










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
ORIGINAL RESEARCH ARTICLE
Clinical effectiveness of light-curing units of the School of Dentistry of the Federal University of Goias
Laís Santos GonçalvesI; Mércia Bráulio GonçalvesI; Marília Morais MartinsI; Gersinei Carlos de FreitasI; Lawrence Gonzaga LopesI; Terezinha Jesus Esteves BarataI
IDepartment of Prevention and Oral Rehabilitation, School of Dentistry, Federal University of Goias – Goiânia – GO – Brazil.
ABSTRACT
Introduction: The clinical longevity of the procedures is directly associated to the adequate activation (photopolymerization) of adhesive restorative materials.
Objective: To evaluate and compare by allocation the conservation status and power density of the light-curing units available at the School of Dentistry of the Federal University of Goias (FO/FUG) for clinical care.
Material and methods: The following information and specific techniques of all light sources existing at FO/UFG, available for clinical care in 2011, were collected: dental/ambulatory clinic where they are located, type of source [device of halogen light and light-emitting diode (LED)], brand, parallelism test (halogen light sources), state of conservation of the light transmitter tip, density of the potency/intensity/irradiance in mW/cm2 and acquisition date. The data obtained were submitted to one-way ANOVA (Analysis of Variance) and Turkey test for multiple comparisons (P < 0.05).
Results: In the second half of 2011, FO/UFG had 20 light sources (04 halogens and 16 LEDs), of which 90% were found in inadequate condition and 55% of those with power density less than 300 mW/cm2. There was no statistically significant difference in the power density between halogen and LED sources tested (P = 0.526). Likewise, no statistical difference was observed between the power density of the light sources (LED) placed at the Clinic II and III (P = 0.479). Also there was no statistically significant difference between the light sources (LED Halogen X) at the Clinic I (P = 0.943).
Conclusion: The light sources regardless of the clinic in which they were located presented mostly with inadequate clinical effectiveness in terms of their conservation status and power density.
Keywords: Endodontics; root canal preparation; gutta-percha.
Introduction
The advancement of aesthetical Dentistry is inter-related to the improvement of both the adhesive restorative materials and the light-curing systems for activation of these materials 3,15,22.
Among the adhesive materials available in dental market, resin composites have been increasingly used in current oral rehabilitation because they attend the function and aesthetical expectations 3,13.
Resin composites are composed by three main components: organic matrix, inorganic filler and bonding agent 14. Bis-GMA (bisphenol A-glycidyl methacrylate) and/or UDMA (urethane dimethacrylate), associated with monomers of low molecular weight as TEGDMA (triethylene glycol dimethacrylate) and EGDMA (ethylene glycol dimethacrylate), comprised the components of the organic matrix 7. The inorganic filler particles within the organic matrix aim to ameliorate the mechanical properties, viscosity and degree of conversion of the resin composites 23. The silane, on the other hand, is the bonding agent most common in the composition of resin composites with the aim of linking the filler particles to the organic matrix. The accelerator/initiator system completes the composition of the resin composites, which can be chemically or physically activated by this system. The chemical activation occurs through a reaction between the benzoyl peroxide and the tertiary amine respectively within the base paste and the catalyst paste 12. On the other hand, the physical activation occurs when the photoinitiators within the resin composites are sensitized by the light sources or light-curing devices 7. Among the photoinitiators, camphorquinone can be emphasized which exhibits a wavelength around 450 to 500 nanometers, with absorption peak at the 460 nm band of light 21.
Among the light sources available in dental market, the light emitting diode devices (LEDs) have been an alternative to the halogen light sources 16. They emit light at specific and narrow wavelength bands, generally at the range between 440 and 500 nanometers, making them an efficient light source for resin composites 15,19,24.
Additionally to the efficiency in photoactivation, LEDs are also a light source of longer clinical durability, lower cost, and lower maintenance than other light sources 8,15,19.
Regardless of the activation system (chemical or physical) of a resin composite, its activation aims to obtain a uniformly and deeply high conversion of the material, associated with low stress of contraction therefore assuring the clinical longevity of the restoration 6. Thus, the success of the restorative procedure using resin materials is directly related to the adequate activation of the restorative procedure [25]. Concerning to the physical activation (photopolymerization) of resin composite, some factors are essential: density of potency/intensity/irradiance, time of exposure, distance from the light transmitter tip to the material to be light-cured, and properties of the resin composites 1,6.
To obtain the adequate characteristics of the resin composites, most of the manufactures recommend the use of an intensity of light/irradiance or minimum power density of 400 mW/cm² 5,11 associated with an exposure time between 20 and 40 seconds 9.
Still regarding to the distance from the transmitter tip to the resin material to be light-cured, it is emphasized that the distance should be as close to the material as possible because the light intensity tend to decrease as the tip is moved away 6.
Consequently, the lack of photoactivation is one of the main factors limiting the clinical success of the restorations with resin composites 3,19,20. This occurs because the lack of photoactivation of the resin composite mostly causes the superficial staining and marginal microleakage 18.
These aspects are related to the improper polymerization of the resin composite and to the increase in the content of the residual monomers 2. Thus, the conservation of the light sources, and consequently, their power density may influence negatively on the mechanical and physical properties of the resin materials. In this context, the aim of this present study is to evaluate the conservation and compare the power density of the light sources available in the School of Dentistry of the Federal University of Goias (FO/UFG) used in the clinical care. The null hypothesis is that the light sources existing in the clinics of FO/UFG had similar conservation and power density.
Material and methods
The following information and technical specifications of all light sources existing in the clinics of FO/UFG and available for clinical care were gathered: the clinic where the device was located, type of source (halogen and LED), brand, parallelism test (halogen light sources), state of conservation of the light transmitter tip, density of the potency/intensity/irradiance in mW/cm2 and acquisition date.
The parallelism test was conducted for the halogen light sources. This test assess the performance of the optical fiber through the contact of the light transmitter tip onto a text printed, when it is possible to visualize it with distinctness the parallelism is considered as positive; if the text is blurred the text is considered as negative 3.
The light intensity or power density of each light source was verified through a radiometer (Curing Radiometer Model 100 p/n – 10503, Demetron Research Corp., USA), according to the protocol proposed by Marson et al. 15 in mW/cm². To measure the power density, the active tip of the light source was placed centrally and perpendicularly to the radiometer and then three readings were performed, so that an arithmetic average was obtained. The first reading was executed for 10 seconds after the light source was switched on, the second and third readings were carried out consecutively with intervals of 30 seconds between each other.
The data obtained were submitted to descriptive statistical analysis, one-way analysis of variance (Anova), and Tukey test for multiple comparisons. The level of significance adopted was 5% (P < 0.05).
Results
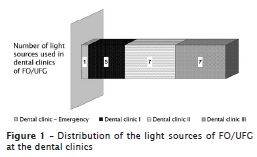
In the second semester of 2011, FO/UFG had 20 light sources, of which 4 were halogens (Dabi Atlante) and 16 were LEDs [DMC (4), Schuster (9) and Sanders (3)]. These light sources were used in the Dentistry graduation and post-graduation courses and were located at 4 dental clinics (figure 1).
The light sources were employed in nine disciplines of graduation: Primary Care Clinic I and II, Children's Clinic I and II, Internship in Integrated Clinical I, II, III and IV and Emergency Clinic. Of these disciplines, the Emergency Clinic is taught in its own clinic, two disciplines are taught in Clinic I (Children's Clinic I and II), two in Clinic II (Primary Care Clinic I and II) and four disciplines in Clinic III (Integrated Clinic I, II, III and IV). This totalized about 100 hours per week of usage of the clinics for the graduation activities. Eventually, the discipline of Surgery and the Extension projects as well as the post-graduation courses utilized the clinics and consequently the light sources when necessary. Concerning to the time of acquisition, it was observed that all light sources of FO/UFG were acquired for more than six months prior to the study, and there had not been any program of periodical preventive maintenance.
In relation to the conservation state, it was observed that 90% of the light sources of FO/UFG showed an inappropriate conservation state, with cracks and/or fractures, as well as residues of resin composite and/or adhesive agent in the light transmitter tip. This study still revealed that 75% of the halogen transmitter light tip exhibited a negative parallelism.
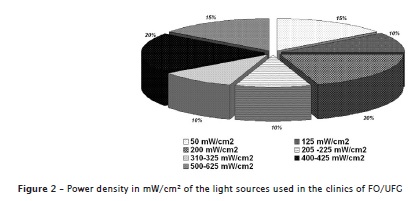
Concerning to the power density, 55% of the light sources showed density lower than 300 mW/cm2 (50-225 mW/cm2) and 35% of the sources exhibited density greater or equal to 400 mW/cm2 (400 – 625 mW/cm2) (figure 2).
The power density values in mW/cm² of the light sources of the clinics of FO/UFG are seen in tables I and II and are divided per type of source and location in the clinic.

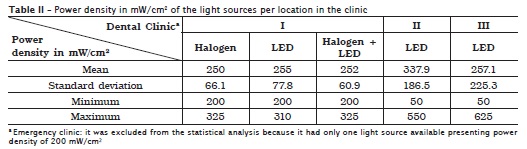
There were no statistical significant differences in the power density among the LED light sources located at the Clinics II and III (P = 0.479). Additionally, there were no statistically significant differences between LED and halogen light sources at Clinic I (P = 0.943). Based on these results, the null hypothesis was accepted.
Discussion
This present study revealed an inadequate conservation state of the light sources available for the clinical care at FO/UFG. Similar situation was observed by Baldi et al. 3 in the School of Dentistry of the State University of Ponta Grossa, in which 69.23% of the light sources were inadequate for use. Likely, in the Dentistry Clinic of the State University of Londrina, Beltrani et al. 4 observed that, regarding to the conservation state of the light transmitter tips, 91.7% exhibit debris, 83.3% were not capable of transmitting light and 16.7% showed any type of fracture.
It is important to emphasize that the performance of the halogen light sources can be decreased by the inadequate maintenance of the optic fiber and light transmitter tip 4,17. It is important to consider that the inadequate conservation of the light sources is related to a smaller intensity of light emission 3-5,15,27. This premise was corroborated by the results obtained by this present study. It can be affirmed that the conservation state of the light sources was directly related to the power density observed. Pascotto et al. 17 still emphasized that the adequate photopolymerization of a resin composite is linked to the light intensity and to the exposure time. It is known that the halogen light devices demand a minimum light intensity of 400 mW/cm² for the adequate photoactivation of the resin composites. On the other hand, LED sources required a minimum light intensity of 300 mW/cm² and at least 20 seconds of exposure time 26.
This present study observed that 65% of the light sources of FO/UFG exhibited power density smaller than 400 mw/cm² (figure 2). Similar condition was found by Borges et al. 5 in the dental clinics of the Federal University of Maranhao. The authors verified that 68% of the light sources tested showed power density smaller than 400 mw/cm².
Likely, studies on the evaluation of the power density in private dental offices have observed these same outcomes, such as those by Freitas et al. 10 in the city of São Luís (MA) and Marson et al. 15 in Maringá (PR). Freitas et al. 10 observed that 46.01% of LED light sources tested exhibited power density smaller than 100 mW/cm²; 44.17% showed power density between 100-400 mW/cm²; and 9.82% presented density greater or equal to 400 mW/cm². For the halogen sources, the authors verified a density between 100 and 400 mW/cm² in 94.73% of the sources tested, while in 5.27% they found an intensity lower than 100 mW/cm²; none light source showed intensity greater than 400 mW/cm². Marson et al. 15 found that 50% of the halogen light sources exhibited power density above 300 mW/cm², 20% between 200-300 mW/cm² and 30% lower than 200 mW/cm².
The literature has described that this clinical situation can result in aesthetic involvement, marginal microleakage, and decrease of the physical and biological properties of the resin composites 7.
Based on this aforementioned discussion, it can be affirmed that the conservation state of the light source directly interfered in the photoactivation effectiveness. Baldi et al. 3, Beltrani et al. 4, Borges et al. 5 and Freitas et al. 10 affirmed that it is necessary the periodical maintenance of the light sources, once their conservation state is related to the power intensity and consequently with the polymerization effectiveness. Therefore, the clinic staff must be aware of these requirements regarding the use of the light sources and the need of a preventive maintenance protocol to achieve the photopolymerization effectiveness.
Conclusion
• The clinical effectiveness of the light sources was dependent on their conservation state and power density, which were inadequate for most of the sources tested;
• The light sources in clinical use exhibited similar conditions of conservation state and power density, regardless the clinic where they were located.
References
1. Accetta DF, Magalhães Filho TR, Weig KM, Fraga RC. Influência dos fotopolimerizadores (luz halógena x LED) na resistência à compressão de resinas compostas. Fac Odontol Rev.2008 Sep-Dec;49(3):17-9. [ Links ]
2. Bagis YH, Rueggeberg FA. The effect of post-cure heating on residual, inreacted monomer in a commercial resin composite. Dent Mater. 2000 16:244-7. [ Links ]
3. Baldi RL, Teideri LD, Leite TM, Martins R, Delgado LAC, Pereira SK. Intensidade de luz de aparelhos fotopolimerizadores utilizados no curso de Odontologia da Universidade Estadual de Ponta Grossa. Publ UEPG Ci Biol Saúde. 2005 Mar;11(1):39-46. [ Links ]
4. Beltrani FC, Caldarelli PG, Kossatz S, Hoeppner MG. Avaliação da intensidade de luz e dos componentes dos aparelhos fotopolimerizadores da Clínica Odontológica da Universidade Estadual de Londrina. Revista Brasileira de Pesquisa em Saúde. 2012 14(1):5-11. [ Links ]
5. Borges FMGS, Rodrigues CC, Freitas SAA, Costa JF, Bauer J. Avaliação da intensidade de luz dos fotopolimerizadores utilizados no curso de Odontologia da Universidade Federal do Maranhão. Rev Ciênc Saúde. 2011 Jan-Jun;13(1):26-30. [ Links ]
6. Davidson CL, De Gee AJ. Light-curing units, polymerization, and clinical implications. J Adhes Dent. 2000;2(3):167-73. [ Links ]
7. Ferracane JL. Resin composite – state of the art. Dent Mater. 2011 Jan;27(1):29-38.
8. Firoozmand LM, Balducci I, Araújo MAM. Influência da fotopolimerização e da cor da resina composta na microdureza. Pesq Bras Odontoped Clín Integr. 2009 Jan-Apr;9(1):37-42. [ Links ]
9. Freitas ABDA, Gomes HR, Guimarães FBR, Marinho VA, Barros LM. Influência do tipo de aparelho fotopolimerizador na absorção de água por restaurações de resina composta. Inst Ciênc Saúde Res. 2008;26(1):65-9. [ Links ]
10. Freitas SAA, Costa JF, Bauer JRO. Avaliação da intensidade da luz dos aparelhos fotopolimerizadores utilizados em clínicas odontológicas de São Luís – MA. Rev Pesq Saúde. 2011 May-Aug;12(2):27-31.
11. Godoy EP, Pereira SK, Carvalho BM, Martins GC, Franco APGO. Aparelhos fotopolimerizadores: elevação de temperatura produzida por meio da dentina e durante a polimerização da resina composta. Rev Clín Pesq Odontol. 2007 Jan-Apr;3(1):11-20. [ Links ]
12. Grando PR, Magnani MBBA, Pereira AC, Meneghim MC, Kurame M, Tavares SW. Colagem de bracket ortodôntico com resina composta e com ionômero de vidro. J Bras Ortodon Ortop Facial. 2002 Mar-Apr;7(38). [ Links ]
13. Loretto SC, Silva AKS, Brandão RKZ, Carneiro MCM, Souza Júnior MHS. Avaliação in vitro da fenda de contração de polimerização formada por diferentes resinas compostas universais. RSBO. 2010 Oct-Dec;7(4):430-8. [ Links ]
14. Lukaszczyk J, Janicki B, Frick A. Investigation on synthesis and properties of isosorbide based bis-GMA analogue. J Mater Sci Mater Med. 2012 May;23(5):1149-55. [ Links ]
15. Marson FC, Mattos R, Sensi LG. Avaliação das condições de uso dos fotopolimerizadores. Rev Dentística. 2010;9(19):15-20. [ Links ]
16. Nomoto R, McCabe JF, Nitta K, Hirano S. Relative efficiency of radiation sources for photopolymerization. Odontology. 2009;97:109-14. [ Links ]
17. Pascotto RC, Pereira SK, Carneiro FP. Avaliação dos aparelhos fotopolimerizadores utilizados em clínicas odontológicas. J Bras Dent Estét. 2003 Jan-Mar;2(5):29-35. [ Links ]
18. Prado Junior RR, Moita Neto JM, Mendes RF, Parente DM. Estudo quimiométrico qualitativo da polimerização de resina composta. RGO. 2008 Jul-Sep;56(3):261-6. [ Links ]
19. Reston EG, Barbosa AN, Busato ALS, Klein Junior CA, Carli G, Carvalho CM et al. Microdureza de resina composta polimerizada com LEDs de diferentes gerações e luz halógena. Stomatos. 2008 Jul-Dec;14(27):17-25. [ Links ]
20. Rodrigues Neto E, Elossais AA, Munõz Cháves OF, Pereira NRS, Silva PG, Saad JRC. Estudo comparativo de aparelhos fotopolimerizadores para determinar o grau de conversão de resinas compostas utilizando o espectrofotômetro de infravermelho. RGO. 2007 Oct-Dec;55(4):357-61. [ Links ]
21. Rueggeberg FA. Contemporary issues in photocuring. Compend Contin Educ Dent Suppl. 1999 Nov;25:4-15. [ Links ]
22. Rueggeberg FA. State-of-the-art: dental photocuring – a review. Dent Mater. 2011 Jan;27(1):39-52.
23. Ruyter IE, Oysaed H. Composites for use in posterior teeth: composition and conversion. J Biomed Mater Res. 1987 Jan;1:11-23. [ Links ]
24. Souza AR, Youssef MN, Turbino ML, Mello B. Avaliação do grau de polimerização de duas resinas compostas utilizando luz halógena e dois diferentes tipos de LEDs. RPG Rev Pós Grad. 2005;12(4):474-80. [ Links ]
25. Strydom C. Dental curing lights – maintenance of visible light curing units. SADJ. 2002 Jun;57(6):227-33.
26. Vieira GF, Freire IA, Agra CM, Goveia JC, Matson E. Análise da irradiação de diversos aparelhos fotopolimerizadores. Rev Odontol Univ São Paulo. 1998 Oct-Dec;12(4). [ Links ]
27. Wunderlich Junior AE. Avaliação de potência de fotopolimerizadores à LED utilizados em consultórios. Ortodontia SP. 2009;42(2):95-100. [ Links ]
 Corresponding author:
Corresponding author:
Terezinha Jesus Esteves Barata
Avenida Universitária, esquina com 1.ª Avenida, s/n, Setor Universitário
CEP 74605-220 – Goiânia – GO – Brasil
E-mail: terezinhabarata@yahoo.com.br
Received for publication: February 14, 2013
Accepted for publication: February 22, 2013
