










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.9 no.4 Joinville Out./Dez. 2012
Case Report Article
Persistent infection in root-filled tooth: an SEM morphological analysis after apical microsurgery
Rina Andréa Pelegrine I ; Carlos Eduardo Fontana I ; André Antonio Pelegrine II ; Alexandre Sigrist De Martin I ; Flávia Casale Abe I ; Roberta Aranha de Araujo I ; Carlos Eduardo da Silveira Bueno I
II Department of Implantology, São Leopoldo Mandic Center of Post-Graduation – Campinas – SP – Brazil
ABSTRACT
Introduction and Objective: Endodontic failure can be associated to well-conducted treatments due to microbial factors characterized by intra or extraradicular infections not eliminated during endodontic treatment. Case report: This report describes a case of persistent apical periodontitis of an asymptomatic maxillary lateral incisor endodontically retreated and subsequently subject to apical surgery. Conclusion: After SEM morphological analysis of the apical fragment, areas of cementum-dentin resorption that were probably responsible for the perpetuation of the disease process were observed.
Keywords: apical periodontitis; apical surgery; retreatment.
Introduction
The role of the microorganisms in the pulp pathology and periapical tissues has been reported since the classic study of Kakehashi et al. 6 and increasingly continued to be target of researches 5,8,11-14,17. Cleaning and shaping concepts and anatomical knowledge have been currently associated with new technical resources aiming to obtain the effective decontamination of the root canal systems and to reach the excellence in Endodontics. However, the literature has shown that the endodontic failure may be related to well-conducted treatments, because of the presence of bacterias localized in areas of isthmuses, ramifications, deltas, irregularities and dentinal tubules are not eliminated by the endodontic procedures of disinfection 13. Persistent microorganisms may also be present in areas of resorption of apical cementum and periapical tissues 2,10, decisively contributing for the endodontic therapy failure. Organized in biofilms adjacent to the apical foramen, these microorganisms show high resistance both to antimicrobial agents and to the defense mechanisms of the host 16, therefore making easy the perpetuation of the periradicular pathological processes. According to Siqueira Jr. 13, the development of a non-surgical strategy to fight the apical biofilm is questionable, and therefore the apical surgery is indicated when the periradicular infections persist.
This report describes a case of persistent apical periodontitis in a asymptomatic maxillary lateral incisor, which was endodontically retreated and failed, followed by the surgical approach.
Case report
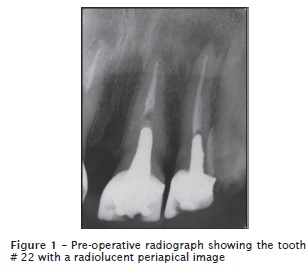
A male, 35-year-old patient, without pain complaint was referred to the evaluation of the left maxillary lateral incisor. The clinical analysis indicated the lack of tooth mobility, pain to vertical percussion and to palpation. The pre-operative radiograph evidenced periapical radiolucency (figure 1), suggesting a chronic apical periodontitis. The back history indicated that the tooth had undergone endodontic treatment 10 years ago. The quality of the endodontic obturation was considered as unsatisfactory and the post and core was maladapted. Consequently, the endodontic retreatment and the removal of the post and core was indicated.
The patient was informed that the conventional endodontic retreatment and the clinical/radiograph following-up would be the approaches of choice. However, the persistence of the lesion after 1 year of following-up led to the execution of the apical endodontic surgery to complement the procedure. The patient agreed with the treatment planing.
Conventional endodontic retreatment
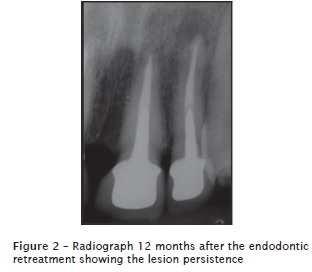
After local anesthesia (2% lidocaine with 1:1000.000 epinephrine), the crown and the post and core were removed through ultrasound device (5AE model– Gnatus, Rio de Janeiro, Brazil). After absolute isolation with rubber dam, the endodontic filling was removed with the aid of an operating microscope (Alliance, São Paulo, Brazil) and the ProTaper D system (Dentsply, Ballaigues, Switzerland). The endodontic retreatment was performed using ProTaper Universal system (Dentsply, Ballaigues, Switzerland), under constantly irrigation with 5.25% sodium hypochlorite (Fórmula e Ação, São Paulo, Brazil). Once the instrumentation was concluded, 17% EDTA solution (Fórmula e Ação, São Paulo, Brazil) was used for 3 minutes associated with ultrasound vibrations to remove the smear layer. The root canal was dried with sterilized absorbent paper points and filled with gutta-percha points (Dentsply, Petrópolis, Brazil) and Endomethasone sealer (Septodont, Saint-maurdes- Fossés, France) using the continuous-wave condensation technique. After the endodontic retreatment, the tooth received a new post and core and porcelain crown. Figure 2 shown the radiograph 1 year after the retreatment, evidencing the persistence of the periapical radiolucency. The apical microsurgery was indicated.
Apical microsurgery
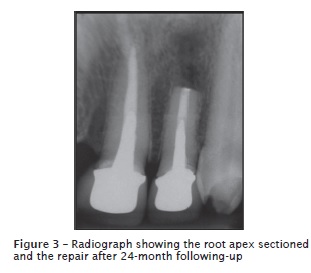
Prior to the surgical procedure, the oral cavity antisepsis with 0.2% chlorhexidine gluconate (Siafarma, Campinas, São Paulo, Brazil) was performed. After the local anesthesia (2% lidocaine with 1:100.000 epinephrine) and incision, a mucoperiosteal flap was raised. The periapical pathology was detected at the radicular apex with cortical bone fenestration. The bone window was enlarged and the periapical tissues curetted. Three millimeters of root apex was resected orthogonally to the longitudinal axis using a carbide bur (Dentsply, Ballaigues, Switzerland) under 0.9% sodium chloride solution irrigation (Baxter, São Paulo, Brazil). The apical fragment was removed and washed with saline solution for posterior analysis in scanning electronic microscopy (SEM). The root retropreparation was performed using an ultrasonic tip (TRA21 D – Trinks, São Paulo, Brazil) with the aid of operating microscope and subsequently filled with MTA (Angelus, Londrina, Brazil). The flap was repositioned and sutured with 5-0 nylon thread. Antibiotics and analgesics were provided to the patient (amoxicillin 500 mg, 3 times a day for 5 days, and ibuprofen 600 mg for pain, 2 times a day as needed). The patient was instructed regarding post-operative care and returned 1 week later for suture removal. The clinical and radiograph followingup was performed from 6 to 24 months, without symptomatology; and the repair of the periapical area was observed (figure 3).
Scanning electronic microscopy
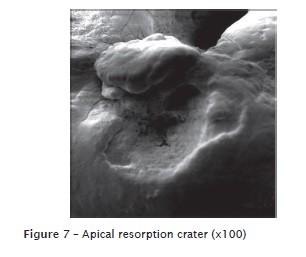
The root fragment removed during the surgery was submitted to metallization (figure 4) to reduce the artifacts, and the root apex surface was studied under SEM at 15 kV (Zeiss DSM 940 A, Oberkochen, Deutschland). The magnifications allowed to observe the apical foramen, apical foramina and apical resorption crater (x50) (figure 5); the apical foramen (x100) (figure 6) and apical resorption crater (x100) (figure 7).



Discussion
The main cause of endodontic failure is the persistence of the microbial infection in the root canal system and/or periradicular area 9,10. Facing the apical periodontitis persistence, the non-surgical endodontic retreatment and the apical surgery constitute treatment approaches, each one with its specific indication. Allgayer and Vanni 1 affirmed that the conventional endodontic retreatment should be cautiously indicated after an accurate evaluation of its benefits and risks. In this present clinical case, the endodontic retreatment was indicated because the initial endodontic treatment was unsatisfactory after the radiographic analysis, presenting failures in the compaction of the filling material and lack of adaptation of the post and core.
According to Danin et al. 3, the apical surgery should be the treatment of choice in cases of the primary endodontic treatment failure or retreatment. The apical surgery aims to remove the altered and damaged periapical tissues and to promote the sealing of the apical root portion, facilitating the regeneration of soft and hard tissues, including the formation of new attachment cells 18. After 1-year following-up and the evidence of the lesion persistence, the apical surgery associated with the operating microscopy was indicated, based on the aforementioned literature. The operating microscope together with the endodontic surgery considerably contributes for the achievement of best treatment results 4,15.
In this present case report, 3mm of the apical fragment was removed. The need of removing the root apex is imperative, because the most part of the apical ramifications and lateral canals is located there 7.
The SEM morphological analysis evidenced an extensive area of dentin-cementum resorption, which possibly contained microorganisms unachievable for the endodontic procedures of disinfection. According to Tronstad et al. 16, endodontic treatment failure may be attributed to the presence of extraradicular infection and microorganisms, which are surrounded by an extracellular matrix and protected from the defense system of the host and systemic antimicrobial therapies.
Conclusion
Areas of apical root resorption favor the extraradicular biofilm formation and contribute for the perpetuation of the periapical pathology. Endodontic microsurgery proved to be a successful a lternat ive in the resolut ion of persistent extraradicular infections.
References
1. Allgayer S, Vanni JR. Intraradicular post and core removal followed by endodontic retreatment: thirteen-year follow-up. RSBO. 2011;8(1):99-104. [ Links ]
2. Byström A, Happonen RP, Sjögren U, Sundqvist G. Healing of periapical lesions of pulpless teeth after endodontic treatment with controlled asepsis. Endod Dent Traumatol. 1987;18:58-63.
3. Danin J, Stromberg T, Forsgren H, Linder L, Ramskold LO. Clinical management of nonhealing periradicular pathosis-surgery versus endodontic retreatment. Oral Surgery Oral Medicine Oral Pathol. 1996;82:213-7.
4. Feix LM, Boijink D, Ferreira R, Wagner MH, Barletta FB. Microscópio operatório na endodontia: magnificação visual e luminosidade. RSBO. 2010;7(3):340-8.
5. Guimarães NLSL, Otoch HM, Andrade LC, Ferreira CM, Rocha MMNP, Gomes FA. Microbiological evaluation of infected root canals and their correlation with pain. RSBO. 2012;9(1):31-7.
6. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposure of dental pulps in germfree and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965;20:340-9.
7. Kim S, Kratchman S. Modern endodontic surgery concepts and practice: a review. J Endod. 2006;32:601-23.
8. Leonardo MR, Rossi MA, Silva LAB, Ito IY, Bonifácio KC. EM evaluation of bacterial biofilm and microorganisms on the apical external root surfasse of human teeth. J Endod. 2002;28(12):815-8.
9. Lin LM, Skribner JE, Gaengler P. Factors associated with endodontic treatment failures. J Endod. 1992;18:625-7.
10. Nair PNR, Sjögren U, Krey G, Kahnberg KE, Sundqvist G. Intraradicular bacteria and fungi in root-filled, asymptomatic human teeth with therapy-resistent periapical lesions: a long-term light and electron microscopic follow-up study. J Endod. 1990;16:580-8.
11. Noiri Y, Ehara A, Kawahara T, Takemura N, Ebisu S. Participation of bacterial biofilms in refractory and chronic periapical periodontitis. J Endod. 2002;28(10):679-83.
12. Signoretti FGC, Endo MS, Gomes BPFA, Montagner F, Tosello FB, Jacinto RC. Persistent extraradicular infection in root-filled asymptomatic human tooth: scanning electron microscopic analysis and microbial investigation after apical microsurgery. J Endod. 2011;37(12):1696-700.
13. Siqueira Jr JF. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod. 2001;34(1):1-10.
14. Sunde PT, Olsen I, Debelian GJ, Tronstad L. Microbiota of periapical lesions refractory to endodontic therapy. J Endod. 2002;28(4):304-10.
15. Taschieri S, Del Fabbro M, TestoriT, Francetti I, Weinstein R. Endodontic surgery using 2 different magnification devices: preliminary results of a randomized controlled study. J Oral Maxillofac Surg. 2006;64:235-42.
16. Tronstad L, Kreshtod D, Barnet t F. Microbiological monitoring and results of treatment of extraradicular endodontic infection. Endod Dent Traumatol. 1990;6:129-36.
17. Vieira AR, Siqueira Jr JF, Ricucci D, Lopes WSP. Dentinal tubule infection as the cause of recurrent disease and late endodontic treatment failure: a case report. J Endod. 2012;38(2):250-4.
18. Von Arx T, Gerber C, Hardt N. Periradicular surgery of molars: a prospective clinical study with a one-year follow-up. Int Endod J. 2001;34:520-5.
 Correspondence:
Correspondence:
Rina Andréa Pelegrine
Rua das Areias, n. 37 – Cambuí
CEP 13024-530 – Campinas – SP – Brasil
E-mail: rinapelegrine@terra.com.br
