










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
ORIGINAL RESEARCH ARTICLE
Influence of different surface treatments on the shear bond strength of a methacrylate resin composite repaired with silorane-based resin
Leonardo Fernandes da CunhaI; Dilcele Silva Moreira DziedzicI; Bruno Moreno NascimentoI; Samantha Shaffer Pugsley BarattoII; Carla Castiglia GonzagaII; Adilson Yoshio FuruseII; José MondelliI; Odirlei Arruda MalaspinaIII
IDepartment of Operative Dentistry, Endodontics and Dental Materials, Bauru School of Dentistry – Bauru – SP – Brazil.
IIMaster of Science Program in Clinical Dentistry, Positivo University – Curitiba – PR – Brazil.
IIISuperior School of Health Sciences, Amazonas State University – Manaus – AM – Brazil.
ABSTRACT
Introduction: When repairs are needed in restorations made with methacrylate-based resin composites, the clinician still has doubts whether it is possible to use a silorane-based material and which is the best procedure.
Objective: To evaluate the shear bond strength between a methacrylate-based resin composite and a silorane-based material using different surface treatments.
Material and methods: Eighty flat bases made with methacrylate resin composite (Filtek Z350 XT) were prepared (n = 8). The bases were stored into water at 37°C for one week. Ten groups were evaluated: G1 (control – no repair); G2 (surface grinding, washing, drying, adhesive and repair with Filtek Z350 XT); G3 (surface grinding, washing, drying, adhesive and repair with silorane – Filtek P90); G4 (surface grinding, washing, drying, adhesive, silane and repair with Filtek Z350 XT); G5 (surface grinding, washing, drying, application of silane, adhesive and repair with silorane – Filtek P90). All groups were kept at 37°C for 24 h in either water (G1 to G5) or ethanol (G6 to G10). The results were analyzed with one-way ANOVA and Tukey test (α = 0.05).
Results: There were significant differences between groups (p < 0.001). Only repairs made with silane and Z350 XT (G4 = 46.2 ± 12.9; G9 = 48.1 ± 16.3) resulted in values similar to controls (G1 = 59.2 ± 15.8; G6 = 62.3 ± 15.9) (p = 0.33). The smallest value occured when the repair was performed with silane and silorane-based based and stored into ethanol (G10 = 29.9 ± 12.4). The storage media had little influence on the results.
Conclusion: The silorane-based resin composite was not effective for repair of the methacrylate-based material.
Keywords: composite resins; shear strength; adhesives.
Introduction
The long-term durability of resin composite restorations is a constant worry 9,20. Invariably, the replacement of a restoration results in greater weariness of the tooth structure 13. For this reason, the restoration repair is a more conservative, faster, and a lower cost procedure both for the professional and the patient.
The study of the physical-chemical and mechanical properties of the adhesive systems should not only be studied between tooth structure and restorative material, but also between two dental materials. If the adhesive bonding between an old and new resin is effective, the restoration repair becomes a treatment option to be recommended 21.
In studies evaluating the bond strength of repairs of resin composites, the surface grinding followed by the application of silane bonding agents have demonstrated good results 10.
otwithstanding, this studies have been conducted on resins with the same organic matrix.
In the last decade, a resin with a new silorane-based monomer has been described, which is the result of a reaction between oxirane and siloxane molecules 22. In this new system, the opening of the oxirane ring during the polymerization reaction compensates the stresses generated during the polymerization contraction. Studies have reported on this new technology. Eick et al. 8 described the hydrophobicity of the material, resulting in stability under oral fluids. A smaller amount of Streptoccocus has also been found on this new resin 5, therefore favoring the longevity of the material. Additionally, a good color stability 6,11, bonding values similar for enamel and dentine has been reported 12. Therefore, this material seems to be promising for restoration of posterior teeth. However, data on the bonding of this material on methacrylate-based resins still lack in the literature. Thus, during the repair of silorane-based repair, it is not clarified which would be the effectiveness and best surface treatment to provide an adequate bonding between the old restoration and new silorane-based resin repair.
Moreover, the behavior of the interaction among the layers should be evaluated at long term. This aging can be simulated laboratorially through storage of the specimens into aqueous solutions. Normally, the immersion into water at 37ºC is the medium of choice. However, the ethanol solutions well known as aging solutions for BisGMA-based materials can accelerate the material degradation because they can diffuse through the resin provoking its softening 3. Thus, the aim of this study was to evaluate the shear bond strength of methacrylate- and silorane-based resin composites through using different surface treatments and storage media.
Material and methods
Eighty flat bases made with acrylic resin were prepared containing a cylindrical orifice of 6 mm of diameter and 2 mm of deepness. These orifices were filled with a methacrylate-based resin (Filtek Z350 XT, 3M ESPE, St. Paul, USA). Of the 80 resin composite bases, 64 were immersed into distilled water at 37ºC for one week.
The resin composite insertion was executed with a resin spatula at two increments. Each layer was light-cured through a device (Elipar Trilight – Espe - 500mv/cm2) for the period recommended by the manufacturer. This same device was employed during all study phases and the irradiance was checked with a radiometer linked to the light-curing device prior to each use. To adapt the last resin composite increment, a polyester strip (TDV Dental Ltda., Pomerode, Brazil), was placed aiming to leave the surface as flat as possible. The 80 surfaces of resin composite were divided into 10 groups (n = 8). The experimental treatments were executed on the resin composite surface. The groups were divided as follows:
• G1 – Control group: immediately after the construction of a flat resin composite base onto the acrylic resin matrix, only one cylinder of Filtek Z350 XT (3.5 mm of diameter per 2 mm of height) was executed onto the resin composite surface with the aid of Teflon matrix. Following, the specimens were stored into distilled water at 37°C for one week. After the construction, the specimens were immersed into distilled water at 37oC for 24 h, prior to the shear bond strength test;
• G2: the resin composite surface was grinded with the aid of a medium grit sandpaper (Sof Lex Pop-on, 3M Espe, St. Paul, USA), washed with water jet for 15 s and dried with air jet for 20 s at 10 cm of distance. Next, the adhesive agent (Adper Single Bond 2, 3M Espe, St. Paul, USA) was applied according to the manufacturer's instructions. With the aid of a Teflon matrix, a cylinder of Filtek Z350 XT resin composite was constructed (3.5 mm of diameter per 2 mm of height). After the construction, the specimens were immersed into distilled water at 37oC for 24 h;
• G3: same treatment of G2, however, Filtek P90 adhesive system (3M Espe, St. Paul, USA) and Filtek P90 silorane-based resin composite (3M Espe, St. Paul, USA) were used. After the construction, the specimens were immersed into distilled water at 37oC for 24 h;
• G4: the surface was grinded with medium grit sandpaper, washed with water jet for 15 s and dried with air jets for 20 s at 10 cm of distance. Following, a silane (Silano, Ângelus, Londrina, Brazil) and Single Bond 2 adhesive agent were applied and a cylinder of Filtek Z350 XT resin composite was constructed. After the construction, the specimens were immersed into distilled water at 37oC for 24 h;
• G5: same treatment of G4, however the Filtek P90 adhesive system and Filtek P90 silorane-based resin composite was used. Then, the specimens were immersed into distilled water at 37oC for 24 h;
• G6, G7, G8, G9 e G10: same treatments of G1, G2, G3, G4 and G5, respectively; however, after the construction of the resin composite cylinders, the specimens were kept into ethanol (75% in volume) at 37oC for 24 hours, to mimic the resin composite aging. After the storage period in either water or ethanol, the specimens were submitted to shear bond strength test in a universal testing machine (EMIC, São José dos Pinhais – PR, Brazil), with crosshead speed of 1.0 mm/min.
Data were analyzed through one-way ANOVA. The possible statistical differences among groups were determined by Tukey test. A global level of significance of 5% was adopted.
Results
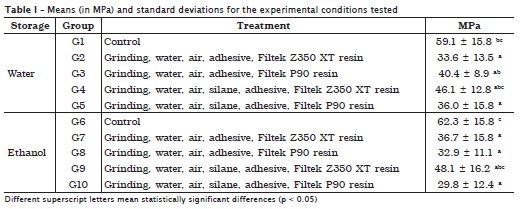
The means (in MPa) and standard deviations of the results obtained are seen in table I. There were statistically significant differences among the treatments proposed (p < 0.001). Only the repairs executed with silane and Z350 XT (G4 = 46.2 ± 12.9; G9 = 48.1 ± 16.3) were capable of generating values similar to those of controls (G1 = 59.2 ± 15.8; G6 = 62.3 ± 15.9) (p = 0.33). None repair performed with silorane-based resin generated shear bond strength values similar to those of control group. The smallest value was obtained when the repair was carried out with the silorane-based resin after the application of a silane and storage in ethanol (G10 = 29.9 ± 12.4). Generally, the storage media had a little influence on the results.
Discussion
Silorane-based resins have been recently launched worldwide. Magni et al. 16 evaluated the repair with silorane-based resin onto another silorane-based resin. Accordingly, Ivanovas et al. 14, Lurhs et al. 15 and Maneenut et al. 17 studied the silorane-based repair and verified that it is possible to execute a methacrylate-based resin repair onto a silorane-based resin. However, information on silorane-based resin repair onto methacrylate-based resin is still scarce. The idea of repairing a methacrylate-based resin with a silorane-based resin is justified because not always the professional knows the resin type that was employed to construct a prior restoration. This aspect was recently studied by Popoff et al. 18. In a clinical study with one year of following-up, these authors observed that the silorane-based resin used to repair a methacrylate-based resin behaved similarly to control group, in which the repair was executed with a methacrylate-based resin. In this present study, however, none repair performed with silorane-based resin generated bond strength values similar to those of control group. Maybe the evaluation time of one year employed in the study of Popoff et al. 18 had not been enough to detect a possible clinical difference.
Different methods can measure the bond strength to determine either the effectiveness or the ineffectiveness of the adhesion between different materials, such as microtensile, microshear or shear bond strength. In this present study, the shear bond strength method was used to measure the adhesive forces between aged methacrylate-based resin simulating a restoration and a new methacrylate- or silorane-based resin. This type of test has the advantage to mimic the clinical condition very closely because it results in stress on the interface between the materials 1.
The most commonly and traditionally technique for in vitro aging of specimens is the storage in water for longer times 7. This decrease in the adhesive effectiveness is caused by the hydrolysis degradation of the organic components present in the adhesive interface. Notwithstanding, another simulated aging method is storage in ethanol, as used by Asmussen 1 and Furuse et al. 10. The different methods of aging are employed attempting to estimate which would be a possible clinical behavior at long term. In this present study, there were no differences between water and ethanol storage. It is important to highlight that the specimens were aged in ethanol for only 24 h and that longer times could have influence on the results.
The different treatments influence on the bond strength of the different groups. The chemical treatment of the resin composite prior to the construction of the repairs by applying silanizing agents is controversy according to the studies conducted by Soderholm et al. 19, Brosh et al. 4 and Furuse et al. 10. In this present study, the shear bond strength values of the silanized groups with silorane-based repairs were smaller; however, there were no statistical significant differences in relation to the groups in which the silane agent was not applied. It is important to emphasize that only one type of methacrylate-based resin was used in this present study and that not all materials are similar. Thus, the data here presented should be cautiously interpreted. Further studies evaluating different methacrylate-based resins as well as different types and methods of silane application should be conducted.
Conclusion
Taking into consideration the limitations of this present study, it can be concluded that the repair of methacrylate-based resin with silorane-based resin demonstrated the smallest shear bond strength values.
References
1. Anusavice KJ. Phillips materiais dentários. 10. ed. Rio de Janeiro: Guanabara Koogan; 1998. [ Links ]
2. Asmussen E. Softening of BISGMA-based polymers by ethanol and by organic acids of plaque. Scand J Dent Res. 1984 Jun;92(3):257-61. [ Links ]
3. Benetti AR, Asmussen E, Munksgaard EC, Dewaele M, Peutzfeldt A, Leloup G et al. Softening and elution of monomers in ethanol. Dent Mater. 2009 Aug;25(8):1007-13. [ Links ]
4. Brosh T, Pilo R, Bichacho N, Blutstein R. Effect of combinations of surface treatments and bonding agents on the bond strength of repaired composites. J Prosthet Dent. 1997 Feb;77(2):122-6. [ Links ]
5. Buergers R, Schneider-Brachert W, Hahnel S, Rosentritt M, Handel G. Streptococcal adhesion to novel low-shrink silorane-based restorative. Dent Mater. 2009 Feb;25(2):269-75. [ Links ]
6. Cunha LF, Santana L, Baratto SSP, Mondelli J, Haragushiku GA, Gonzaga CC et al. Staining susceptibility of methacrilate and silorane-based materials: influence of resin type and storage time. RSBO. 2013 Apr-Jun;10(2):161-6. [ Links ]
7. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M et al. A critical review of the durability of adhesion to tooth tissue: methods and results. J Dent Res. 2005 Feb;84(2):118-32. [ Links ]
8. Eick JD, Smith RE, Pinzino CS, Kostoryz EL. Stability of silorane dental monomers in aqueous systems. J Dent. 2006 Jul;34(6):405-10. [ Links ]
9. Ergucu Z, Turkun LS. Clinical performance of novel resin composites in posterior teeth: 18-month results. J Adhes Dent. 2007 Apr;9(2):209-16. [ Links ]
10. Furuse AY, Cunha LF, Benetti AR, Mondelli J. Bond strength of resin-resin interfaces contaminated with saliva and submitted to different surface treatments. J Appl Oral Sci. 2007 Dec;15(6):501-5. [ Links ]
11. Furuse AY, Gordon K, Rodrigues FP, Silikas N, Watts DC. Colour-stability and gloss-retention of silorane and dimethacrylate composites with accelerated aging. J Dent. 2008 Nov;36(11):945-52. [ Links ]
12. Garcia RN, Alvarez AEG, Dias CE, Mazaro MA, Firmo T, Stuker H et al. Bond strength of contemporary restorative systems to enamel and dentin. RSBO. 2011;8(1):54-60. [ Links ]
13. Gordan VV. Clinical evaluation of replacement of class V resin based composite restorations. J Dent. 2001 Sep;29(7):485-8. [ Links ]
14. Ivanovas S, Hickel R, Ilie N. How to repair fillings made by silorane-based composites. Clin Oral Investig. 2011 Dec;15(6):915-22. [ Links ]
15. Luhrs AK, Gormann B, Jacker-Guhr S, Geurtsen W. Repairability of dental siloranes in vitro. Dent Mater. 2011 Feb;27(2):144-9. [ Links ]
16. Magni E, Ferrari M, Papacchini F, Hickel R, Ilie N. Influence of ozone application on the repair strength of silorane-based and ormocer-based composites. Am J Dent. 2010 Oct;23(5):260-4. [ Links ]
17. Maneenut C, Sakoolnamarka R, Tyas MJ. The repair potential of resin composite materials. Dent Mater. 2011 Feb;27(2):e20-7. [ Links ]
18. Popoff D, Rosa TS, Ferreira R, Magalhaes C, Moreira A, Mjor I. Repair of dimethacrylate-based composite restorations by a silorane-based composite: a one-year randomized clinical trial. Oper Dent. 2012 Sep-Oct;37(5):E1-E10. [ Links ]
19. Soderholm KJ, Zigan M, Ragan M, Fischlschweiger W, Bergman M. Hydrolytic degradation of dental composites. J Dent Res. 1984 Oct;63(10):1248-54. [ Links ]
20. Turkun LS, Turkun M, Ozata F. Clinical performance of a packable resin composite for a period of 3 years. Quintessence Int. 2005 May;36(5):365-72. [ Links ]
21. Vankerckhoven H, Lambrechts P, van Beylen M, Davidson CL, Vanherle G. Unreacted methacrylate groups on the surfaces of composite resins. J Dent Res. 1982 Jun;61(6):791-5. [ Links ]
22. Weinmann W, Thalacker C, Guggenberger R. Siloranes in dental composites. Dent Mater. 2005 Jan;21(1):68-74. [ Links ]
 Corresponding author:
Corresponding author:
Leonardo Fernandes da Cunha
Centro Odontológico Brasiliense – Brasília Shopping/SCN
Quadra 5, Bloco A
CEP 70710-500 – Brasília, DF – Brasil
E-mail: cunha_leo@yahoo.com.br
Received for publication: September 12, 2012
Accepted for publication: December 20, 2012
