leco-Berrocal MI, Martinez-Gonzalez JM. Metaanalysis of filler materials in periapical surgery. Med Oral Patol Oral Cir Bucal. 2008 Mar;13(3):180-5.
4. Gondim EJ, Kim S, Souza-Filho FJ. An investigation of microleakage from root-end fillings in ultrasonic retrograde cavities with or without finishing: a quantitative analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005 Jun;99(6):755-60.
5. Hirsch JM, Ahlstrom U, Henrikson PA, Heyden G, Peterson LE. Periapical surgery. Int J Oral Surg. 1979 Jun;8(3):173-85.
6. Húngaro Duarte MA, Oliveira El, Kadre GD, Vivan RR, Guerreiro Tanomaru JM, Tanomaru Filho M et al. Radiopacity of portland cement associated with different radiopacifying agents. J Endod. 2009 May;35(5):737-40.
7. Ishikawa H, Sawada N, Kobayashi C, Suda H. Evaluation of root-end cavity preparation using ultrasonic retrotips. Int Endod J. 2003 Sep;36(9):586-90.
8. Jacobovitz M, Pappen FG, Lima RKP. Obturação com MTA associada à cirurgia parendodôntica no retratamento de reabsorção radicular apical externa: relato de caso. RSBO. 2009 Jun;6(2):208-13.
9. Kahn FH, Rosenberg PA, Schertzer L, Korthals G, Nguyen PN. An in-vitro evaluation of sealer placement methods. Int Endod J. 1997 May;30(3):181-6.
10. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006 Jul;32(7):601-23.
11. Kogan P, He J, Glickman GN, Watanabe I. The effects of various additives on setting properties of MTA. J Endod. 2006 Jun;32(6):569-72.
12. Lee ES. A new mineral trioxide aggregate root-end filling technique. J Endod. 2000 Dec;26(12):764-5.
13. Leonardi DP, Fagundes FS, Haragushiku GA, Tomazinho PH, Baratto-Filho F. Endodontic surgery: evaluation of different techniques for accomplishment of apicoectomy. RSBO. 2006;3(2):15-9.
14. Lodi LM, Poleto S, Soares RG, Irala LED, Salles AA, Limongi O. Paraendodontic surgery: case report. RSBO. 2008;5(2):69-74.
15. Martí Bowen E, Peñarrocha M. An update in periapical surgery. Med Oral Patol Oral Cir Bucal. 2006 Nov;11(6):503-9.
16. Reis-Araújo CJ, Paim KS, Rios MA, Albuquerque DS, Baratto-Filho F, Vanni JR. Estudo histológico comparativo entre MTA e cimento Portland. RSBO. 2008 Aug;5(2):57-63.
17. Rosales-Leal JI, Olmedo-Gaya V, Vallecillo-Capilla M, Luna-del Castillo JD. Influence of cavity preparation technique (rotary vs. ultrasonic) on microleakage and marginal fit of six end-root filling materials. Med Oral Patol Oral Cir Bucal. 2011 Mar;16(2):185-9.
18. Shah PMM, Chong BS, Sidhu SK, Ford TRP. Radiopacity of potential root-end filling materials. Oral Surg Oral Med Oral Pathol. 1996 Apr;81(4):476-9.
19. Stamos DE, Gutmann JL, Gettleman BH. In vivo evaluation of root canal sealer distribution. J Endod. 1995 Apr;21(4):177-9.
20. Tagger M, Katz A. A standard for radiopacity of root-end (retrograde) filling materials is urgently needed. Int Endod J. 2004 Apr;37(4):260-4.
21. Tagger M, Katz A. Radiopacity of endodontic sealers: development of a new method for direct measurement. J Endod. 2003 Nov;29(11):751-5.
22. Tanomaru-Filho M, Bronzi ES, Wilhelmsen NSW, Duarte MAH. Capacidade seladora do Sealer 26 e AH Plus em obturações retrógradas. Rev Paul Odontol. 1999 Feb;21(1):34-6.
23. Tanomaru-Filho M, Silva GF, Húngaro Duarte MA, Gonçalves M, Guerreiro Tanomaru JM. Radiopacity evaluation of root-end filling materials by digitization of images. J Appl Oral Sci. 2008 Dec;16(6):376-9.
24. Torabinejad M, Higa RK, McKendry DJ, Pitt Ford TR. Dye leakage of four root end filling materials: effects of blood contamination. J Endod. 1994 Apr;20(4):159-63.
25. Torabinejad M, Pitt Ford TR. Root end filling materials: a review. Endod Dent Traumatol. 1996 Aug;12(4):161-78.
26. Torabinejad M, Rastegar AF, Kettering JD, Pitt Ford TR. Bacterial leakage of mineral trioxide aggregate as a root end filling material. J Endod. 1995 Mar;21(3):109-21.
27. Torabinejad M, Watson TF, Pitt Ford TR. Sealing ability of a mineral trioxide aggregate when used as a root end filling material. J Endod. 1993 Dec;19(12):591-5.
28. Wiemann AH, Wilcox LR. In vitro evaluation of four methods of sealer placement. J Endod. 1991 Sep;17(9):444-7.
29. Xavier CB, Weismann R, Oliveira MG, Demarco FF, Pozza DH. Root-end filling materials: apical microleakage and marginal adaptation. J Endod. 2005 Jul;31(7):539-42.
 Correspondence:
Correspondence:
Mário Tanomaru-Filho
Rua Humaitá, 1680 – Centro – Caixa Postal 331
CEP 14801-903 – Araraquara – SP – Brasil
E-mail:tanomaru@uol.com.br
Received for publication: March 12, 2012.
Accepted for publication: April 04, 2012.
