










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
ORIGINAL RESEARCH ARTICLE
DMFT index of 12 year-old students of public schools participating in the Project of Education for Working for Health
Denise VizzottoI; Helena Maria Antunes PaianoI; Ana Caroline RudeyI; Andréia Karina LoveraI; Pricylla HagemannI; Tatiane GazollaI
IDepartment of Dentistry, University of Joinville Region – Joinville – SC – Brazil.
ABSTRACT
Introduction: Epidemiological surveys provide a key basis for assessing current and future oral health care needs of a population by yielding reliable data for designing national or regional health programs 12.
Objective: To assess the oral health status of 12-year-old adolescents by applying DMFT index in the city of Joinville, SC, who took part in the PEW Health Project 2010-2011 and designing a comparative study between 2003 and 2010 national, state, municipal and other DMFT surveys for this same age range.
Material and methods: Analytical cross-sectional observational study. Dental health assessment tool used was DMFT and deft index. The codes and criteria used for the survey used the tooth as a study unit according to methodology proposed by WHO and reported in the SB-Brazil Assessor's Manual 3. Sample size was 194 students attending public junior high school. Chi-square test for qualitative variables and Student's t test for quantitative variables were used, with two-tailed significance level of 5%.
Results: DMFT was 0.84, standard deviation 1.31 and confidence interval 0.65 (lowest) and 1.02 (highest). Rate of cavity-free children or zero DMFT was 58.8%, a total of 114 children.
Conclusion: The students of the city of Joinville, SC assessed by this study showed low cavity prevalence, thereby reaching WHO approved targets for 2010.
Keywords: DMFT index; dental caries; epidemiological surveys; oral health.
Introduction
The knowledge of the health or disease condition of a population is fundamental for establishing a health working planing. In Brazil, the Law #8,080 of September 19 of 1990, known as Organic Health Law claims (Article 7th, VII) "the use of epidemiology for the establishment of priorities, allocation of resources and programmatic guidance" 14,19.
The epidemiological surveys provide an important basis for the estimative of both the current situation and the further necessity of health care of a population, resulting in reliable data for the development of either national or regional health programs. The main index for epidemiological surveys in oral health has been DMFT (decayed, missed, and filled teeth) 12.
The World Health Organization (WHO) uses the mean DMFT index at 12 years-old as the basic index of comparison for oral health of different populations. This index is of easy collection in primary schools, so that DMFT for this age group has been the best epidemiological index to describe the oral health status of the childhood and adolescence 14.
The caries attack rate, was originally created by Klein and Palmer in 1937, known by the acronym DMF and it is still the most used index worldwide, being kept as the basic landmark for the diagnosis of dental conditions, preparation and assessment of Oral Health Programs. The caries attack rate (DMFT) has been applied to permanent teeth. For primary teeth, the index is identified by lowercase letters, so-called deft index, which uses criteria similar to those of DMFT 12,17. The sampling method, used in DMFT, it is a stratified technique, aiming to include the most important population subgroups regarding to the different levels of the disease and comprise a standardized number of individuals of determined age groups at each site 12.
According to WHO 23, there are five severity stages for DMFT at 12 years-old: very low (from 0 to 1.1), low (from 1.2 to 2.6), moderate (from 2.7 to 4.4), severe (from 4.5 to 6.5), very severe (6.6 or higher).
In the first Brazilian epidemiological study, conducted in 1986 by the Ministry of Health, at 12 years-old, it was detected that tooth caries reached a DMFT index of 6.7, with prevalence higher than 90% 1.
WHO advocated for the 2000s a mean DMFT of 3.0 at 12 years-old, that is, at most three teeth injured by the disease; for the 2010s a mean DMFT of at most one tooth injured by the disease 8. The survey conducted in 2010 by the Brazilian Ministry of Health (SB Brazil 2010) 4, comprised 177 Brazilian cities, 26 state capitals, and the Federal District as well as 30 cities randomly selected for each one of the five regions of the country. In 2003, at 12 years-old, the disease reached 69% of the population, decreasing to 56% in 2010. This decrease of 13 percentage points corresponds to a decrease of 19% in the disease prevalence. The mean number of teeth damaged by the disease also decreased at 12 years-old: from a DMFT index of 2.8 in 2003 to 2.1 in 2010, a reduction of 25%. The proportion of caries-free children at 12 years-old increased from 31% to 44% 4. The city of Joinville (SC) was enrolled in the sample of the 2003 survey and the DMFT index found at 12 years-old was 1.19 20.
The purpose of this study was two-fold: to assess the diagnosis of the oral health condition of adolescents at 12 years-old, through DMFT index, attending public junior high schools of the city of Joinville (SC) participating in the Project of Education for Working for Health 2010/2011 (PEW-Health); and to elaborate a comparative study among the Brazilian national, state, and municipal DMFT index of 2003 and 2010 as well as other studies at this age range.
Material and methods
Analytical cross-sectional observational study. Dental health assessment tool used was DMFT and deft index. The codes and criteria used for the survey used the tooth as a study unit according to methodology proposed by WHO and reported in the SB-Brazil Assessor's Manual 3.
The survey was conducted in the following four public junior high school: "Rosa Maria Berezoski Demarchi" (Paraíso district), "Pauline Parucker" (Boehmerwaldt district), "Hilda Ana Krischs" (Iririú district) and "Lacy Luíza Flores" (Itinga district), located in the suburbs of the city of Joinville (SC). The choice for the districts and schools was determined by the social-economic status presented by the students and the location in the areas enrolledin the Family Health Teams of the PEW-Health of 2010/2011, respectively. The mean income of the parents/legal guardians per home and district was R$ 400.00; R$ 500.00; R$ 600.00 and R$ 480.00, respectively 7.
The sample was composed by 194 students of 12 years-old, 11 months and 29 days up to the moment of the data collection, regardless of the gender, race and social class. The sampling was randomly obtained. Exclusion criteria comprised students aging above the age range; using orthodontic appliance at the moment of the examination and/or whose parents/legal guardians did not sign the consent form. Prior to the examinations, oral hygiene through toothbrushing and toothpaste was executed in all students selected for the research. The examinations were carried out only after the signing of a clarified consent form by the parents and/or legal guardians (Ethical Committee in Research protocol number #115/2011). The data collection followed the methodology proposed by the Brazilian Health Ministry: outdoors in a bright environment through using disposable tongue depressors; plane dental mirror and WHO dental probe.
The collection instrument used was a structured questionnaire, available at the Brazilian Ministry website 3, and adapted following the requirements of this study. Only the blanks corresponding to the general information (number identity of the student, age in years, gender, race, date of examination) and the blanks regarding to Dental Caries and Treatment Needs were filled in using the codes proposed by the Brazilian Ministry of Health.
Four examiners, four annotators and two assistants participated in data collection (undergraduate students of the School of Dentistry of the Joinville Region - Univille). Inter- and intra-examiner agreement calibration was performed according to the methodology proposed 3, obtaining a general minimum percentage of agreement of 0.988% and minimum weighted kappa of 0.778.
Data were stored in MsExcel 2003 software. Descriptive tables were constructed and the statistical tests applied were Chi-square to compare the qualitative variables and Student's t test for quantitative variables with two-tailed level of significance of 5%.
Results
The number of students in the four public students during the period of the study and in the age range was 611. Two-hundred and seventy-one students were randomly drawn to compose the sample. However, 194 students at 12 years-old were, in fact, examined. Of these, 100 (51.5%) were male and 94 (48.45%) female. Concerning to race, 108 students identified themselves as Caucasian, (representing more than 50% of the sample), Brown (35.05%), Black (6.19%), Yellow (2.06%) and Indian (1.03%).
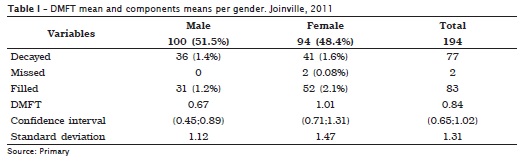
The DMFT mean found was of 0.84 (SD = 1.31), confidence interval of 0.65 (minimum) and 1.02 (maximum). The percentage of caries-free children (DMFT = 0) was of 58.8%, corresponding to 114 children. The caries prevalence was of 23%, without statistically significant differences between genders (male = 23%; female = 22.3%) (p = 0.91 – Chi-square test of independence). There were no statistically significant differences between genders for general sample DMFT (p = 0.07 for male and p = 0.88 for females – Student's t test).
Concerning to the DMFT composition – decayed, missed, and filled – all components showed similar proportions between genders (table I). Statistically, there were no differences of mean DMFT values between genders.
For children with traumatized teeth, the percentage was of 10.3%, which corresponded to 20 children with a total of 42 (0.8%) traumatized teeth, while 29.4% of the population studied required the treatment of one or more teeth.
Discussion
Between the 1960s and 70s, the tooth caries rates exhibited high values at 12 years-old in developed and some developing countries. In the last years, the disease decrease at this age has been observed in Brazil and worldwide 18.
This present study corroborates these affirmations, because the DMFT found in the population researched was of 0.84, which is considered of very low prevalence, according to the measurement scale of caries attack severity at 12 years-old advocated by WHO 23.
Traebert et al. 21 studied a student population from the city of Blumenau (SC/Brazil). A sample of 1,473 students participated in the survey, representing four strata: 6-12 year-old students from public and private schools. The caries prevalence in the permanent dentition at 12 years-old was of 54.7%, and DMTF index was of 1.46 for public schools. In the public schools, at this same age, it could be seen that 53.0% of children did not exhibit treatment requirements. Cypriano et al. 6 examined 3,731 children from 5 to 12 years-old and found tooth caries data in seven cities of the region of Sorocaba (São Paulo/Brazil) which had or did not have fluoridation of the public water supply. At 12 years-old, 32.3% of the students were caries free and the DMFT was of 2.6. The children living in fluoridated areas had the smallest caries experience in primary dentition; also, these areas showed a higher percentage of caries free children, denoting the best conditions of oral health in these cities. Such data are different from those of this present study.
Freire et al. 9 conducted a study aiming to compare 12-year-old students from private and public study regarding to the caries prevalence, periodontal status, dentofacial anomalies, and fluorosis. This was a cross-sectional study with 1,947 12-year-old students enrolled in urban area of the city of Goiânia (Goiás/Brazil), divided into 1,790 children from public and 157 from private schools, in 2003. Most of the students examined were female (51.6%), and the caries prevalence was of 64% and the mean DMFT was of 2.29. The components decayed, missed, and filled comprised 49.6%, 2.1% and 48.2% of the index, respectively. The students from public schools showed the highest prevalence of the disease and highest values of both DMFT and its components than those of the private schools.
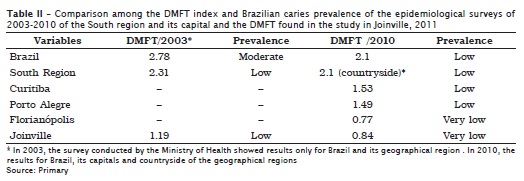
The SB Brazil 2003 epidemiological survey, conducted by the Brazilian Health Ministry 2, found a Brazilian DMFT of 2.78 at 12 years-old, value similar to that of the Brazilian South region (2.31); that of the study of Freire et al. 9 for the city of Goiânia, (Goiás/Brazil), in 2003; and that of the study of Cypriano et al. 6 for seven cities of the area of Sorocaba (São Paulo/Brazil), whose mean DMFT values were 2.29 and 2.6, respectively. However, this value was far above the mean of 1.19 found for the city of Joinville in 2003 20 and of 1.46 reported in the study of Traebert et al. 21 in public schools of the city of Blumenau (SC).
In the SB Brazil 2010 epidemiological survey 4, DMFT at 12 years-old was of 2.1, value similar to that found in the countryside of the Brazilian South region (2.17). The same data for the capitals of Curitiba and Porto Alegre was of 1.53 e 1.49, respectively. Notwithstanding, the same study found a mean of 0.77 for the city of Florianópolis, which was similar to that found in the city of Joinville (2011) by this present study.
The DMFT means found in SB Brazil 2010 4 for the Brazilian South (2.06) and Southeast regions (1.72) were similar between each other, although higher than that of this present study (0.84). For the Brazilian North (3.16), Northeast and Midwest regions (2.63), the DMFT mean was very higher than those of the other regions and that of this present study.
The data of table II demonstrated a reduction of the DMFT index from 2.78 to 2.1, which corresponds to 26%, when compared to those of the Brazilian epidemiological surveys of 2003 and 2010 4. This reduction could also be observed for the city of Joinville, whose DMFT mean changed from 1.19 in 2003 to 0.84 in 2011, resulting in a reduction of 30%.
Still regarding the caries-free children (DMFT = 0), this study found a value of 58.8%, which was similar to that found in the city of Florianópolis (68.4%), reported in the SB Brazil 2010 epidemiological survey 4, and higher than that found in the capital of the South Region: Porto Alegre (48.8%) and Curitiba (44.7%), and that found in the countryside of the South Region (39.7%). There were no statistically differences between the results of Joinville in 2011 and of Florianópolis in 2010 (p = 0.76 –Student's t test). However, there were statistically significant differences in relation of the other results (p < 0.005 – Student's t test).
Concerning to the DMFT components, this study found 22.7% for "D" (decayed), which was very below the results reported by SB Brazil 4 for all country (54.1%), countryside of the South Region (55.3%) and for Florianópolis (59.7%), as seen in table III.
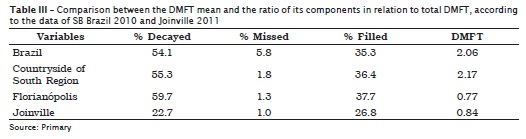
For the M component (missed), the study found a value of 1.0%, which was lower than those reported in the SB Brazil 2010 epidemiological survey 4 for Brazil (5.8%), countryside of the South Region (1.8%) and Florianópolis (1.3%).
Concerning to F component (filled), the present study found a value of 26.8%, which was different from those of the SB Brazil 2010 epidemiological survey for Brazil (35.3%), countryside of the South Region (36.4%) and Florianópolis (37.4%) 4. It could be inferred that the result found in the study of Joinville is in agreement with the percentage of decayed teeth, which was lower than those of the other areas, as previously cited. Still, the study identified that 70.6% of the adolescents did not required any treatment.
The prevalence of caries in the city of Joinville, considering the sample studied, exhibits a decrease similar to that found by the Brazilian Ministry of Health at 12 years-old. The mean DMFT value decreased from 1.19 to 0.84, exhibiting a reduction of 30%, while this same index showed a reduction of 26% for all the country. The result confirms the decrease in the caries prevalence at this age range, similarly to which has been happening in the Brazilian South and Southeast Regions, and demonstrated by the epidemiological surveys conducted by the Brazilian Ministry of Health in 2003 and 2010 2,4.
Pinto 16, Marcenes and Bonecker 10, Traebert et al. 21 observed that the oral health condition improved in the last decades in Brazil.The authors cited as possible causes for this decrease: the addition of fluoride to public water supply, the large use of fluoride dentifrices and the changes in the health services which accompanied the implementation of the Brazilian Unified Health System. Other important causes would be, in some countries, the consumption of sugar and the improvement in the life conditions of the population 10,16,21. The results found by the survey in Joinville demonstrated the decrease in the caries rates, confirming the findings in the aforementioned studies.
According to SB Brazil epidemiological survey 2, at 12 years-old, there are marked differences between the cities with and without water supply fluoridation. Joinville is a fluoridated city since 1979, so that 12-year-old children have already been receiving fluoride since their birth.
Conclusion
The 12-year-old students of the city of Joinville (SC) evaluated by this study exhibited a low prevalence of caries, reaching the rate advocated by WHO for 2010 8, fact that indicates that preventive and oral health promotion measurements for this age range are right on target. Other oral health epidemiological surveys should be conducted to monitor the epidemiological profile of this population.
References
1. Brasil. Ministério da Saúde. Secretaria Nacional de Programas Especiais de Saúde. Divisão Nacional de Saúde Bucal. Levantamento epidemiológico em saúde bucal: Brasil, zona urbana, 1986. Brasília; 1988. [ Links ]
2. Brasil. Ministério da Saúde. Coordenação Nacional de Saúde Bucal. Condições de saúde bucal da população brasileira – Projeto SB Brasil 2003: resultados principais. Brasília; 2004.
3. Brasil. Ministério da Saúde. Coordenação Nacional de Saúde Bucal. Pesquisa Nacional de Saúde Bucal – Projeto SB Brasil 2010. Brasília; 2009.
4. Brasil. Ministério da Saúde. Coordenação Nacional de Saúde Bucal. Condições de saúde bucal da população brasileira – Projeto SB Brasil 2010: resultados principais. Brasília; 2011.
5. Brasil. Ministério da Saúde. Secretaria de Gestão do Trabalho e da Educação na Saúde. PET Saúde. Brasília; 2011. [cited 2011 Jun 29]. Available from: URL:http://portal.saude.gov.br/portal/saude/profissional/visualizar_texto.cfm?idtxt=35306. [ Links ]
6. Cypriano S, Pecharki GD, Sousa MLR, Wada RS. A saúde bucal de escolares residentes em locais com ou sem fluoretação nas águas de abastecimento público na região de Sorocaba, São Paulo, Brasil. Cad Saúde Pública. 2003;19:1063-71. [ Links ]
7. Diagnóstico Social da Criança e do Adolescente de Joinville. [cited 2011 Oct 20]. Available from: URL:http://www.criancaeadolescentejlle.org/ind_ugs.html. [ Links ]
8. Frazão P. Epidemiologia em saúde bucal. In: Pereira AC (Org.). Odontologia em saúde coletiva: planejando ações e promovendo saúde. Porto Alegre: Artmed; 2003. p. 64-82. [ Links ]
9. Freire MCM, Reis SCGB, Gonçalves MM, Balbo PL, Leles CR. Condição de saúde bucal em escolares de 12 anos de escolas públicas e privadas de Goiânia, Brasil. Rev Panam Salud Publica. 2010;28(2):86-91. [ Links ]
10. Marcenes W, Bonecker MJS. Aspectos epidemiológicos e sociais das doenças bucais. In: Buischi YP (Org.). Promoção de saúde bucal na clínica odontológica. São Paulo: Artes Médicas; 2000. p. 75-98. [ Links ]
11. Nadanovsky P. O declínio da cárie. In: Pinto VG (Org.). Saúde bucal coletiva. São Paulo: Santos; 2000. p. 341-51. [ Links ]
12. Organização Mundial de Saúde. Levantamento epidemiológico básico de saúde bucal: manual de instruções. São Paulo: Santos; 1991. [ Links ]
13. Organização Mundial de Saúde. Levantamentos básicos em saúde bucal. 4. ed. São Paulo: Santos; 1999. [ Links ]
14. Pereira AC. Odontologia em saúde coletiva: planejando ações e promovendo saúde. Porto Alegre: Artmed; 2003. Cap. IV. [ Links ]
15. Pinto VG. Saúde bucal: panorama internacional. Ministério da Saúde. Secretaria Nacional de Programas Especiais de Saúde. Divisão Nacional de Saúde Bucal. Brasília; 1990. [ Links ]
16. Pinto VG. Índice de cárie no Brasil e no mundo. Rev Gaúcha de Odontologia. 1996;44:8-12. [ Links ]
17. Pinto VG. Epidemiologia das doenças bucais no Brasil. In: Kriger L (Org.). Promoção de saúde bucal. São Paulo: Artes Médicas; 1997. p. 24-41. [ Links ]
18. Pinto VG. Saúde bucal coletiva. 4. ed. São Paulo: Santos; 2000. p. 341-51. [ Links ]
19. Rouquayrol MZ. Epidemiologia e saúde. 4. ed. São Paulo: Medsi; 1994. [ Links ]
20. Secretaria Municipal da Saúde. Gerência de Atenção Básica. Área técnica da odontologia. Relatório do Levantamento Epidemiológico SB Brasil 2003. Joinville; 2003. [ Links ]
21. Traebert JL, Peres MA, Galesso ER, Zabot NE, Marcenes W. Prevalência e severidade da cárie dentária em escolares de seis e doze anos de idade. Rev Saúde Pública. 2001;35(3):283-8. [ Links ]
22. Weyne SC. A construção do paradigma de promoção de saúde: um desafio para as novas gerações. In: Kriger L (Org.). Promoção de saúde bucal. São Paulo: Artes Médicas; 1997. p. 1-26. [ Links ]
23. World Health Organization. Dental caries levels at 12 years, May 1994. The Oral Health Programme. Genebra; 1994. 19 p. [ Links ]
 Corresponding author:
Corresponding author:
Denise Vizzotto
Rua Eduardo Miers, n. 102, apto. 504 – Atiradores
CEP 89203083 – Joinville – SC – Brasil
E-mail: dvizzotto@brturbo.com.br
Received for publication: December 19, 2012
Accepted for publication: February 25, 2013
