










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Case Report Article
Radix entomolaris – A case report
Felipe Davini I; Rodrigo Sanches Cunha II; Carlos Eduardo Fontana I; Claudia Fernandes de Magalhães Silveira I; Carlos Eduardo da Silveira Bueno I
II Division of Endodontics, Department of Operative Dentistry, University of Manitoba – Manitoba – Canada.
ABSTRACT
Introduction: A comprehensive knowledge on the root canal anatomy is a basic prerequisite for the endodontic treatment successful. Mandibular molars may have an additional root located lingually (radix entomolaris) or buccally (radix paramolaris). In the literature, this anatomy variation is considered rare in Caucasian populations. Awareness and understanding of the presence of unusual external and internal root canal morphology contributes to the successful outcome of the root canal treatment. Objective and case report: The purpose of this study was to report a clinical case of successful endodontic treatment in a mandibular molar with pulp necrosis and characterized as radix entomolaris in which the use of magnification and ultrasonic tips (the microsonics concept) was fundamental to the management of the variations in the internal anatomy. Conclusion: A better understanding of the root canal morphology is essential for endodontic treatment success, as well as the use of technologic advancements in Endodontics including computed tomography, ultrasonic tips and the operating microscope.
Keywords: Endodontics; root canal treatment; morphology.
Introduction
The success of the endodontic therapy depends on the complete cleaning and shaping of the root canal systems, on the tridimensional obturation and on the proper coronary sealing. For that purpose, the knowledge on the morphology of the root canal system as well as its variations may contribute for endodontic treatment success. It is known that the mandibular first molar may display several anatomical variations. Most of the first molars of the Caucasian population exhibit two canals: one mesial and one distal 1; the mesial root has two canals ending into two different apical foramens or, sometimes, these canals are united at the root ending, resulting in a single foramen. The distal root generally shows a large kidney-shape root canal; however, if the orifice is narrow and round, a second distal canal may be present 18. The anatomical variations has been described in the mandibular first molar: Fabra-Campos 9 reported the presence of three mesial canals and Stroner 16 observed the occurrence of three distal canals.
The number of roots may also vary in mandibular molars, in which a third additional root, firstly mentioned in the literature by Carabelli 4, is called radix entomolaris. This supernumerary root is located in distolingual position, mainly in the mandibular first molars. When located in the mesiobuccal surface, the anomaly is called radix paramolaris. The identification and external morphology of this anomaly containing a supernumerary lingual or buccal root, are described by Carlsen and Alexandersen 5.
Although both macrostructures are rare conditions in the Caucasian population, the knowledge on its occurrence is important. The aim of this study was to describe a clinical case of a mandibular first molar with four canals and three roots: one mesiobuccal, one mesiolingual, one distobuccal, and one distolingual (radix entomolaris).
Case report
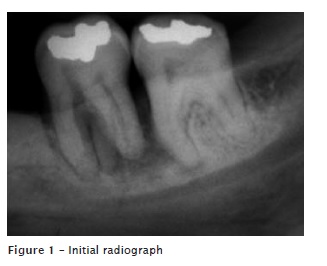
A 34-year-old Caucasian male patient was referred to endodontic treatment of a left mandibular first molar. The tooth exhibited signs and symptoms of pulp necrosis. Clinical examination was executed through the vertical percussion and pulp tenderness to cold, which were negative. In the radiographic examination, a diffuse bone rarefaction was seen due to a chronic apical periodontitis Also, the presence of a third root was observed (figure 1).
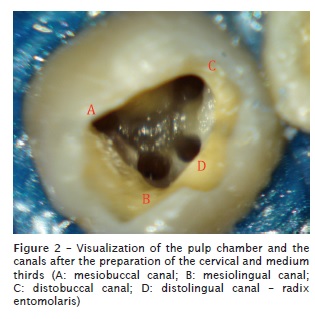
After the anesthesia of the inferior alveolar nerve by 4% articaine + 1:100,000 epinephrine (DFL, Rio de Janeiro, RJ, Brazil), the surgical access and the absolute isolation of the tooth were performed through a dental dam. The canals were negotiated through the aid of a size 15 K hand instrument (Dentsply Maillefer, Ballaigues, Switzerland), after the visual inspection with the aid of an operating microscope (Alliance, São Paulo, SP, Brazil). A dark line was observed between the distal orifice of the canal and distolingual corner of the pulp chamber floor. At this stage, the dentin was removed through diamond-coated ultrasonic tips (size TRA 24, Dental Trinks, São Paulo, SP, Brazil ) mounted in a ultrasonic device (Gnatus, Ribeirão Preto, SP, Brazil), and a second distal orifice of the canal was detected. The enlargement of the cervical and medium thirds through nickel-titanium rotary instruments (ProTaper Universal, sizes S1 and Sx, Dentsply Maillefer, Ballaigues, Switzerland) and Gates-Glidden burs (sizes 4, 3 and 2; Dentsply Maillefer, Ballaigues, Switzerland) was performed, resulting in more visible canals, including the radix entomolaris canal (figure 2).
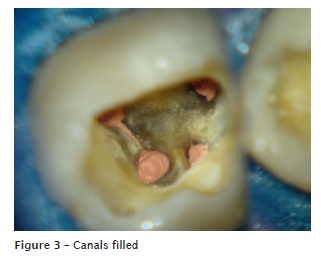
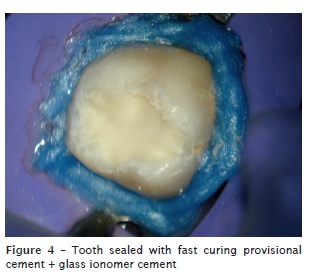
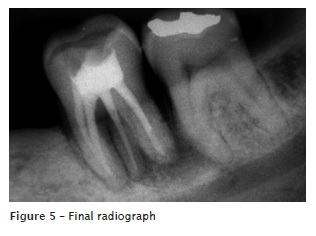
Odontometry was determined through electronic apical locator (Root ZXII. JMorita, Suita City, Osaka, Japan), and the canals were shaped through ProTaper Universal instruments (Dentsply Maillefer, Ballaigues, Switzerland). During cleaning and shaping, the canals were irrigated with 2.5% sodium hypochlorite and 17% EDTA-T (fórmula e ação). Root canal obturation was executed through gutta-percha points and endodontic sealer (AH Plus, Dentsply Maillefer, Ballaigues, Switzerland), by using the continuous wave of condensation (figure 3). The endodontic access was sealed with glass ionomer cement, and the patient was referred to his general dentist to perform the tooth restoration (figures 4 and 5).
Discussion
Prevalence of the radix entomolaris and paramolaris
The presence of a single radix entomolaris in the mandibular first molar has been associated with determined ethical groups. In Black populations, the maximum frequency found is 3% 14, while in Caucasians and Indians, the occurrence is lower than 5% 19. In Chinese, Eskimos, and American Indian population, studies have shown that radix entomolaris occurs in a constancy ranging from 5% to more than 30% 21. Because of its high frequency in these populations, the o radix entomolaris is considered normal (eumorphic root morphology). In Caucasians, the radix entomolaris is not common with maximum occurrence from 3.4 to 4.2%, 6,11. The aetiology behind the formation of radix entomolaris is still uncertain; it can be related to external factors during odontogenesis or to the penetration of an atavic gene or polygenic system (atavism is the reappearance of a trace after several generations of absence). In eumorphic roots, racial genetic factors influenced the deepest expression of a particular gene which results in the most accentuated phenotypic manifestation 12,13. Curzon 7 suggested that the molar of three roots has a high degree of genetic trace penetrance; its domain reflected in the fact of which the trace prevalence was similar in pure Eskimos and in the mixture of Eskimos with Caucasians.
The radix entomolaris may be found in the first, second and third mandibular molar; its less occurrence is in the second molar 20. Some studies reported a bilateral occurrence of radix entomolaris of 50-67% 15,22. Bolk 3 reported the presence of an additional root located at the buccal surface: the radix paramolaris. This macrostructure is very rare and occurs less frequently than the radix entomolaris. The prevalence of the radix paramolaris, as observed by Visser 20, was of 0% for the mandibular first molar, 0.5% for the second molar, and 2% for the third molar. Other studies 5,14, however, reported the radix paramolaris in mandibular first molars.
Morphology of radix entomolaris
The radix entomolaris is located distolingually, with its total or partial coronal third fixed to the distal root. The dimensions of the radix entomolaris varied from a short tapered extension to a mature root with normal length.
In most of the cases, the pulp extension is radiographically visible. Generally, the radix entomolaris is smaller than the disto- and mesiobuccal roots and may be separated from the other roots, or partially fused to them. Visual magnifications, such as magnifying glasses and operating microscopes 10, as well as the use of computed tomography are important tools for the identification of extra canals by the clinicians 1.
Conclusion
The dentist should be aware of this uncommon anatomy in the mandibular first molars of the Caucasian population. The initial diagnosis of either the radix paramolaris or the radix entomolaris before the beginning of the endodontic treatment is important to facilitate the procedures during treatment and avoid the mislocation of any canal. Periapical radiographs executed in the pre-operatory stage with different horizontal angulation help to identify these additional roots. The use of the operating microscope and the modification of the access cavity are also of fundamental importance for the location of the root canal orifice present in this extra root.
References
1. Abuabara A, Schreiber J, Baratto-Filho F, Cruz GV, Guerino L. Análise da anatomia externa no primeiro molar superior por meio da tomografia computadorizada cone beam. RSBO. 2008 Aug;5(2):38-40. [ Links ]
2. Barker BC, Parson KC, Mills PR, Williams GL. Anatomy of root canals. III. Permanent mandibular molars. Aust Dent J. 1974;19:403-13.
3. Bolk L. Welcher Gebißreihe gehören die Molaren an? Z Morphol Anthropol. 1914;17:83-116.
4. Carabelli G. Systematisches Handbuch der Zahnheilkunde. 2. ed. Viena: Braumuller und Seidel; 1844. p. 114.
5. Carlsen O, Alexandersen V. Radix entomolaris: identification and morphology. Scan J Dent Res. 1990;98:363-73.
6. Curzon ME. Three-rooted mandibular permanent molars in English Caucasians. J Dent Res. 1973;52:181.
7. Curzon ME. Miscegenation and the prevalence of three-rooted mandibular first molars in the Baffin Eskimo. Community Dent Oral Epidemiol. 1974;2:130-1.
8. Fabra-Campos H. Unusual root anatomy of mandibular first molars. J Endod. 1985;11:568-72.
9. Fabra-Campos H. Three canals in the mesial root of mandibular first permanent molars: a clinical study. Int Endod J. 1989;22:39-43.
10. Feix LM, Boijink D, Ferreira R, Wagner RH, Barletta FB. Microscópio operatório na Endodontia: magnificação visual e luminosidade. RSBO. 2010 Jul-Sep;7(3):340-8.
11. Ferraz JA, Pecora JD. Three-rooted mandibular molars in patients of Mongolian, Caucasian and Negro origin. Braz Dent J. 1993;3:113-7.
12. Reichart PA, Metah D. Three-rooted permanent mandibular first molars in the Thai. Community Dent Oral Epidemiol. 1981;9:191-2.
13. Ribeiro FC, Consolaro A. Importancia clinica y antropologica de la raiz distolingual en los molars inferiores permanentes. Endodoncia. 1997;15:72-8.
14. Sperber GH, Moreau JL. Study of the number of roots and canals in Senegalese first permanent mandibular molars. Int Endod J. 1998;31:112-6.
15. Steelman R. Incidence of an accessory distal root on mandibular first permanent molars in Hispanic children. J Dent Child. 1986;53:122-3.
16. Stroner WF. Mandibular first molar with three distal canals. Oral Surg. 1984;57:554-7.
17. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod. 1999 Jun;25(6):446-50.
18. Thoden Van Velzen SK, Wesselink PR, De Cleen MJH. Endodontologie. 2. ed. Houtem/Diegem: Bohn Stafleu Van Loghum; 1995. p. 142-3.
19. Tratman EK. Three-rooted lower molars in man and their racial distribution. Br Dent J. 1938;64:264-74.
20. Visser JB. Beitrag zur Kenntnis der menschlichen Zahnwurzelformen. Hilversum: Rotting; 1948. p. 49-72.
21. Walker T, Quakenbush LE. Three rooted lower first permanent molars in Hong Kong Chinese. Br Dent J. 1985;159:298-9.
22. Yew SC, Chan K. A retrospective study of endodontically treated mandibular first molars in a Chinese population. J Endod. 1993;19:471-3.
 Correspondence:
Correspondence:
Felipe Davini
Rua Clóvis Bevilacqua, 243 – Jardim Guanabara
CEP 13073-021 – Campinas – SP – Brasil
E-mail: felipedavini@me.com
Received for publication: October 28, 2011.
Accepted for publication: January 14, 2012.
