










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.3 Joinville Jul./Set. 2012
Case Report Article
The importance of microsonics concept for optimization of endodontic retreatment outcome: a case report
Cláudia Fernandes de Magalhães Silveira I; Carlos Eduardo Fontana I; Felipe Davini I
Roberta Aranha de Araújo Arruda I; Carlos Eduardo da Silveira Bueno I
ABSTRACT
Introduction: During the past few decades, the endodontic treatment has benefited from the development of new techniques and devices, which have improved the outcome and predictability. Important attributes such as the operating microscope and ultrasonics have found indispensable applications in a number of dental procedures in endodontics. Objective and case report: This study describes a case of endodontic retreatment of a maxillary first molar in which the second mesiobuccal canal could be located by extending the access to the mesial direction further than usual and by a closer inspection of the pulp chamber floor. Conclusion: The "microsonics concept" has enhanced the quality of endodontic treatment and retreatment, becoming increasingly more useful in applications such as localization of root canal orifices.
Keywords: Endodontics; endodontic retreatment; morphology.
Introduction
For the endodontic treatment success, the location of all root canals is fundamental for their complete cleaning and shaping, resulting in a hermetic sealing through the filling material 14,20. The localization of extra canals and other anatomic irregularities depend on three main factors: knowledge of the clinician on the probability of the occurrence of additional canals; careful radiographic examination; careful evaluation of the pulp chamber floor through a magnifying device, such as the operating microscope 4,10. In the endodontic practice, computed tomography is a very useful tool in the evaluation of the root canal morphology, its location as well as the visualization of the root morphology 1,5,20,21.
The maxillary molars show extremely complex morphology, presenting in several times a difficult treatment 1,18,19. Thus, this tooth group needs to be minutely evaluated by the professional, preferably under the magnification provided by the operating microscope. The incidence of the fourth canal ranges from 50.4% to 95% 8,13,16,19; the probability of locating a fifth canal is of 2.25% 2, a few authors already reported 6 canals 6,15.
Alaçam et al. 4 compared the localization of a second mesiobuccal canal (MB2) without the use of an operating microscope, with its use and with its association with an ultrasonic device. The results showed the location of MB2 in 62%, 67% and 74% of the teeth, respectively. The use of the ultrasonic device in association with the operating microscope increased the location of MB2 canals when compared with the non-use of the microscope. The sectioning of these teeth revealed the presence of the MB2 canal in 82% of the teeth.
The aim of this study was to report a clinical case of the endodontic retreatment of a maxillary first molar in which the mislocation of the fourth canal during the first intervention accounted for the treatment failure. The knowledge of the clinician together with the available technology was fundamental for the location, cleaning and shaping of all root canal system.
Case report
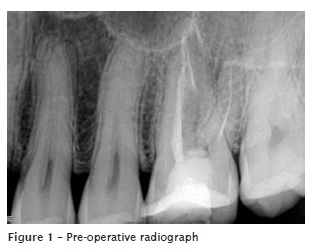
A 43-year-old male patient searched for the endodontic clinic of the São Leopoldo Mandic School of Dentistry and Center of Dentistry Researches of Campinas (SP, Brazil), reporting intermittent pain in the left maxillary first molar (tooth #26) during mastication. The patient informed that this tooth had already undergone endodontic treatment two years ago. The clinical examination revealed moderate pain to percussion in this tooth and no tenderness to palpation. The radiographic examination showed the deficient filling of the canals (figure 1). The tooth presented a composite resin restoration. Based on this history and on the clinical and radiographic examinations, the diagnosis of symptomatic apical periodontitis was established. The patient was informed about the necessity of the root canal retreatment.
After the anesthesia of the tooth, the restorative material was removed, and the absolute isolation and initial irrigation with 2.5% sodium hypochlorite (Biodinâmica Química e Farmacêutica Ltda., Ibiporã, PR, Brazil) was performed. A small correction in the surgical access was necessary, aiming to expose better the mesiobuccal canal orifice.
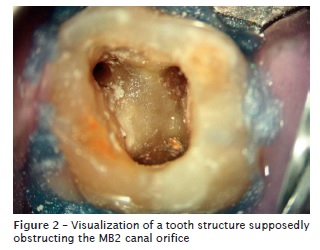
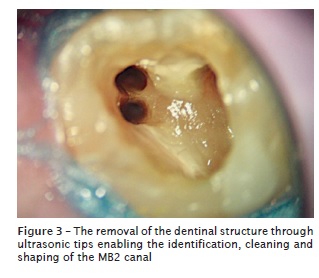
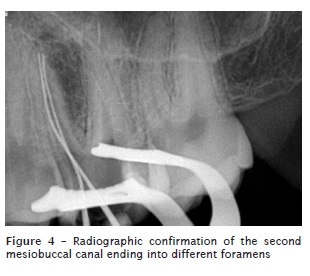
During the examination through operating microscope (Alliance, São Paulo, SP, Brazil), three canal orifices were found. With the aid of ultrasonic tips (size TRA 24, Dental Trinks, São Paulo, SP, Brazil) mounted into an ultrasound device (Gnatus, Ribeirão Preto, SP, Brazil), the access was rectified, and the structure which supposedly obstructed the MB2 canal orifice was removed, enabling the location of the MB2 canal (figures 2 and 3). The canals were negotiated through K type files (Dentsply Maillefer, Ballaigues, Switzerland ) and the following chemical-mechanical preparation was executed through ProTaper Universal rotary instruments (Dentsply Maillefer, Ballaigues, Switzerland). At this same appointment, the desobturation of the cervical and medium thirds of the mesiobuccal, distobuccal, and palatal canals with the aid of a ultrasonic tip (size TRA 12) and Gates-Glidden burs (size 4, 3 and 2). Next, a rotary system (ProTaperD, Dentsply Maillefer, Ballaigues, Switzerland), to complement the desobturation of the cervical, medium and apical thirds (D1, D2 and D3, respectively; D1 instrument at 500 rpm; D2 and D3 at 400 rpm, all at torque 4). The procedure was concluded with the insertion of a size 15 within all the extension of the canals. The electronic odontometry was performed by using a electronic apex locator (Root ZX II, J Morita, Suita City, Osaka, Japan) and a radiograph through hand files put in position to identify the canals (figure 4).
The instrumentation of the canals was executed through rotary instruments (ProTaper Universal, Dentsply Maillefer, Ballaigues, Switzerland). During the cleaning and shaping process, irrigation was executed by 2.5% sodium hypochlorite (Biodinâmica Química e Farmacêutica Ltda., Ibiporã, PR, Brazil). The last irrigation was performed through 17% EDTA (Fórmula & Ação, São Paulo, SP, Brazil), passively agitated through ultrasonic tips (size TRA 12, Dental Trinks, São Paulo, SP, Brazil) for 1 minute, followed by a final irrigation with 2.5% sodium hypochlorite (Biodinâmica Química e Farmacêutica Ltda., Ibiporã, PR, Brazil).
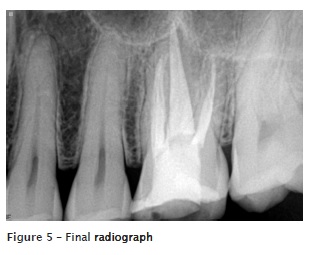
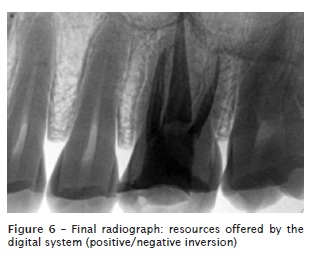
The obturation occurred by Taggers hybrid technique, which comprises the lateral condensation and McSpadden condensers (Dentsply Maillefer, Ballaigues, Switzerland), with gutta-percha and endodontic sealer (AH Plus, Dentsply DeTrey, Konstanz, Germany) (figures 5 and 6). The surgical access was sealed with composite resin, and the patient referred to the restorative treatment.
Discussion
In this clinical case, the mislocation of the second root canal in the mesiobuccal root led to the first treatment failure, a situation already cited by some literature reports. This deficiency was supplied, posteriorly, by the endodontic retreatment, which allied the technology provided by the microsonics concept for the complete cleaning and shaping of all root canal system 7,17.
With the advent of the operating microscope, the clinical procedures have been better conducted, mainly by the visual magnification and by the increasing of the luminosity provided by the device. Several procedures, during the endodontic treatment, such as the access and location of the canals, became more predictable, through the use of this device 4,12,20.
The surgical access or crown opening should be performed in a way that it allows the direct access to root canal. The clinician should be capable of visualizing all aspects of the coronal third of the root canal system, by the removal of all tooth structure or restorative material that may interfere in the straight access 4,18. To obtain such access, the conventional triangular access cavity can be modified into several shapes, such as trapezoidal 3,11,19, rectangular 9, rhomboidal 18 and ovoid 8, depending on each clinical situation. In this present study, the conventional triangular access was initially performed, being posteriorly modified to negotiate the extra canals. The variations of the root canal system constitute a continuous challenge for the endodontist, and the endodontic treatment success is related to the domain of such anatomy by the clinician.
Conclusion
Based on this clinical case, it can be concluded that the high level of magnification and illumination provided by the use of the operating microscope make easy the location of the second canal in the mesiobuccal root of the maxillary molars, as well as the employment of the ultrasonic tips for the removal of small dentin structures which may obstruct the canal orifices. The modification of the surgical access can be of great value for the location and, consequently, for the endodontic treatment success.
References
1. Abuabara A, Schreiber J, Baratto-Filho F, Cruz GV, Guerino L. Análise da anatomia externa no primeiro molar superior por meio da tomografia computadorizada cone beam. RSBO. 2008 Aug;5(2):38-40. [ Links ]
2. Acosta Vigouroux SA, Trugeda Bosaans SA. Anatomy of the pulp chamber floor of the permanent maxillary first molars. J Endod. 1978 Jul;4:214-9.
3. Aggarwal V, Singla M, Logani A, Shah N. Endodontic management of a maxillary first molar with two palatal canals with the aid of spiral computed tomography: a case report. J Endod. 2009 Jan;35(1):137-9.
4. Alaçam T, Tinaz AC, Genç O, Kayaoglu G. Second mesiobuccal canal detection in maxillary first molars using microscopy and ultrasonics. Aust Endod J. 2008 Dec;34(3):106-9.
5. Bauman R, Scarfe W, Clark S, Morelli J, Scheetz J, Farman A. Ex vivo detection of mesiobuccal canals in maxillary molars using CBCT at four different isotropic voxel dimensions. Int Endod J. 2011 Aug;44(8):752-8.
6. Bond JL, Hartwell G, Portell FR. Maxillary first molar with six canals. J Endod. 1988 Feb;14(5):258-60.
7. Cunha RS, Davini F, Fontana CE, Miguita KB, Bueno CES. O conceito microsonics: primeiro molar superior com cinco canais – relato de caso. RSBO. 2011 Apr-Jun;8(2):231-5.
8. Fogel HM, Peikoff MD, Christie WH. Canal configuration in the mesiobuccal root of the maxillary first molar: a clinical study. J Endod. 1994 Mar;20(3):135-7.
9. Ghoddusi J, Naghavi N, Zarei M, Rohani E. Mandibular first molar with four distal canals. J Endod. 2007 Dec;33(12):1481-3.
10. Hülsmann M. A maxillary first molar with two disto-buccal root canals. J Endod. 1997 Nov;23(11):707-8.
11. Iqbal M, Fillmore E. Preoperative predictors of number of root canals clinically detected in maxillary molars: a PennEndo Database study. J Endod. 2008 Apr;34(4):413-6.
12. Kottoor J, Velmurugan N, Surendran S. Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning: a case report. J Endod. 2011 May;37(5):715-9.
13. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod. 1990 Jul;16:311-7.
14. Maggiore F, Jou YT, Kim S. A six-canal maxillary first molar: case report. Int Endod J. 2002 May;35(5):486-91.
15. Martínez-Berna A, Ruiz-Badanelli P. Maxillary first molars with six canals. J Endod. 1983 Sep;9(9):375-8.
16. Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol. 1972 Jan;33:101-10.
17. Plotino G, Pameijer CH, Grande NM, Somma F. Ultrasonics in endodontics: a review of the literature. J Endod. 2007 Feb;33(2):81-95.
18. Stropko JJ. Canal morphology of maxillary molars: clinical observations of canal configurations. J Endod. 1999 Jun;25(6):446-50.
19. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J. 1993 Sep;26:257-67.
20. Verma P, Love RM. A micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. Int Endod J. 2011 Mar;44(3):210-7.
21. Zhang R, Wang H, Tian YY, Yu X, Hu T, Dummer PM. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J. 2011 Nov;44(11):990-9.
 Correspondence:
Correspondence:
Cláudia Fernandes de Magalhães Silveira
Rua Pilar do Sul, 429 – Chácara da Barra
CEP 13093-757 – Campinas – SP – Brasil
E-mail:claudinhasilve@gmail.com
Received for publication: November 11, 2011.
Accepted for publication: December 12, 2011.
