










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Case Report Article
Location of three canals in the mesiobuccal root of the maxillary first molar
Andressa Salles Gonçalves Pais I ; Carlos Eduardo Fontana II ; Alexandre Sigrist De Martin II ; Elcia Bravin de Carvalho I ; Carlos Eduardo da Silveira Bueno II
II Department of Dentistry, São Leopoldo Mandic Center of Post-Graduation – Campinas – SP – Brazil.
ABSTRACT
Introduction:The knowledge on the complex anatomy of the maxillary first molar and location of extra canals are essential for diagnosis and endodontic treatment success. Objective:The purpose of this study was to report a clinical case showing a varied number of root canals in maxillary molars with the aid of the operating microscope (OM). Case report: The endodontic retreatment of the right maxillary first molar with unusual anatomical variation was performed, displaying three canals in the mesiobuccal root (MB), a root canal in the distobuccal root (DV) and a root canal in the palatal root (P). To remove the resin core inside pulp chamber with and without the aid of dental operating microscope, a high-speed drill and ultrasonic tip (diamond round) was used, respectively, for the refinement of the pulp chamber walls. The dental operating microscopewas used during the access surgery, location, negotiation of canals and checking of the completion of all stages of the retreatment. Subsequently, the cleaning, shaping and filling of the root canal system was completed. The presence of three canals in the mesiobuccal root, one in the distobuccal root and one in the palatal root was found. Conclusion: Variations in the number of canals could be confirmed during the surgery access in endodontic retreatment cases with the aid of dental operating microscope.
Keywords: dental operating microscope; maxillary first molar; endodontic retreatment; mesiobuccal canal.
Introduction
The knowledge on the complex external and internal tooth morphology is important to perform the diagnosis and treatment of the root canal system, minimizing endodontic treatment failures, which may compromise its success 6,16,18,19,22 because either of the incomplete removal of the pulp tissue, mainly in areas which are not accessed during root canal cleaning and shaping or the inappropriate coronary and apical sealing of the obturation. The constant challenge of the total cleaning of root canal system especially occurs in multiradicular teeth 5. Vigouroux and Trugeda Bosaans 22 conducted an important study in which they examined in detail the configuration of pulp chamber floor (shape, dimentions, relationship with the intrapulpar sulcus and tapered shape of the root canals openings) in 134 maxillary first molars.
The unprecedented publishing of a study by Cecic et al, in 1982, reporting a maxillary first molar showing five canals with two mesiobuccal (MB) canals, one distobuccal (DB) canal and two palatal (P) canals 4. Gray 11 observed five canals in 2.4% of the maxillary first molars with two MB canals , two DB canals and one P canal. However, in this study, the occurrence of three root canals in MB root was not reported. On the other hand, the studies of Beatty 3, Ferguson et al. 8 and Favieri et al. 6, reported five root canals showing three canals in MB root. Maggiore et al. 16 located three roots and filled six canals in the maxillary first molar, displaying two MB canals, one DB canal, and one main P canal which was divided into three canals at the apical third. The author affirmed that several failures in the endodontic treatment occurs because of the lack of location and cleaning of MB2 and that molars showing four root canals are more frequent than those showing three canals. Kottoor et al. 13,14 reported the endodontic treatment of the maxillary first molar with seven and eight canals, respectively, confirmed through the operating microscope and the aid of cone beam computed tomography.
Fogel et al. 9 examined the configuration of the location of the root canals in MB roots through surgical telescope, optical fiber and endodontic explorer. The authors concluded that the accuracy in locating the MB2 canal depends on the use of magnification, proper illumination and modified access and concluded that 71.2% of the teeth had their canals negotiated, from which 31.7% showed two distinct foramens.
An in vitro study on 51 maxillary permanent molars conducted by Kulild and Peters in 1990 15 demonstrated the presence of MB2 canal in 96.1% of the teeth after sectioning 1 mm cuts, which were verified under microscopy. A variety of methods in the literature has been suggested to help the location of MB2 canals. Ferguson et al. 8 used a method of weariness of the sulcus between the MB1 and palatal canals with the aid of a size 2 round bur at low speed.
The operating microscope has helped the clinicians to locate the mesiobuccal canals 5,7. Ferguson et al. 8 employed the operating microscope to analyze the incidence of MB2 in 45 maxillary molars and observed that this tool considerably increases the chances of the location and endodontic treatment of MB2 canal.
Current in vitro studies on the morphology of mesiobuccal root of the maxillary first molar through computed tomography concluded that MB2 canal is present in 80% of 30 teeth evaluated 20.
The aim of this study was to report the importance of visual magnification and microscopic documentation in the location of five root canals on the pulp chamber floor during a endodontic retreatment of a right maxillary permanent first molar showing three roots, comprising three canals in the mesiobuccal (MB) root, one canal in distobuccal (DB) root and one canal in the palatal (P) root.
Case report
A 35-year-old female patient sought treatment in a private dental office. During anamnesis, she did not report any contributory disease. Her chief complaint was the need of endodontic retreatment of the right maxillary permanent first molar due to prosthodontic reasons. At this first appointment, this tooth was completely asymptomatic (negative) to clinical tests: pulp tenderness, vertical and horizontal percussion, coronary and apical palpation. The tooth showed no mobility and periodontal pocket after gingival sulcus probing at buccal, palatal, mesial and distal surfaces. There were no signs of fistula or swelling.
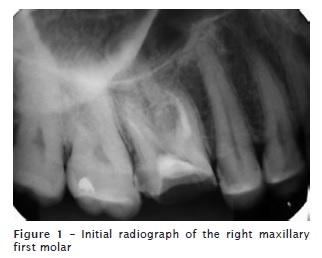
The radiographic examination (figure 1), exhibited three completely formed roots with no apical rarefaction, but showed a deficient filling within the MB root, lacking of the filling material within the DB and P canals, which confirmed the referral for endodontic retreatment of this tooth and the need of the construction of a new post and core and crown.
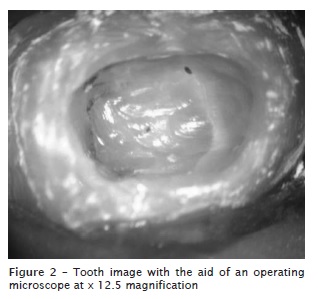
After the anesthesia of the right posterior alveolar nerve with 4% articaine and 1:100,000 adrenalin (Articaíne DFL, Indústria e Comércio Ltda., Rio de Janeiro, RJ, Brazil), the resin core was removed from the pulp chamber almost reaching the pulp floor. Following, absolute isolation was executed with the aid of a clasp and the mechanical removal of the resin material was finished (figure 2) with the aid of an operating microscope (DFVasconcelos, São Paulo, Brazil) at x 12.5 and a diamond-coated ultrasonic round tip (Trinks, São Paulo, Brazil). Copious irrigation by 5.25% sodium hypochlorite (Biofarm, Espírito Santo, Brazil) and the refinement of all pulp chamber walls by using the same ultrasonic round tip as well as a minimum weariness between the openings of MB1 and P canals was performed.
Pulp floor was probed through a straight endodontic explorer (Odous De Deus, Belo Horizonte, Brazil) to check the possible extra canals. Through the aid of the operating microscope, the filling material inside MB1 canal was removed by using a size ST21 ultrasonic tip (Enac, Osada, Japan). The first checking of the presence of the orifices of the MB1, DB, and P canals was confirmed through the operating microscope. The MB2 canal was firstly located with the aid of a size #10 instrument (CC Cord, Inc United Dental Manufactures, Germany) pre-curved through pliers (Odous De Deus, Belo Horizonte, Brazil) and then negotiated.
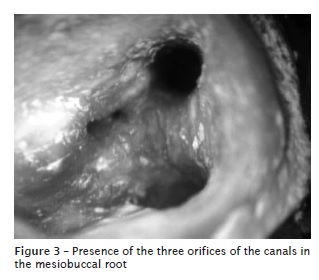
The cleaning and shaping of the canals were concluded and a second checking through operating microscope of the MB1, MB2, DB and P canals was performed, which enabled the location of the MB3 orifice in the MB root (figure 3). After several attempts of negotiation through size #8, #10 and #15 pre-curved instruments (CC Cord, Inc United Dental Manufactures, Germany), it was chosen to executed a gentle weariness of the sulcus on the pulp chamber floor, which starts in the orifice of the MB1 canal towards the orifice of the P canal, with the aid of a diamond-coated ultrasonic round tip.
At the second clinical appointment, the instrumentation was carried out through the enlargement of the cervical and medium thirds by using Gates-Glidden bur (Dentsply Maillefer, Switzerland) in decreasing order, that is, size #4, #3, #2, and #1, as well as the technique of segmented preparation with the aid of nickel-titanium Pro-Design instruments (Easy Endo Equipments, Belo Horizonte, Brazil), under copious irrigation with 5.25% sodium hypochlorite. The apical locator (NovApex-Fórum Engineering Technologies, Israel) confirmed the real root canal length based on the initial radiograph, while the trans-operative radiographed confirmed the relationship among the instruments inside the canals, their inclinations and location of the possible junction of the MB1 and MB2 canals.
Following, a final irrigation was performed with 5 ml of 17% EDTA (Biofarm, Espírito Santo, Brazil). After 3 minutes the canals were irrigated with 5.25% sodium hypochlorite which was vibrated by the passively insertion of a ST21 ultrasonic tip. Root canals were dried with the aid of size 0.019 Capillary Tips (Ultradent Products, Inc South Jordan, Utah, USA) and fine-medium size absorbent paper points (Endopoints, Indústria e Comércio, Rio de Janeiro, Brazil), one at each canal. The working length of a fine-medium size gutta-percha point (Microtips, Ultimate Dental, Tenn, Korea) was established at 0.5 mm short of the apex of the main canals, with following obturation through continuous wave of condensation and endodontic sealer (Pulp Canal Sealer Extended Work Time, Sybron Endo, EUA). The System B Heatsourse (Analytic Endodontics Redmond, WA, USA) was used to condense the gutta-percha at the Downpack phase. At the Backfilling phase of the canals, an injection pistol for heated gutta-percha was used (Obtura II, Obtura Corp., Fenton, USA), except for the palatal canal, where 2/3 of the working length was left empty to receive a post.
Immediately after the obturation of the root canals, a provisional material (Coltosol, Vigodent SA Indústria e Comércio, Rio de Janeiro, Brazil) was inserted at 3 mm short of the orifices of the mesiobuccal and distobuccal canals to enable the cementation of a provisional crown. The final restoration of the tooth was achieved by a metallic post and core and the total crown.
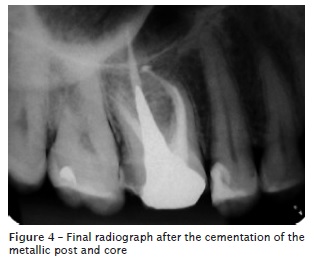
Orthoradial radiographic examination enabled to analyze the final obturation of the root canal systems and the installation of the metallic post and core (figure 4).
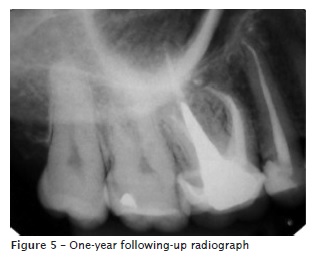
Radiographic following-up after 1 year of the endodontic retreatment and the lack of symptoms and radiographic alterations confirmed the treatment success (figure 5).
Discussion
The knowledge on the complex tooth morphology of the maxillary first molar is an important factor for the planning and execution of endodontic therapy. There are situations in which the endodontist only succeeds in locating extremely atresic and/or calcified orifices of root canals and is not capable of negotiating them to perform instrumentation, even with the aid of the operating microscope.
Goga et al. 10 concluded that the limitation existing in the radiographic image which provide a bidimensional image of the teeth, in addition to the superposition of canals and roots of multiradicular teeth, makes difficult the location of extra canals and not resulting in clear evidence of their existence, which justifies the necessity of pre-, trans-, and post-operative radiographs at different angulations to facilitate their observation. Weine and Eskoz 23 affirmed that the clinical and radiographic following-up appointments are essential, mainly in cases of endodontic retreatment, whose prognosis is always more questionable regarding to healing than the endodontic treatment. Currently, other method employed for confirming the anatomical variations and extra root canals is cone beam computed tomography 1,13.14.
The composite resin core within the pulp chamber is difficult to remove safely by naked eye because of the close contact of this restorative material with the pulp chamber floor and its color very similar to dentin. This new concept of crown bonding to restorative materials enables the increasing of iatrogenic procedures such as pulp floor perforations, which justifies the use of ultrasonic tips providing a minimum weariness of this site. Yoshioka et al. 24 recommended that the negotiation of MB2 may be executed within a safe limit, confirming that the negotiation of any root canal should be carefully performed to prevent accidents. This is also valid for MB3 canals.
To perform the endodontic treatment, the clinician should keep in mind the external tooth morphology and the internal morphology of the pulp chamber floor, even with the aid of magnification, illumination 5,7 and straight endodontic explorer, as used in the studies of Yoshioka et al. 24. The large surgical access, adequate illumination without the use of an operating microscope, and the use endodontic instruments contributed for the location of the canals 6.
There are several methods for the location of the canals. In this case report, the insertion of the diamond-coated ultrasonic round tip and the small weariness between the MB1 and P canal was employed. On the case report described by Ferguson et al. 8, the method of choice to locate the canals was to perform a weariness through size #2 round bur at low speed, resulting in the location of three canals in the MB of the maxillary first molar 8. India 2, methylene blue dyes and fluorescein plus optical fiber 17 may be employed to detect the orifices of atresic and/or calcified canals.
Studies of Imura et al. 12 confirmed the increasing of the location rate of the canals because of the highest knowledge on the internal morphology, modification of the opening shape and use of the operating microscope. All these factors positively influenced the success rate of the treatment 16,18.
Rotary instrumentation was chosen in this case report because of its advantage in reducing the time amount of the biomechanical preparation and the failures related to the instrumentation 5.
The effect of the irrigation solution, such as 5.25%, sodium hypochlorite and 17% EDTA chelating solution on the removal of the smear layer helped the cleaning of the root canals system in areas where the endodontic instruments are not capable of reaching and consequently provided the penetration of the endodontic sealer and thermoplasticized gutta-percha. This case report confirmed through distoradial radiograph the presence of the isthmus at the medium third of the canals 6. According to the studies of Vertucci 21, 75% of the isthmus were observed in this third and 15% in the apical third.
This case report showed that the clinicians must know the anatomical variation during all phases of the endodontic diagnosis and treatment, because the adequate root canal therapy can be performed respecting the possible challenges of the anatomical space of the pulp. Additionally, the use of the operating microscope may be decisive for the endodontic treatment success.
Conclusion
Variations in the number of the canals can be confirmed during the access surgery in cases of endodontic retreatment with the aid of the operating microscope.
References
1. Abuabara A, Schreiber J, Baratto-Filho F, Cruz GV, Guerino L. Análise da anatomia externa no primeiro molar superior por meio da tomografia computadorizada cone beam. RSBO. 2008 Aug;5(2):38-40. [ Links ]
2. Baratto-Filho F, Zaitter S, Haragushiku GA, Campos EA, Abuabara A, Correr GM. Internal anatomy of maxillary first molars by using different methods. J Endod. 2009 Mar;35(3):337-42.
3. Beatty RG. A five-canal maxillary first molar. J Endod. 1984 Apr;10(4):156-7.
4. Cecic P, Hartwell G, Bellizzi R. The multiple root canal system in the maxillary fist molar: A case report. J Endod. 1982 Mar;8(3):113-5.
5. Cunha RS, Davini F, Fontana CE, Miguita KB, Bueno CES. O conceito microsonics: primeiro molar superior com cinco canais – relato de caso. RSBO. 2011 Apr-Jun;8(2):231-5.
6. Favieri A, Barros FGB, Campos LC. Root canal therapy of a maxillary first molar with five root canals: case report. Braz Dent J. 2006;17(1):75-8.
7. Feix LM, Boijink D, Ferreira R, Wagner RH, Barletta FB. Microscópio operatório na Endodontia: magnificação visual e luminosidade. RSBO. 2010 Sep;7(3):340-8.
8. Ferguson DB, Kjar KS, Hartwell GR. Three canals in the mesiobuccal root of a maxillary first molar: a case report. J Endod. 2005 May;31(5):400-2.
9. Fogel HM, Christie WH, Peikoff MD. Canal configuration in the mesiobuccal root of the maxillary first molar: a clinical study. J Endod. 1994 Mar;20(3):135-7.
10. Goga R, Chandler NP, Oginni AO. Pulp stones: a review. Int Endod J. 2008 Jun;41(6):457-68.
11. Gray R. The maxillary first molar. In: Bjorndal A, Skidmore E, eds. Anatomy and morphology of the human teeth. Lowa City: Univerty of lowa; 1983. p. 31-40.
12. Imura N, Hata G, Toda T, Otani SM, Fagundes MIRC. Two canals in mesiobuccal roots of maxillary molars. Int Endod J. 1998 Nov;31(6):410-4.
13. Kottoor J, Velmurugan N, Sudha R, Hemamalathi S. Maxillary first molar with seven root canals diagnosed with cone-beam computed tomography scanning: a case report. J Endod. 2010 May;36(5):915-21.
14. Kottoor J, Velmurugan N, Surendran S. Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning: a case report. J Endod. 2011 May;37(5):715-9.
15. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod. 1990 Jul;16(7):311-7.
16. Maggiore F, Jou YT, Kim S. A six-canal maxillary first molar: case report. Int Endod J. 2002 May;35(5):486-91.
17. Nallapati S, Glassman G. Use of ophthalmic dye in root canal location. Endodontic Practice. 2004 Jun;15(6):1-6.
18. Ozcan E, Aktan AM, Ari H. A case report: unusual anatomy of maxillary second molar with 3 mesiobuccal canals. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Jan;107(1):e43-6.
19. Pasternak Jr B, Teixeira CS, Silva RG, Vansan LP, Sousa Neto M. Treatment of a second maxillary molar with six canals. Aust Endod J. 2007 Apr;33(1):42-5.
20. Somma F, Leoni D, Plotino G, Grande NM, Plasschaert A. Root canal morphology of the mesiobuccal root of maxillary first molars: a micro-computed tomographic analysis. Int Endod J. 2009 Feb;42(2):165-74.
21. Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol. 1984 Nov;58(5):589-99.
22. Vigouroux SAA, Trugeda Bosaans SA. Anatomy of the pulp chamber floor of the permanent maxillary first molar. J Endod. 1978 Jul;4(7):214-9.
23. Weine FS, Eskoz N. Canal configuration of the mesiobuccal root of the maxillary second molar. J Endod. 1995 Jan;21(1):38-42.
24. Yoshioka T, Kikuchi I, Fukumoto Y, Kobayashi C, Suda H. Detection of the second mesiobuccal canal in mesiobuccal roots of maxillary teeth ex vivo. Int Endod J. 2005 Feb;38(2):124-8.
 Correspondence:
Correspondence:
Andressa Salles Gonçalves Pais
Av. Américo Buaiz, n.º 501
Ed. Victoria Office Tower – Torre Norte, sala 307 – Enseada do Suá
CEP 29050-911 – Vitória – ES – Brasil
E-mail:andressa_pais@hotmail.com
Received for publication: October 04, 2011.
Accepted for publication: December 14, 2011.
