










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
ORIGINAL RESEARCH ARTICLE
Effect of Gates Glidden, La Axxess, SX and ultrasound on the circularity and area of mesial canals of mandibular molars
Etevaldo Matos Maia FilhoI; Erick Miranda SouzaII; Edimar Oliveira MenesesI; Cláudia de Castro RizziI
IDentistry Course, Ceuma University – São Luís – MA – Brazil.
IIDentistry Course, Florence Institute – São Luís – MA – Brazil.
ABSTRACT
Introduction: Biomechanical preparation must provide a taper shape at crown-apex direction for root canal resulting in adequate space for irrigation and enabling an effective obturation. However, this stage requires a cervical preparation aiming to remove the interferences to make the access to the apical portion easy for instrumentation.
Objective: To evaluate in vitro the effect of coronal flaring on the root canal area and in the circularity of mesial canals of lower molars after using Gates Glidden, La Axxess, Sx file or a ultrasonic TU-24tip.
Material and methods: Twenty-four lower molars had their roots embedded into acrylic resin. Then the roots were sectioned horizontally at 2 mm below the cement-enamel junction. The sections were photographed before and after the different coronal flaring. All images were analyzed using Image J software to calculate the root canal area and the circularity of the root canal. One-way Anova was used to compare the circularity among the groups, while Kruskal-Wallis test was used for comparing the areas. A Pearson test was used to correlate root canal area and circularity data.
Results: There was no significant difference among the groups neither for the circularity (p > 0.05) nor for the root canal area (p > 0.05). There was observed a significant inverse correlation between the root canal area and the circularity (r2 = 0.135; p < 0.05).
Conclusion: Different coronal flaring techniques have produced similar root canal area and circularity, however the larger the canal area the lower the circularity.
Keywords: Endodontic; root canal; instrumentation.
Introduction
Biomechanical preparation is an indispensable phase for endodontic treatment success. It must provide a taper shape at crown-apex direction resulting in adequate space for irrigation and enabling an effective obturation. Additionally, for a better root canal cleaning and shaping, root canal preparation must provide free and direct access the apical portion. Crown-down instrumentation techniques 6 provided the prior flaring of the cervical third for the further access to the apical area. Consequently, an inaccurate preparation of the cervical third will compromise this access mainly in curved roots, as in the mesial roots of mandibular molars and buccal roots of maxillary molars. Cervical flaring 1 aims to make straight the curvatures of the cervical and medium thirds by removing the interferences to make easy the access to the apical area and to decrease the stress during instrumentation 8, consequently diminishing the frequency of fracture of the instruments 10. Additionally, when cervical flaring is not previously executed, an alteration of the working lenght may occur during the instrumentation of the canals 17.
The circularity is defined as the quality or characteristic of which is round and it can vary from values of 1 (perfect circle) to 0 (straight). Mathematically, it is obtained through the circularity formula = 4 π (area/ perimeter2). Cervical flaring should be as circular as possible, decreasing the amount of reentrances, favoring obturation because gutta-percha points exhibit a circular cross-section. Notwithstanding, it is mandatory that this maneuver preserve the risk zone, avoiding perforations at the furcation area; for this purpose, several tools have been used, among them, the use of Gates Glidden and La Axxess burs 17.
Nickel-titanium instruments have been incorporated to the endodontic armamentarium because of their good flexibility, which make them suitable for the preparation of curved canals. ProTaper system for instrumentation (Dentsply/Maillefer, Ballaigues, Switzerland) comprises the SX instrument aiming to the enlargement of the cervical third of the root canal for a posterior apical preparation.
The ultrasound has been used for apical preparations in parendodontic surgery 3, lateral condensation technique 2, placement and removal of the calcium hydroxide inside root canals 9,20. In the endodontic market, ultrasound points are available to execute the cervical flaring of the root canals; however, there have been no studies in the literature on evaluating the capability of ultrasound in cervical flaring. Thus, the aim of this study is to assess the effect of size 3 Gates Glidden bur (Dentsply/Maillefer), size 1 La Axxess bur (SybronEndo, USA), SX (Dentsply/Maillefer) and ultrasound TU-24 tip (Trinity, São Paulo, SP, Brazil) on the amount of dentine removed and on the circularity of the mesial root canals of mandibular first molars.
Material and methods
This present study was approved by the Ethical Committee in Research of the University Center of Maranhao under protocol number #0078/111. Twenty-four mandibular human first molars were selected and their mesial-buccal and mesial-lingual canals were used. The teeth were cleaned with 5% de NaOCl for 24 hours, followed by the carefully removal of the periodontal tissue and calculus. Next, the teeth were washed under running water, dried and stored in 10% formalin solution.
The teeth were embedded into acrylic resin (Artigos Odontológicos Clássico Ltda., São Paulo, SP, Brazil) through using a stainless steel muffle system similar to that described by Kuttler et al. 14. The long axis of the tooth was positioned perpendicularly to the horizontal plane. After the resin polymerization, the teeth were kept at environment temperature for 48 hours.
The coronal access was executed with the aid on number 1016 cylindrical drill (KG Sorensen®, São Paulo, SP, Brazil), under constant irrigation and complemented by Endo-Z drill (Dentsply Maillefer, Ballaigues, Switzerland).
The mesial roots were initially negotiated with a size 10 K file without aiming to the flaring of the root canal.
Two previous radiographs of each mesial root were performed with a size 10 file inside the root canal: at the buccal-lingual and mesial-distal directions. The exposure time and the x-ray processing technique were standardized. The radiographs were analyzed in a dark room with the aid of a negatoscope and x3.5 magnifying glass. Only teeth with moderate curvature roots between 10-35º were used, employing the method of Schneider 18.
With the aid of a precision cutting machine at low speed (Extec® Labcut 1010, Enfield, CT, USA), the blocks were cut perpendicularly to their long axes, 2 mm below the enamel-cementum junction.
The cuts were photographed with a resolution of 7 megapixels by using a digital camera (PowerShot G12, Canon, Japan) linked to an operating microscope (Opto, São Carlos, SP, Brazil) at X20 magnification. The images captured were processed digitally in Adobe Photoshop CS3 software (Adobe System Incorporated, USA), and the root canal area was delimited prior to the procedures. The images were saved in jpeg format.
Each sample was relined in the muffle and the patency was tested with the aid of a size 10 K file to check for the presence of obstructions due to the cutting procedure.
An experienced operator equally trained for the use of the instruments, using only a single instrument of each type, performed all cervical flarings. The techniques were executed at a pre-established sequence so that each technique prepared 12 canals: 6 mesial-lingual and 6 mesial-buccal, totalizing 48 canals.
Gates Glidden, La Axxess and SX instruments were used in a straight handpiece (1:1; Kavo, Joinville, SC, Brazil) together with an endodontic electric motor (Endo Pro Torque/Driller, Jaguaré, SP, Brazil). Size 3 Gates Glidden and size 1 La Axxess were employed at a speed of 6000 rpm, while a speed of 300 rpm was used for SX instruments. The ultrasound TU-24 tip (Trinity, São Paulo, SP, Brazil) was used together with an ultrasound device (Profi Class - Dabi Atlanti, Ribeirão Preto, São Paulo, Brazil), at Endo mode and maximum power for 60 s and water irrigation.
After preparation, the canals were irrigated with 1% sodium hypochlorite with the aid of a syringe and size 31 gauge needle (Ultradent Inc, South Jordan, UTA, USA).
After the preparation, the cuts were removed from the muffle and again photographed similar to previously described. The images, before and after preparation, were transferred to Image J software version 1.46r (http://rsbweb.nih.gov/ij/). To calculate the area and circularity of the root canal, a configuration was carried out in the Analyze/Set Measurements menu by selecting the options Area and Shape descriptors. After delimiting the area regarding to the root canal, the values of area and circularity were obtained by clicking in Analyze/Measure.
The data of the measurements performed on the images before and after the cervical flaring, both for circularity and area, were typed in sheets of Microsoft Excel 2007 for Windows (Microsoft Corporation® USA), and the statistical analyses were executed with SPSS 18.0 software (SPSS Inc, Chicago, IL, USA).
After data tabulation, a descriptive statistical analysis was conducted by emphasizing the means and standard deviations for each treatment type.
To verify whether there were differences among groups in relation to area and circularity, firstly tests were applied to evaluate whether the area and circularity values of the mesial-buccal and mesial-lingual canals would be statistically equal to be included in a single group and whether the distribution was normal and homogeneous. The t test did not exhibit statistically significant difference in either the circularity or area between the mesial-buccal and mesial-lingual canals (p > 0.05). The normality (Shapiro-Wilk test) and homogeneity (Levene test) hypothesis was satisfied for circularity (P > 0.05), but not for the area (p < 0.05). Thus, a parametric test was applied for the circularity (one-way Anova) and a non-parametric test for area (Kruskal-Wallis). Pearson correlation test was applied between the increase of the area and the increase of the circularity. For all tests, the level of significance was set at 0.05.
Results
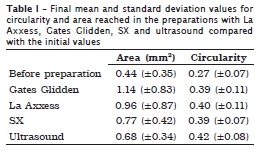
The area and circularity mean values are seen in table I.
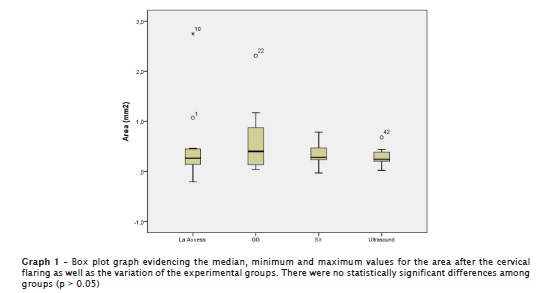
There were no statistical significant differences among treatments for either circularity (p > 0.05) or area (p > 0.05), that is, all preparations showed values statistically similar both for circularity and area.
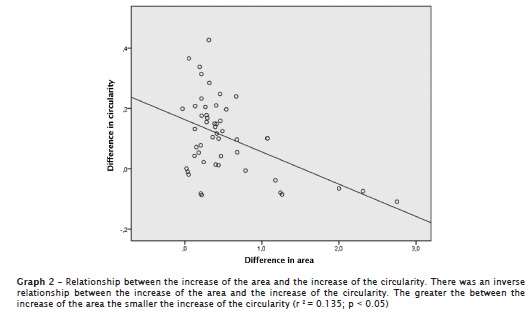
There was a statistically significant negative correlation between the increase of the area and the increase of the circularity for all treatments (r2 = 0.135, p < 0.05). Therefore, the greater the area increase, the smaller the increase of the circularity, indicating that the enlargement of the canal area does not imply in better circularity of the preparation (graph 2).
Discussion
The muffle system 5 employed in this study enables comparing the area worn and the circularity after the cervical flaring and it has been used to evaluate the effect of the root canal instrumentation 12,19,21 and the impact of the preparation of the remnant of dentine post 15. It is a simple method enabling an analysis before and after the cervical flaring and it is of easy reproduction.
According to Bower 4 the furcation area in mandibular molars is found 2 mm below the enamel-cementum junction. Based on this knowledge, the teeth were sectioned at this same measurement. A similar criterion was adopted by Wu et al. 22.
The circularity is an important factor to be considered during the biomechanical preparation and varies between 0 (straight) and 1 (perfect circle). The initial mean value of circularity was of 0.27±0.07, showing little variation before the canals had been prepared. All preparations provided a gain of about 30% in circularity, without however, showing statistically significant difference among groups. Notwithstanding, a negative correlation between the increase of the area and the increase of the circularity was noted (r2 = 0.135, p < 0.05), exhibiting that the increase of the area decreased the circularity. In other words, a better circularity was obtained when there was a smaller weariness of the cervical area. Thus, the greater the area worn the smaller the circularity gain. These data are important, because one could think that the greater the area worn the greater would be the circularity; also, it shows that more conservative wear avoids damages to the furcation area and provides a more circular cervical area. By interpreting the r2 value, one can conclude that the variation in the increasing of the area accounted for 13.3% of the variation of the increase of the circularity, which demonstrates a significant medium effect size of an variable on another. In other words, although there would be other variables accounting for the circularity variation, the area variation was an important factor and it should be taken into consideration during the cervical flaring preparation. Gates Glidden drill provided the greater cervical flaring; however, it was the group together with La Axxess drill, in which the variation showed the greatest mean with standard deviations equal to 0.83 and 0.87, respectively. This large variation in cervical flaring provoked by Gates Glidden drill have already been evidenced in other studies 13,22 and it is not clinically desirable because it can eventually reach the furcation area and cause perforation, as already demonstrated 11,16.
The result of this study showed that La Axxess drill promoted an increase of area similar to that reached by Gates Glidden drill; however, it is known that this latter, differently from La Axxess drill, does not have taper, therefore executing a more uniform wear of the root canal. Thus, caution must be taken in the cervical preparation with these instruments. The preparations with SX files and ultrasound tips were more predictable, because they exhibited little variation. The possible explanation for this smaller wear variation in these groups would be the speed with which SX file was driven (300 rpm), which decreased the cutting action of this instrument; also, it is known that nickel-titanium instruments tend to become more centralized within the root canal than stainless steel instruments 7. On the other hand, a greater control was obtained with the use of the ultrasound tip because it was adjusted to the entrance of the root canal, enabling a controlled wear. SX file presented the smallest mean of cervical dentine removal than Glidden and La Axxess drills; however, without statistically significant differences. Unlikely, Mahran and AboEl-Fotouh 16 concluded that Protaper system removed significantly less dentine from the cervical region than Gates Glidden drills.
Although the ultrasound has been well indicated for the apical preparation in parendodontic surgeries 3, as far as we are concerned, this present study is the first evaluating its use in cervical preparation The ultrasonic diamond tip used in this study is not indicated for the cervical flaring and it was selected because of its similarity to La Axxess drill. Despite of its promising results, further studies are necessary to prove its clinical effectiveness considering other aspects such as the capacity of preserving the furcation region, decreasing the risk of perforation.
Conclusion
Considering the limits of this study, it can be concluded that cervical preparations showed a similar increase of the area and circularity. Notwithstanding, the greater the area increase, the greater the circularity increase.
References
1. Abou-Rass M, Frank AL, Glick DH. The anticurvature filing method to prepare the curved root canal. J Am Dent Assoc. 1980 Nov;101(5):792-4. [ Links ]
2. Bailey GC, Cunnington SA, Ng YL, Gulabivala K, Setchell DJ. Ultrasonic condensation of gutta-percha: the effect of power setting and activation time on temperature rise at the root surface – an in vitro study. Int Endod J. 2004 Jul;37(7):447-54.
3. Bernardes RA, de Moraes IG, Garcia RB, Bernardineli N, Baldi JV, Victorino FR et al. Evaluation of apical cavity preparation with a new type of ultrasonic diamond tip. J Endod. 2007 Apr;33(4):484-7. [ Links ]
4. Bower RC. Furcation morphology relative to periodontal treatment. Furcation entrance architecture. J Periodontol. 1979 Jan;50(1):23-7. [ Links ]
5. Bramante CM, Berbert A, Borges RP. A methodology for evaluation of root canal instrumentation. J Endod. 1987 May;13(5):243-5. [ Links ]
6. Buchanan LS. The standardized-taper root canal preparation, part 1: concepts for variably tapered shaping instruments. Dent Today. 1998 May;17(5):54-60. [ Links ]
7. Carvalho LA, Bonetti I, Borges MA. A comparison of molar root canal preparation using stainless-steel and nickel-titanium instruments. J Endod. 1999 Dec;25(12):807-10. [ Links ]
8. Constante IG, Davidowicz H, Barletta FB, Moura AA. Location and angulation of curvatures of mesiobucal canals of mandibular molars debrided by three endodontic techniques. Braz Oral Res. 2007 Jan-Mar;21(1):22-8. [ Links ]
9. Deveaux E, Dufour D, Boniface B. Five methods of calcium hydroxide intracanal placement: an in vitro evaluation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000 Mar;89(3):349-55. [ Links ]
10. Ehrhardt IC, Zuolo ML, Cunha RS, De Martin AS, Kherlakian D, de Carvalho MC et al. Assessment of the separation incidence of Mtwo files used with preflaring: prospective clinical study. J Endod. 2012 Aug;38(8):1078-81. [ Links ]
11. Gluskin AH, Brown DC, Buchanan LS. A reconstructed computerized tomographic comparison of Ni-Ti rotary GT files versus traditional instruments in canals shaped by novice operators. Int Endod J. 2001 Sep;34(6):476-84. [ Links ]
12. Hulsmann M, Schade M, Schafers F. A comparative study of root canal preparation with Hero 642 and Quantec SC rotary Ni-Ti instruments. Int Endod J. 2001 Oct;34(7):538-46. [ Links ]
13. Isom TL, Marshall JG, Baumgartner JC. Evaluation of root thickness in curved canals after flaring. J Endod. 1995 Jul;21(7):368-71. [ Links ]
14. Kuttler S, Garala M, Perez R, Dorn SO. The endodontic cube: a system designed for evaluation of root canal anatomy and canal preparation. J Endod. 2001 Aug;27(8):533-6. [ Links ]
15. Kuttler S, McLean A, Dorn S, Fischzang A. The impact of post space preparation with Gates-Glidden drills on residual dentin thickness in distal roots of mandibular molars. J Am Dent Assoc. 2004 Jul;135(7):903-9. [ Links ]
16. Mahran AH, AboEl-Fotouh MM. Comparison of effects of ProTaper, HeroShaper, and Gates Glidden Burs on cervical dentin thickness and root canal volume by using multislice computed tomography. J Endod. 2008 Oct;34(10):1219-22. [ Links ]
17. Schmitz Mda S, Santos R, Capelli A, Jacobovitz M, Spano JC, Pecora JD. Influence of cervical preflaring on determination of apical file size in mandibular molars: SEM analysis. Braz Dent J. 2008;19(3):245-51. [ Links ]
18. Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol. 1971 Aug;32(2):271-5. [ Links ]
19. Souza EM, do Nascimento LM, Maia Filho EM, Alves CM. The impact of post preparation on the residual dentin thickness of maxillary molars. J Prosthet Dent. 2011 Sep;106(3):184-90. [ Links ]
20. van der Sluis LW, Wu MK, Wesselink PR. The evaluation of removal of calcium hydroxide paste from an artificial standardized groove in the apical root canal using different irrigation methodologies. Int Endod J. 2007 Jan;40(1):52-7. [ Links ]
21. Wu MK, van der Sluis LW, Wesselink PR. The capability of two hand instrumentation techniques to remove the inner layer of dentine in oval canals. Int Endod J. 2003 Mar;36(3):218-24. [ Links ]
22. Wu MK, van der Sluis LW, Wesselink PR. The risk of furcal perforation in mandibular molars using Gates-Glidden drills with anticurvature pressure. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005 Mar;99(3):378-82. [ Links ]
 Corresponding author:
Corresponding author:
Etevaldo Matos Maia Filho
Rua Duque Bacelar, Q. 1, Casa 11 – Altos do Calhau
CEP 65071-785 – São Luís – MA – Brasil
E-mail: rizzimaia@yahoo.com.br
Received for publication: August 7, 2013
Accepted for publication: March 14, 2013
