










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Case Report Article
Free-hand stratification with composite resins for the closure of anterior diastema
Leonardo Fernandes da Cunha I,III; Thiago Majolo Valeretto I; Rodrigo Pirolo II; José Mondelli I,III; Carla Castiglia Gonzaga II; Adilson Yoshio Furuse II
II Post-graduation in Dentistry, Professional Master Course in Clinical Dentistry, Positivo University – Curitiba – PR – Brazil.
III Operative Dentistry, Funorte – Resende – RJ – Brasil.
ABSTRACT
Introduction: Dental diastemas are common findings at dental clinics. This clinical situation produces discomfort in many patients and its solution is difficult to many professionals. Silicone guides, made from waxed casts, have been used to assist the stratification of resin composites in cases of dental diastemas. This technique, however, does not necessarily need to be used as protocol in all situations. Objective: To demonstrate the stratification technique without silicone guides. Case report: The present study reports a case of stratification technique for anterior diastemas closure without silicone guide. Conclusion: The closure of diastemas can be quickly and easily performed using composite resins without the need of previously manufacturing silicone guides.
Keywords: diastema; dental aesthetics; composite resins.
Introduction
Tooth diastemas are gaps or spaces between two adjacent teeth in the same tooth arch 5. They show multifactorial aethiology and very common occurrence in general population. These spaces may frequently cause aesthetic damage to the smile and dentofacial harmony. Thus, the solution of this clinical problem has been constantly searched. Additionally, the spaces between anterior teeth are a common occurrence after orthodontic treatment. In these cases, a restorative procedure is required 6.
The restorative technique may generate several questions to the dentists. Currently, the use of silicone guide has been largely recommended to reproduce the palatal anatomy of fractured anterior teeth, as well as to reconstruct the occlusion guides 9 and conoid lateral incisors 3, and to close diastemas 11. One of the justifications for its use would be to facilitate the stratification technique of the composite resin on the anterior teeth. However, this technique demands at least two appointments to perform the impression and the waxing.
Additionally, there would be an additional cost of the waxing executed by the prosthetic laboratory. In less extensive cases, such as single diastemas, the free-hand stratification technique may be considered as a viable option. Therefore, it needs to be well reported in the literature and widespread to students and professionals. Additionally, with the improvement of the adhesive restorative dentistry, the current composite resins in association with the adhesive systems have been capable to support greater masticatory efforts in the anterior area without undergoing fracture or displacement. The composite resins still show great optical properties, reproducing not only the color, but also the translucency, texture and brightness of the natural teeth. Currently, the use of materials employing nanotechnology in their development has been an option for aesthetic restorations 2,4,13. Therefore, the knowledge on the materials and instruments employed, the stratification and technique used as well as the systematic training to achieve the predictability and sedimentation of the experience is fundamental. In these situations, the direct adhesive restorative systems with the use of composite resins have been a conservative, fast, low-cost alternative with favorable longevity 8. Thus, the aim of this study was to report, through a clinical case, the free-hand stratification technique of nanoparticulated composite resins in the restorative treatment of the closure of anterior diastemas.
Case report
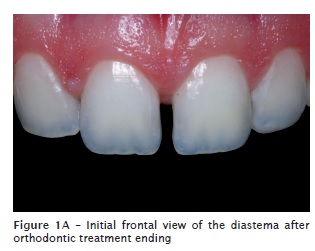
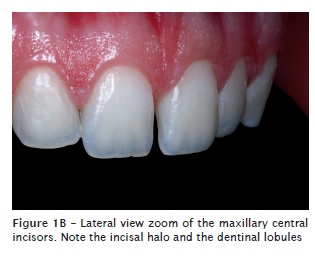
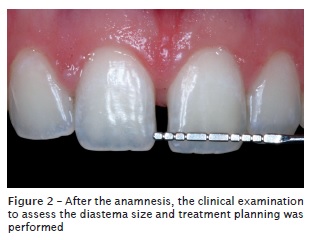
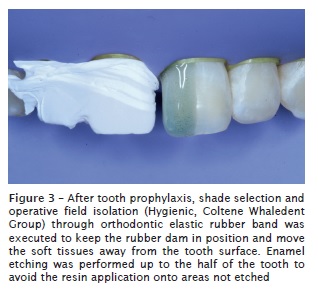
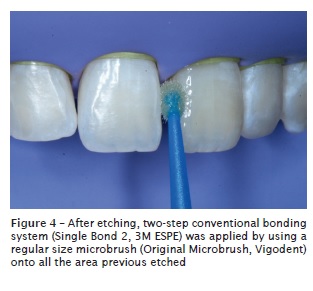
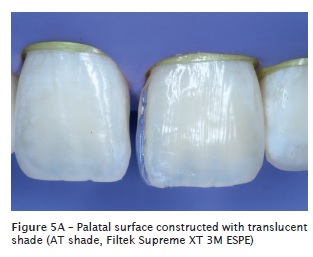
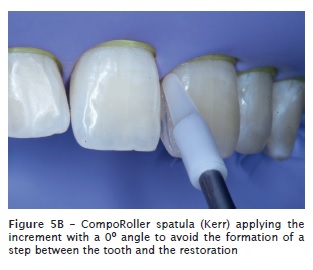
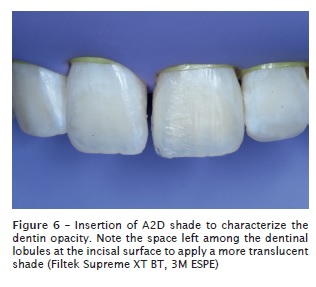
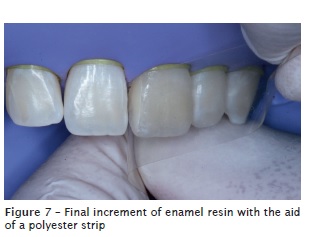
A 21-year-old female patient sought treatment after the ending of the orthodontic treatment. Clinically, the presence of diastemas between the maxillary central incisors was verified (figures 1A and 1B). Also, the clinical normality of the supporting and pulp structures was checked after the anamnesis and radiographic examination. Because the diastema was small, that is, less than 2 mm (figure 2), we opted for the restoration of the teeth employing the direct restorative adhesive system. For that purpose, the teeth were submitted to prophylaxis by pumice and water, and the selection of dentin and enamel shades were performed. The absolute isolation of the operative field was executed by dental rubber dam (Hygienic, Coltene Whaledent Group), kept in place with the aid of orthodontic elastic rubber bands to obtain a gingival displacement from the incisors. A polytetrafluorethylene strip was initially placed onto the right central incisor to avoid the etching of this tooth. The enamel surface was etched by 35% phosphoric acid (3M ESPE) up to the half of the tooth to avoid the application of the resin onto an area not etched (figure 3). Following, the surface was dried by absorbent paper and the bonding agent was applied (Adper Single Bond 2, 3M ESPE) by using a regular size microbrush (Original Microbrush, Microbrush International) (figure 4) and light-curing was performed according to the manufacturer's instructions. The palatal surface was free-hand applied, that is, without the use of a silicone guide, and with the aid of a CompoRoller spatula (Kerr), by using the translucent shade of the resin (Filtek Supreme XT, AT shade, 3M ESPE) (figure 5A). The spatula was inclined to end the restoration at a 0° angle to the enamel surface, therefore avoiding the creation of a step between the tooth and the material (figure 5B). An increment of the A2D shade was applied, leaving a space in the incisal surface to characterize this tooth area (figure 6). A more translucent shade (BT shade, Filtek Supreme XT) was placed onto this area, characterizing the nuance and the translucency of the incisal edge. A single layer of the A2E shade was applied onto the labial surface and spread with the aid of a polyester strip, prior to the final light-curing (figure 7).
Each portion of the composite resin was light-cured through a LED device (Blue Star 3, Microdont) for the time recommended by the manufacturer, continuously, and closest to the area. The same procedures were executed in the right central incisor (figure 8). Immediately after the removal of the absolute isolation, the restoration finishing was carried out with the aid of a size 12 scalpel blade. At this stage, the incisal adjustment was also performed.
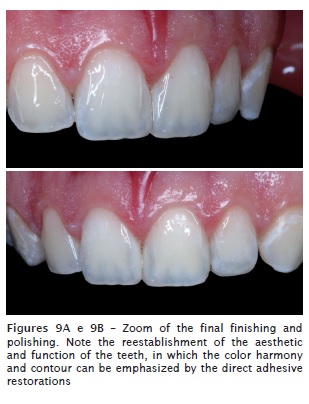
After 24 hours, the final finishing and polishing were executed. Sanding strips (KG Sorensen) were employed onto the interproximal surfaces, while the restoration contours were delimited through abrasive discs at decreasing order (Diamond Pro, FGM). Next, rubber cups (Enhance, Dentsply) and felt discs with polishing paste for composite resins (Diamond Excel, FGM) were used to obtain the final brightness. The final aspect of the restoration can be seen in figures 9A and 9B.

Discussion
To achieve good results in cases of closure of diastemas with predictability, several aspects should be considered. The adequate diagnosis and treatment planning should be firstly weighed 6,8. In cases such the one presented here, the evaluation of the diastema size is fundamental for the decision between the direct and indirect treatment, by employing dental ceramics and even the indication of orthodontic treatment. The diastema presented in the case reported here can be classified as small, that is, size between 0.5 and 2 mm 1. Because of its small extension, the restorative treatment was chosen for this case. Several papers, researches and reports demonstrated satisfactory aesthetical outcomes of composite resins in anterior teeth in the most diverse situations, either in fractures or in closure of diastemas 6,15. The direct adhesive restorative procedures, when compared with the indirect systems, has the advantages of: requiring the minimum weariness of tooth structure 10, showing good clinical durability and being executed faster, because they do not need the laboratorial phase. Additionally, they are reversible procedures of low cost.
During the treatment planning, the decision between direct and indirect restorations should take into consideration the patients age, the aesthetic requirement and the presence of large restorations on the teeth to be restore12. Direct restorations, because of its reversibility, enable new future approaches, without damaging to the remnant tooth structures 3. Good results of both the dentinal bonding agents 7 and composite resins 4 have been reported.
The technique employing the silicone guide demands an extra appointment to obtain the impression, and consequently a higher cost. It can be indicated in larger cases, in which there would be the involvement of multiple teeth. However, in cases such this reported here, the free-hand stratification technique can be favorably and predictably indicated. A detail several times neglected when silicone guides obtained from waxed study casts are used is the cervical adaptation on the cervical area of the palatal surface. It is not uncommon to observe the excess of restorative material on this area when such technique is applied. These excesses favor the plaque accumulation and periodontal disease development. The restorative material employed in this present study has nanoparticles. The materials with this type of particles provide a smoother surface and therefore also favor the outcome after polishing and brushing procedures 13. Nanoparticulated composite resins tend to show a smaller brightness loss and smaller increasing of the superficial rugosity as time goes by 4. Additionally, these composites have also showed smaller solubility values 2, which can favor the restoration longevity.
It is interesting to note that the finishing and polishing procedures of the restored surface depend on the system used, as well as on the type of the restorative material employed 14. Accordingly, the dentists should carefully choose not only the restorative system, but also the finishing and polishing materials with which they have more domain and experience. Periodical following-up appointments should be scheduled, because although a nanoparticulated composite resin was employed, there would be a tendency towards superficial staining and brightness loss. Therefore, the restoration repolishing should be performed when necessary, as time goes by.
References
1. Barrancos-Mooney J. Operatória dental. Buenos Aires: Editorial Médica Panamericana; 1999. [ Links ]
2. Berger SB, Palialol AR, Cavalli V, Giannini M. Characterization of water sorption, solubility and filler particles of light-cured composite resins. Braz Dent J. 2009;20(4):314-8.
3. Boselli G, Pascotto RC. Incisivos laterais conóides: diagnóstico, planejamento e tratamento restaurador direto. Revista Dental Press Estética Maringá. 2007;4(2):111-7.
4. Da Costa J, Adams-Belusko A, Riley K, Ferracane JL. The effect of various dentifrices on surface roughness and gloss of resin composites. J Dent. 2010 Mar 1.
5. Dorland WAN. Dorlands illustrated medical dictionary. 28. ed. Philadelphia: Saunders; 1994994994.
6. Furuse AY, Herkrath FJ, Franco EJ, Benetti AR, Mondelli J. Multidisciplinary management of anterior diastemata: clinical procedures. Pract Proced Aesthet Dent. 2007 Apr;19(3):185-91; quiz 92.
7. Hara AT, Amaral CM, Pimenta LA, Sinhoreti MA. Shear bond strength of hydrophilic adhesive systems to enamel. Am J Dent. 1999 Aug;12(4):181-4.
8. Mondelli J. Estética e cosmética em clínica integrada restauradora. São Paulo: Quintessence; 2003.
9. Mondelli J, Cunha LF, Francischone AC, Coneglian EAC, Ribeiro ZMLR. Restauração da guia anterior com resina composta devido a desgaste dentário patológico. Clínica Int J Braz Dent. 2007;3:36666-72.
10. Mondelli J, Sene F, Ramos RP, Benetti AR. Tooth structure and fracture strength of cavities. Braz Dent J. 2007;18(2):134-8.
11. Pontons-Melo JC, Furuse AY, Freitas CA, Mondelli J. Otimizando la estética en el tratamiento de diastemas. Revista de la Asociación Odontológica Argentina. 2009;9(3):239-43.
12. Rossato DM, Saade EG, Saad JRC, Porto-Neto ST. Coroas estéticas anteriores em cerâmica metal-free: relato de caso clínico. RSBO. 2010;7(4):494-8.
13. Senawongse P, Pongprueksa P. Surface roughness of nanofill and nanohybrid resin composites after polishing and brushing. J Esthet Restor Dent. 2007;19(5):265-73; discussion 74-5.
14. Uctasli MB, Arisu HD, Omurlu H, Eliguzeloglu E, Ozcan S, Ergun G. The effect of different finishing and polishing systems on the surface roughness of different composite restorative materials. J Contemp Dent Pract. 2007;8(2):8989-9696.
15. Watanabe H, Khera SC, Vargas MA, Qian F. Fracture toughness comparison of six resin composites. Dent Mater. 2008 Mar;24(3):418-25.
 Correspondence:
Correspondence:
Leonardo Fernandes da Cunha
Centro Odontológico Brasiliense – Brasília Shopping / SCN Quadra 5 – Bloco A
CEP 70710-500 – Brasília – DF – Brasil
E-mail:cunha_leo@yahoo.com.br
Received for publication: March 11, 2011.
Accepted for publication: June 30, 2011.
