










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
CASE REPORT ARTICLE
Preventive and surgical intervention in patient with cerebral palsy – case report
Gabriella Siqueira da MattaI; Maurício BarrivieraI; Andréia de Aquino MarsiglioI; Cláudia Maria de Souza PeruchiI; Alexandre Franco MirandaI
IDepartment of Dentistry for Special Patients, School of Dentistry, Catholic University of Brasília – Taguatinga – DF – Brazil.
ABSTRACT
Introduction: Cerebral palsy is defined as a non-progressive brain disorder of movement and posture. The patient is characterized by mental and motor disabilities, sensory impairments of vision and hearing, besides having seizures and contraction joints.
Objective: To address a multidisciplinary dental intervention in a patient, leucoderma, 11 years-old, with cerebral palsy who attended the Special Patients Clinic of the Catholic University of Brasilia, Brazil.
Case report: Clinical interventions to promote oral health, emphasizing the responsible guidelines regarding oral hygiene techniques, and surgical procedures such as extractions of deciduous teeth #75, #85, #63 (phase 1) and ulectomy in the region of teeth #24 and #25 (phase 2) were performed.
Conclusion: The multidisciplinary assistance targeted to the oral health of the patient with cerebral palsy can be considered as an important strategy for promoting the health and quality of life in this population group.
Keywords: disabled persons; cerebral palsy; oral health; quality of life.
Introduction
Cerebral palsy (CP) is a static brain lesion that may be defined as a non-progressive disorder of movement and posture. It is usually associated with epilepsy, and abnormalities of speech, hearing, vision and mental retardation, which can be determined by prenatal, perinatal, and postnatal factors 2,3.
Individuals with cerebral palsy are classified according to the changes of muscle tone and thetype of movement disorder that these individuals perform: spastic, athetoid, ataxic, hypotonic, and mixed 4,8.
The treatment aims palliative and rehabilitative mental and motor skills, however none of them is able to promote a full recovery of these patients 2,5.
Normally, these patients use anticonvulsant medications, epileptic drugs, which may interfere in oral health as cause gingival hyperplasia associated with the accumulation of biofilm due to the difficulty of performing oral hygiene and reduction in salivary flow 4,9,11.
Diseases of the oral cavity that affect these individuals are the same as those in the general population (caries, periodontal diseases, malocclusion, bruxism and enamel hypoplasia), but they occur more frequently in patients with CP, due to a number of factors associated such as poor oral hygiene, type and consistency of food, use of medications, tonicity of facial muscles, lack of information by the persons responsible for the patient and the lack of access to specialized dental services 12,13.
The dentist, doctors and healthcare professionals who treat patients with disabilities play an important role in health promotion and improvement in quality of life for these patients through multidisciplinary clinical planning, as in cerebral palsy patients who need special care 1,14,23.
The aim of this study was to report a clinical case in which preventive and surgical interventions were performed in a child with cerebral palsy attended at the clinic for Special Patients of the Catholic University of Brasilia, Brazil.
Case report
Patient diagnosed with chronic non-progressive encephalopathy (cerebral palsy), 11 years-old, male, was referred to dental evaluation at the Dental Clinic for Special Patients of the Catholic University of Brasília (UCB) for dental assessment because he presented motor disorder and a high degree of dependence in order to perform daily life activities such as correct oral hygiene (figure 1).
During the anamnesis, the mother reported that she had observed the presence of gingival bleeding and increase in volume in the region of teeth 24 and 25 because the patient insisted on keeping his hand in his mouth.
The doctor responsible for the patient was asked to provide a report on his present systemic condition, as well as the signing of the informed consent by the legal guardian, his mother, for the development and subsequent implementation of the dental treatment plan.
According to the neurological report, the patient presented mental retardation with an undetermined etiology, controlled behavior disorder, symptomatic generalized epileptic syndrome partially controlled by the use of anticonvulsant medications such as clonazepam, ten drops at night; topiramate 50 mg every 8 hours and 100 mg/day of phenobarbital.
At intraoral examination, it was observed the accumulation of biofilm, ogival palate, oroantral communication, anterior open bite, occlusal imbalance, eruption cyst in the region of teeth #24 and #25, semi-erupted teeth #15, #14, #21, #23, #25, #26 and #36, lingual position of the teeth #32 and #42, mesioangular position of teeth #31, #32, #41 and #42 and mobility of teeth #63, #75 and #85.
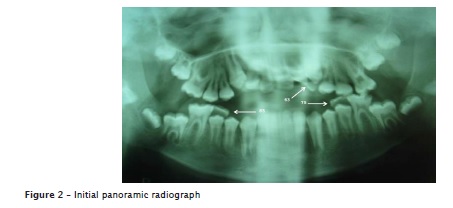
The panoramic radiograph showed the final stage of rhizogenesis in several teeth; advanced stage of rhyzolysis in teeth #63, #75 and #85; teeth #18, #28, #38 and #48 retained and at the beginning of coronal formation showing an early coronary formation (figure 2).
Aiming at reducing the amount of biofilm present, low speed prophylaxis was performed with fluoridated prophylactic paste, rubber cup and Robinson brush with the aid of a mouth opener made of wooden sticks and gauze. At this time, the mother received guidance on measures of oral health promotion, and instructions on how to make as well as the correct use of the mouth opener in order to make easier the patient's oral hygiene.
After clinical and radiographic analysis, the extractions of teeth #75, #85 and #63 were performed (figures 3A and 3B and 3C) in a single appointment. We performed the antisepsis of the oral cavity with gauze soaked into chlorhexidine 0.12% and then to the extraoral region the antisepsis was performed with topical PVPI. The local anesthetic used was Benzotop® 200 mg / g, infiltrative anesthesia was performed. For the entire process of extracting teeth, 1.5 vials of lidocaine hydrochloride 0.2%, 1:100,000 with adrenaline were used.
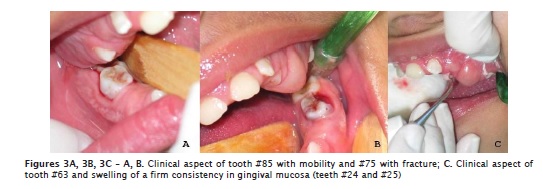
In the clinical analysis of the region of teeth #24 and #25, it was observed a swelling of a firm consistency, which had an aspect of normality (figure 3C). After the radiographic analysis of the region, the ulectomy surgery was indicated after 15 days. This procedure was carried out following pre-surgical approaches previously reported.
For the surgical procedure, infiltration anesthesia was performed in the middle superior alveolar nerve and complementary anesthesia with infiltrative terminals using two vials of 2% lidocaine with 1:100,000 adrenaline. Subsequently, an elliptical incision was made with a size 11 scalpel blade on the edge of the fibrous gingival, contributing to immediate exposure of the occlusal surface of the teeth #24 and #25. Compression was performed in the area with gauze soaked into chlorhexidine 0.12% (figure 4). At the post-operative period, paracetamol 200 mg every 6 hours for 3 days was prescribed and the mother was instructed to clean the area with 0.12%chlorhexidine. The biopsies removed during surgery were sent for histopathological examination at the Catholic University of Brasilia, confirming the diagnosis of eruption cyst.

One week later, the patient returned for clinical reassessment and the area submitted to surgical intervention was in favorable healing conditions and greater exposure of the coronal region of teeth #24 and #25 (figures 5A, 5B).

For the patient's comfort, all the procedures were performed while he was sitting in the wheelchair.
Discussion
Cerebral palsy (CP) describes a group of movement and posture developmental disorders attributed to non-progressive disturbances in the brain of the developing fetus or child causing limitations in daily activities. It is commonly associated with epilepsy, abnormalities of the senses and mental retardation 4,24 therefore, justifying the need to adopt special, intensive and above all, individual care of patients with cerebral palsy, particularly during preventive and minimal dental interventions 2,11,14.
Dental evaluation of the patient with cerebral palsy must be made by careful anamnesis associated with multidisciplinary planning in conjunction with the other health professionals and family members involved 6,15,17.
The dentist plays an important role in the quality of life of patients with cerebral palsy, because the problems in the oral cavity may contribute to a poor quality of life of these special patients 10,18,25.
These patients have a higher predisposition to diseases of the oral cavity such as caries, periodontal diseases, malocclusion, bruxism and enamel hypoplasia with greater frequency than that in the general population 16,19,21,22,24, with some features present in the reported case.
According to Maranhão 12, Nallegowda et al. 14 and Previtali and Santos 16, poor oral hygiene in patients with cerebral palsy is characterized by the inability of these individuals in brushing their teeth and family difficulty in opening their mouths. Thus, there is a need for guidance and training of those responsible to promote oral health.
Guidance on the types and frequency of ingestion of food and oral hygiene techniques are important in the routine of patients with cerebral palsy, especially the use of adaptations, such as the use of wooden spatulas to facilitate opening of the oral cavity of a CP, as described in the case report 7,19,27.
The main difficulty encountered by dentists today is being able to safely perform clinical procedures in these patients, once cerebral palsy is not a negative condition to treatment. If the treatment is properly planned in a multidisciplinary group, invasive procedures can be performed normally 6,9,17.
The dental surgical procedures in patients with cerebral palsy should promote the quality of health of the individual, performed in stages, because these patients cannot stay long in the dental chair. Importantly, clinical activities should always be done by a well trained staff at four hands, in addition to external support, as reported 1,15,26.
It is important to the dentist to have the knowledge on the systemic condition of the individual with CP, drug interactions and the handling of negative side effects 12,15,18.
Several types of physical and mechanical restrictions have been described and used in dental treatment of people with special needs 17, however, no protocol for positioning the patient for ambulatory dental attendance was found, in order to reduce the postural instability caused by the patient's increased muscular tonus and inhibition of reflexes such as the asymmetry of the tonic reflex of the neck, frequently observed in these patients 2,14. However, for the patient's greater comfort all the procedures reported here were performed while he was sat on his own wheelchair 18,20.
Some suggestions should be followed for an adequate clinical attendance, such as: good positioning of the patient, in which the patient is comfortable and does not cause any undesired reflex; the use of immobilizer and mouth openers 17,20. The purpose of all these measures and others are focused on the success of treatment and well-being of the special patient 2,6,9.
The clinical follow-up of patients with cerebral palsy by the dentist should be continuous, respecting the patient's real needs, behaviors performed by the family for the maintenance of oral health and clinical procedures performed 19,25,26, as described.
The ideal dental attendance for the patient with cerebral palsy is early prevention, especially with the active participation of parents or relatives in the process of introducing oral hygiene care and associated with the specialized ambulatory treatment of these patients 2,6,15,17,18.
Conclusion
It can be concluded that the multidisciplinary approach to execute the oral health care of the patient with cerebral palsy, as reported, may be considered as an important strategy in promoting health and quality of life.
References
1. Abanto J, Carvalho TS, Bonecker M, Ortega AO, Ciamponi AL, Raggio DP. Parental reports of the oral health-related quality of life of children with cerebral palsy. BMC Oral Health. 2012;18:12-5. [ Links ]
2. Abreu MHNG, Paixão HH, Resende VLS. Cerebral palsy carriers: important aspects in dentistry. Arq Odontol. 2001;37:53-60. [ Links ]
3. Bax M, Goldstein M, Rosebaun P. Proposed definition and classifications of cerebral palsy. Rev Med Child Neurol. 2005;47:571-6. [ Links ]
4. Costa PHM, Costa MABT, Pereira FM. The clinic-epidemiological profile of patients with cerebral palsy treated in a dentistry center in Distrito Federal, Brazil. Com Ciências Saúde. 2007;18(2):129-39. [ Links ]
5. De Carvalho RB, Mendes RF, Prado Jr RR, Moita Neto JM. Saúde bucal e função motora oral em crianças com paralisia cerebral. Spec Dentist Care. 2011;31(2):58-62. [ Links ]
6. De Oliveira Andrade PM, De Oliveira Ferreira F, Haase VG. Multidisciplinary perspective for cerebral palsy assessment after an international, classification of functioning, disability and health training. Dev Neurorehabi. 2011;14(4):19999-207. [ Links ]
7. Dougherty NJ. A review o cerebral palsy for the oral health professional. Dent Clin North. 2009;53(2):329-38. [ Links ]
8. Guerreiro PO, Garcias GL. Oral health conditions diagnostic in cerebral palsy individuals of Pelotas, Rio Grande do Sul State, Brazil. Ciência & Saúde Coletiva. 2009;14(5):1939-46. [ Links ]
9. Haddad AS. Odontologia para pacientes com necessidades especiais. São Paulo: Editora Santos; 2007. [ Links ]
10. Katz CR. Integrated approach to outpatient dental treatment of a patient with cerebral palsy: a case report. Spec Care Dentist. 2012;32(5):210-7. [ Links ]
11. Manrique D, Melo ECM, Buhler RB. Alterações nasofibrolaringoscópicas da deglutição na encefalopatia crônica não-progressiva. J Pediatr. 2002;77(1):67-70. [ Links ]
12. Maranhão MVM. Anestesia e paralisia cerebral. Rev Bras Anestesiol. 2005;55(6):680-702. [ Links ]
13. Mayson M. People with cerebral palsy: effects of and perspectives for therapy. Neural Plast. 2001;8(51):51-69. [ Links ]
14. Nallegowda MBBS, Mathur BDS, Singh U, Prakash H, Khanna M, Sachdev G et al. Oral health status in indian children with cerebral palsy- a pilot study. IJPMR. 2005;16(1):1-4. [ Links ]
15. National Institutes of Health. Practical oral care for people with intellectual disability. Todays FDA. 2010;22(1):53-9. [ Links ]
16. Previtali EF, Santos MTBR. Dental caries and oral hygiene in children with spastic tetraparetic cerebral palsy receiving either oral feeding or nutrition via gastrostomy tube. Pesq Bras Odontoped Clín Integr. 2009;9(1):43-7. [ Links ]
17. Ribeiro G, Braga MBP, Simões RA. Pacientes com desvios neurológicos: métodos alternativos de prevenção e atendimento. Rev Fac Odontol Anápolis. 2004;6(1):1-6. [ Links ]
18. Santos ATL, Couto GBL. Dental attendance to palsy patient. Int J Dent. 2008;7(2):133-41. [ Links ]
19. Santos MTBR, Guare RO. Caries experience in individuals with cerebral palsy in relation to oromotor dysfuncion and dietary consistency. Spec Care Dentist. 2009;29(5):198-203. [ Links ]
20. Santos MTBR, Manzano FS. Assistive stabilization based on the neurodevelopmental treatment approach for dental care in individuals with cerebral palsy. Quint Int. 2007;38(3):681-7. [ Links ]
21. Santos MTBR, Masiero D, Simionato MRL. Risk factors for dental caries in children with cerebral palsy. Spec Care Dentist. 2002;22:103-7. [ Links ]
22. Santos MTBR, Masiero D, Novo NF, Simonato MRL. Oral conditions in children with cerebral palsy. Spec Care Dentist. 2003;70:40. [ Links ]
23. Santos MTBR, Nogueira MLG. Infantile reflexes and their effects on dental caries and oral hygiene in cerebral palsy individuals. J Oral Rehab. 2005;32(12):880-5. [ Links ]
24. Shinkai RSA, Santos LM, Silva FAE, Santos MN. Contribuição ao estudo da prevalência de bruxismo excêntrico noturno em crianças de 2 a 11 anos de idade. Rev Odontol Univ São Paulo. 199998;12(1):29-37. [ Links ]
25. Souza AL, Horta CAB, Silva CATM, Miranda DK. Saúde bucal de pacientes portadores de necessidades especiais com paralisia cerebral. Rev Paraense. 199997;2:11-8. [ Links ]
26. Staufer K, Hamadeh S, Gesch D. Failure of tooth eruption in two patients with cerebral palsy and bruxism – a 10 years follow up: a case report. Spec Care Dentist. 2009;29(4):169-74.
27. Vivone GP, Tavares MMM, Bartolomeu RS, Nemr K, Chiappetta ALML. Analysis of alimentary consistency and deglutition time in children with spastic quadriplegic cerebral palsy. Rev CEFAC. 2007;9(4):504-11. [ Links ]
 Corresponding author:
Corresponding author:
Alexandre Franco Miranda
Universidade Católica de Brasília – Curso de Odontologia
Clínica de Odontologia para Pacientes Especiais – Campus I – QS 07 – Lote 01 – EPCT
E-mail: alexandrefmiranda@hotmail.com
Received for publication: July 20, 2012
Accepted for publication: February 22, 2013
