










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.4 Joinville Out./Dez. 2012
Original Research Article
Comparison of the sealing ability of different types of glass ionomer cements in temporary restoration
Thiago Vitelli Vasco dos Santos I ; Cleber Keiti Nabeshima I ; Mariana Cavatoni I ; Maria Leticia Borges Britto I
ABSTRACT
Introduction: Glass ionomer cement has been used for temporary restoration; however, several formulations are available. Objective: The aim of this study was compare the linear leakage of different types of glass ionomer cement – R, F, N and C. Material and methods: Forty-four third molars were used and prepared with standardized class I cavity preparations. By using gutta-percha, the cavity height was standardized in 5 mm. The samples were divided into 4 experimental groups (R, N, F and C), and 2 control groups (positive – not restored, and negative – restored using resin). The teeth were waterproofed and immersed in 2% methylene blue. After 7 days, they were sectioned and the measurement of the dye leakage was performed by stereomicroscopy (40X) using a calibrated periodontal probe. Results: Data were analysed by Kruskal Wallis and Dunn tests. There was statistically significant differences (p = 0.002) between R and C, and R and N glass ionomer groups. C and N glass ionomer groups were similar. F glass ionomer group was similar to all other groups. Conclusion: It can be concluded that different types of glass ionomer formulations can influence the peripheral sealing of the restorative material. R glass ionomer was the most effective, while C and N glass ionomers were the least ones.
Keywords: glass ionomer cements; tooth leakage; temporary restoration.
Introduction
The success of the endodontic treatment is closely linked to the maintenance of the disinfection obtained by the chemical-surgical preparation. Studies have reported the periapical development of bacterias 24 hours after the root canal exposure to them 7, therefore justifying the provisional restoration between the appointments.
In this context, zinc oxide and eugenol cement is among the most used materials 19 and exhibits excellent properties of resistance to compression 10; however, it presents high marginal leakage rate 1,4. On the other hand, glass ionomer cement has also been used for temporary restoration 19; it shows high bonding to dentin 17, great resistance to abrasion, and low solubility 11; it exhibits smaller microleakage values when compared with zinc oxide eugenol cement 3,15,20, fluoride release 2 and thermal-linear expansion coefficient similar to the tooth structure.
By comparing microleakage between glass ionomer cements commercialized both in Brazil (Vidrion) and worldwide revealed that the Brazilian trademarks has better sealing capacity with lower cost than worldwide ones 5.
The Brazilian glass ionomer cement is presented in four different specific formulations (R, F, N, and C) for specific indications (restoration, liner, filling and cementation).
The literature reports assessments of teeth restored Vidrion R comparing it with other restorative materials 14,16,18. Also, assessments among restorations performed with other formulations of this material: cementation formulation – Vidrion C 9,13 and N 12,14 have been carried out, however, contradicting its indication. Notwithstanding, there were not studies comparing them.
Thus, the aim of this study was to compare the microleakage of different types of glass ionomer cement (R, F, N and C) during the sealing of endodontic access cavities.
Material and methods
After the approval of the Ethical Committee on Research (protocol number 100/2011), 44 molars with crowns of similar sizes were kept in saline solution (LBS Laborasa, São Paulo, SP, Brazil) for hydration until the moment of its use. The specimens were washed in running water, and an access surgery was standardized as a class I cavity preparation by using a size 1014HL diamond bur (KG Sorensen, São Paulo, SP, Brazil) and Endo-Z bur (Dentsply-Maillefer, Ballaigues, VD, Switzerland). The deepness of the pulp cavity was measured through millimetric periodontal probe (Trinity, São Paulo, SP, Brazil), and with the aid of a size 4 Paiva's condenser (JER, Belo Horizonte, MG, Brazil) the gutta-percha stick (Dentsply, Petrópolis, RJ, Brazil) was inserted and heated toward the pulp floor, resulting in a 5 mm deep cavity.
The samples were randomly divided into four groups of ten specimens each; and each group was restored with different types of glass ionomer:
• Group 1 – glass ionomer cement – restorative type - R (Vidrion R, SSWhite, Rio de Janeiro, RJ, Brazil);
• Group 2 – glass ionomer cement – filling type to intraradicular post - N (Vidrion N, SSWhite, Rio de Janeiro, RJ, Brazil);
• Group 3 – glass ionomer cement – cementation type – C (Vidrion C, SSWhite, Rio de Janeiro, RJ, Brazil);
• Group 4 – glass ionomer cement – liner type – F (Vidrion F, SSWhite, Rio de Janeiro, RJ, Brazil).
The negative control group was composed by two teeth restored with resin composite (TPH, Dentsply, Petrópolis, RJ, Brazil) and covered with a layer of cyanoacrylate adhesive (Superbonder, Henkel, Jacareí, SP, Brazil); the positive control group was composed by two teeth which were not restored.
All root surface and the apex was sealed with two layer of colorless nail polish (Impala, Porto Velho, RO, Brazil). Next, the teeth were immersed in 2% methylene blue (O Graal Farmácia de Manipulação, São Paulo, SP, Brazil) for seven days at 37ºC.
Following, the teeth were washed in running water to eliminate the dye excess and then cut at the mesial-distal direction through a sulcus on the enamel and cement by using a size 1062 diamond bur (KG Sorensen, São Paulo, SP, Brazil) at high speed and through a sulcus on dentin by using double-face diamond discs (KG Sorensen, São Paulo, SP, Brazil) at low speed.
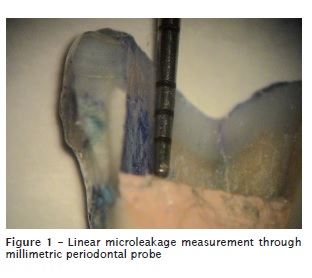
With the aid of an endodontic explorator (JER, Belo Horizonte, MG, Brazil), the restorative material was removed and all cavity surface was analyzed through operating microscope (DF Vasconcellos, São Paulo, SP, Brazil) at x40 magnification. The linear microleakage was measured with the aid of a millimetric periodontal probe by using the occlusal edge as the initial landmark up to the longest point of leakage towards the apical direction (figure 1).
Data were tabulated and submitted to normality test, Kruskal Wallis test, and Dunn test for comparison among groups, with level of significance set at 5%.
Results
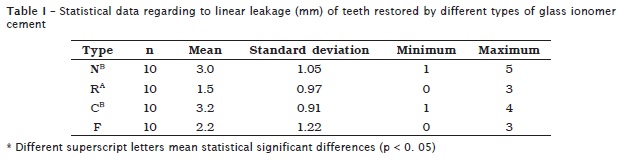
The analysis of linear leakage data showed statistically significant differences (p = 0.002) between Vidrion R and C, and Vidrion R and N. Vidrion C and N were statistically similar. Vidrion F was similar to all other groups. Statistical data can be seen in table I.
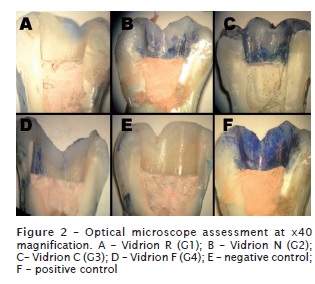
The images representing each group can be seen in figure 2.
Discussion
The search for an appropriate material to seal an endodontic access cavity is still an issue little studied by the research community, nowadays1,3,10,15,16,18,20. Glass ionomer cement has been shown among the most used temporary material 19; however, its modified formulation leads to different types of cements with different indications.
The simpler chemical composition of glass ionomer powder comprises sodium and calcium fluorsilicate and polyacrylic acid, which represents the cementation type material (C). The liner type glass ionomer cement (F) is composed by the addition of barium sulphate and ferric oxide pigment; the restorative type (R) has the ferric oxide replaced by a pigment ranging according to the color desired; the filling type of intraradicular post (N) has the most different formulation, comprising the F type formulation added by silver, copper, tin and zinc. For all types, the liquid composition is the same – tartaric acid and distilled water.
Considering the above informat ion, we hypothesized whether the different formulations would inf luence on the sealing ability of the material when used for sealing the endodontic access cavity.
This present study employed third molars because of their easiest obtainment when compared with other teeth. The standardization of a class I cavity preparat ion for the access surgery was proposed so that different types of cavity preparations would not interfere in the results. The methylene blue dye was chosen because of its recurrent use in studies found in the literature 1,3-6,12-14,20. Also, it is a dye which results in well-defined evidences at the penetration site; it is of ease obtainment and of low cost. It is known that methylene blue favors the reading of marginal leakage when compared to rhodamine-B, which demands activation by ultraviolet radiation for either simple reading or reading through epifluorescent microscope with special filters 15.
The use of a temporary material thickness of 5 mm followed studies in which was observed a better effectivity of the provisional sealing thickness of 4 mm, and in which thickness smaller than 3 mm showed more leakage results 8,21.
The cutting of the samples provided the analysis of all cavity walls without losing any of them, resulting in a more precise assessment of the level of the linear leakage.
The results confirmed the hypothesis that the formulation affects the sealing ability. The best results were verified with Vidrion R, which is indicated by direct restorations. Despite of the lack of studies comparing different types of glass ionomer cement (regarding to their indication), the R type is predominantly among them in literature 3,5,6,11,15,16,18,20. However, there is a great variety among the results because Raggio et al. 14, Ramos and Galn 15 and Pieper et al. 11 observed a good sealing quality of Vidrion R; and Formolo et al. 6 and Seixas et al. 18 found unfavorable results for this same product. Such disagreement among the results could be attributed to the assessment method; most of these studies used scores 5,11,14,15,18, which were subjective interpretations influencing on the results. The findings of this present study showed a leakage mean of 1.5 mm, which is considered small and superficial in this group. In some samples, none dye leakage was observed in all extension of the cavity and surfaces. This value is in agreement with the findings of Valera et al. 20, who found a linear leakage mean of 1.44 mm for the group restored with Vidrion R. Notwithstanding, these findings disagree with those of Ribeiro et al. 16, who observed a mean of 5.7 mm, and those of Couto et al. 3, with mean of 3.41 mm. These differences could be explained due to methodological variations in the studies. Ribeiro et al. 16 obtained very high numbers, however, the authors performed the waterproofing of the specimens by leaving 3 mm of the coronal portion of the root remnant free of protection; this could have allowed the dye access through the dentinal tubules exposed. On the other hand, Couto et al. 3 employed an experimental time period of 21 days, which is three times the time used by this present study.
Concerning to the other groups, Vidrion F showed an intermediary mean value of 2.2 mm; none sample was capable of reaching the limit value to reach the pulp chamber.
Vidrion N, with mean value of 3 mm, showed values close to those of Vidrion C, with higher values of linear leakage. This finding is not in agreement with those found by Pilatti et al. 12 and Raggio et al. 14, who observed little leakage in their studies. This can be again explained by the experimental time period: 48 and 4 hours, respectively, and by the subjective assessment by scores. Another factor that should be taken into consideration is that Raggio et al. 14 employed class V cavity preparations, while this present study used class I preparations.
Vidrion C showed the worst results with leakage values greater than the other types of the material: 90% of the samples had leakage values of 3mm or more for the limit value of 5 mm. These results could be likely attributed to its simpler formulation; the other types of the material contain metallic components added to their formula. The C type shows a more fluid consistency, making it difficult to insert into the cavity, which may also contribute to these results.
It is worth noting that all specimens were immersed into the dye for seven days, which is the mean amount of time between two endodontic appointments. In these conditions, few samples would have reached very closer to the pulp chamber, which occurred only in Vidrion N or C groups. Notwithstanding, although the results showed better results for the other groups, it cannot be affirmed that these would be the same for longer time periods. Therefore, further studies are necessary to provide better information on the influence of different formulations of glass ionomer cement on the sealing ability of endodontic access surgery cavities for longer time periods.
Considering the results of this present study, we recommend that the dentists be alerted regarding to the specific indications of all types of glass ionomer cements, which may influence on the final quality of the product.
Conclusion
According to the results obtained by this present study, it can be concluded that the different formulations of glass ionomer cement may influence on the peripheral sealing ability of the temporary restoration. Considering the immersion time period of seven days, R type was the most effective and the C and N types the least ones.
References
1. Bitencourt PMR, Britto MLB, Nabeshima CK. Comparação da qualidade de selamento periférico de diferentes materiais restauradores provisórios. Rev Odontol UNICID. 2010;22(3):223-8. [ Links ]
2. Carvalho AS, Cury JA. Liberação de flúor de materiais restauradores. Rev Odontol Univ São Paulo. 1998;12(4):357-73.
3. Couto PHA, Pinheiro JMM, Couto LHA, Freitas MRLS. Avaliação in vitro da microinfiltração coronária de cinco materiais seladores temporários usados em Endodontia. Arq Bras Odontol. 2010;6(2):78-88.
4. Fachin EVF, Perondi M, Grecca FS. Comparação da capacidade de selamento de diferentes materiais restauradores provisórios. RPG. Rev Pós-Grad. 2007;13(4):292-8.
5. Ferreira FM, Vale MPP, Jansen WC, Paiva SM, Pordeus IA. Performance of brazilian and imported glass ionomer cements used in atraumatic restorative treatment (art) regarding microleakage in primary molars. J Appl Oral Sci. 2006;14(5):312-8.
6. Formolo E, Sartori A, Demarco FF. Infiltração marginal em cavidades de classe V com o uso de diferentes materiais adesivos. RPG. Rev Pós-Grad. 2001;8(4):306-12.
7. Imura N, Otani SM, Campos MJA, Jardim EG, Zuolo ML. Bacterial penetration through temporary restorative materials in root-canal-treated teeth in vitro. Int Endod J. 1997;30:381-5.
8. Kampfer JTN, Göhring T, Zehnder M, Zehnder A. Leakage of food-borne Enterococcus faecalis through temporary fillings in a simulated oral environment. Int Endod J. 2007;40:471-7.
9. Matsumura OS, Imparato JCP, Camargo MCF, Franco AEA. Utilização dos cimentos de ionômero de vidro no selamento de molares em erupção. Rev Odontopediatr. 1997;5(2):49-53.
10. Mota KS, Britto MLB, Nabeshima CK. Comparação da r e s i s t ênc ia de c imentos restauradores provisór ios ut i l izados em Endodontia. Rev ABO Nac. 2011;19(3):160-4.
11. Pieper CM, Zanchi CH, Rodrigues-Junior SA, Moraes RR, Pontes LS, Bueno M. Sealing ability, water sorption, solubility and toothbrushing abrasion resistance of temporary filling materials. Int Endod J. 2009;42:893-9.
12. Pilatti GL, Zardo M, Queirós AJG. Estudo "in vitro" da microinfiltração apical em retrobturações. Uma avaliação de diferentes materiais utilizados. Rev Paul Odontol. 1994;5:39-44.
13. Pinheiro CC, Santos FS, Scelza MFZ. Estudo comparativo da infiltração marginal frente a alguns materiais restauradores provisórios. RBO. 1997;54(2):59-63.
14. Raggio DP, Rocha RO, Imparato JCP. Avaliação da microinfiltração de cinco cimentos de ionômero de vidro utilizados no tratamento restaurador atraumático (TRA). J Bras Odontopediatr Odontol Bebê. 2002;5(27):370-7.
15. Ramos AA, Galn Jr. J. Infiltração marginal de cimentos provisórios em dentes tratados endodonticamente. RGO. 2004;52(4):305-8.
16. Ribeiro FC, Oliveira FZ, Castro GC, Pimentel KA, Pereira RS, Roldi A et al. Análise in vitro da eficácia do selamento cervical, empregando diferentes materiais restauradores sobre canais radiculares endodonticamente tratados. UFES Rev Odontol. 2008;10(1):27-32.
17. Sá FC, Nolasco GAB, Cesar JA, Sá RS, Dias P. Avaliação da resistência de união interfacial entre diferentes cimentos de ionômero de vidro e resina composta, usando três sistemas adesivos. Semina Ciênc Biol Saúde. 2005;26(1):47-64.
18. Seixas FH, Martinelli DF, Cecchin D, Ribeiro RG, Silva RS, Pécora JD. Avaliação ex vivo da microinfiltração marginal coronária de restauradores provisórios usados em Endodontia. RFO UPF. 2008;13(3):31-5.
19. Vágula MP, Pedott MM, Guimarães MRFSG, Aleixo RQ, Borré MAM. Avaliação da ação antimicrobiana dos materiais seladores temporários utilizados pelos cirurgiões dentistas de Ouro Preto do Oeste – RO. Saber Científ Odontol. 2010;1(1):21-30.
20. Valera MC, Camargo CHR, Teixeira AU, Camargo SEA. Microinfiltração de materiais restauradores temporários usados durante o clareamento dental interno. Ciênc Odontol Bras. 2007;10(4):26-31.
21. Weston CH, Barfield RD, Ruby JD, Litaker MS, McNeal SF, Eleazer PD. Comparison of preparation design and material thickness on microbial leakage though Cavit using a tooth model system. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105(4):530-5.
 Correspondence:
Correspondence:
Cleber Keiti Nabeshima
Av. Amador Bueno da Veiga, n. 1.340 – Penha
CEP 03636-100 – São Paulo – SP – Brasil
E-mail: cleberkn@hotmail.com
