










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.3 Joinville Jul./Set. 2013
CASE REPORT ARTICLE
Pleomorphic adenoma in the oral mucosa of a young adult: a case report
Juliana Andrade CardosoI; Carla Martins FerreiraI; Mariana Moura de Jesus Fernandes GuerraI; Gleicy Gabriela Vitória Spinola Carneiro FalcãoI; Lívia Souza PuglieseI; Jener Gonçalves de FariasI
IDepartment of Dentistry, Metropolitan Union of Education and Culture – Lauro de Freitas – BA – Brazil.
ABSTRACT
Introduction: The pleomorphic adenoma (PA) is the most common benign neoplasia in salivary glands, affecting most commonly the parotid gland of females between the 4th and 6th decades of life. PA can less commonly affect the minor salivary glands; in these cases the main site of attack is the palate.
Objective: This study aims are twofold: to report a clinical case of PA involving minor salivary glands in the oral mucosa, treated conservatively; and to emphasize the importance of pathologic examination in defining the correct diagnosis.
Case report: A 22 year-old melanoderm male patient sought emergency room due to asymptomatic swelling in the right side of the face. After comprehensive clinical examination, it was decided to perform an incisional biopsy to confirm the diagnosis and further treatment. After confirming the diagnosis of pleomorphic adenoma, we opted for enucleation of the lesion to avoid possible complications such as scar retraction and salivary fistula.
Conclusion: It is very important that the dentist early diagnoses the neoplasia to perform more conservative treatments and achieve a better prognosis for the patient, always following-up the case for a period from five to ten years to ensure the non-recurrence of this neoplasia.
Keywords: pleomorphic adenoma; neoplasms; salivary glands.
Introduction
The pleomorphic adenoma (PA) is the most common tumor affection the salivary glands 7,8, accounting for 33.2% to 89.9% of the cases, followed by carcinomas. 7. The parotid gland is the most affected 8,11, followed by the submandibular and minor salivary glands, which have been lesser affected 8. Considering the minor salivary glands, the palate is the place mostly affected 11.
Clinically, PA of minor salivary glands is a single, solid, smooth, well-delimited structure. This tumor is composed of a single mass that is encapsulated and consequently shows mobility, except when the lesion occurs in the palate. Generally, PA is asymptomatic and has a slow development 2,5,6,10.
Some lesions of the salivary glands exhibit similar clinical, histopathological and imaging aspects, which can compose a differential diagnosis of PA 6. PA may affect the hard palate, which has been the site of most of the malign neoplasias such as adenocarcinoma; and it may affect the parapharyngeal space, a common site for lipoma, therefore limiting and making difficult the diagnosis by clinical aspects. Thus, to obtain a correct differential diagnosis, complementary examinations are required 9,11.
The imaging examinations, such as ultrasonography, computed tomography and magnetic resonance, help in the diagnosis of the lesions because they established their origin, location and limits 9. Notwithstanding, microscopic examinations are essential to define the diagnosis because they show the histopathological aspects of the lesions differing the sound cells from the tumoral ones 2,9,12.
PA early diagnosis enables a more conservative treatment by preventing the bone and tissue infiltration of the lesion l 5. The election treatment is the surgical excision by resection with a safe margin of 3 to 5 mm 10, because the lesion may relapse frequently according to its location and surgical technique applied. Normally, the post-operative period is uneventful with complete healing by 15 days. The patient must be followed-up for five years. The appropriate treatment is of extreme importance to reach a good prognosis, therefore avoiding the lesion relapse. A good surgical technique shows a healing rate of 95% 6.
The aim of this study was to report a clinical case of pleomorphic adenoma affecting the minor salivary gland and to discuss its characteristics, emphasizing the important role of the dentist in the correct and early diagnosis of this lesion, resulting in a more conservative treatment and better prognosis for the patient.
Case report
A 22-year-old melanoderm, male patient was referred to the clinic of Specialization in Stomatology of the Metropolitan Union of Education and Culture with chief complaint of a swelling in the right side of the face. The patient was accompanied by his parents.
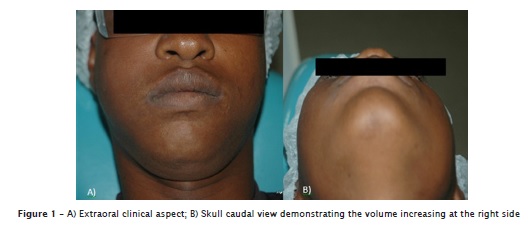
At extraoral physical examination, a facial asymmetry in the right side of the face was observed so that the nasolabial fold disappeared (figure 1).
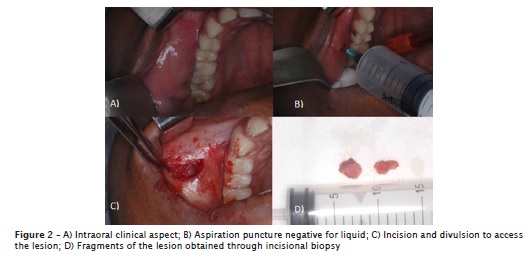
During intraoral physical examination, a tumor lesion could be seen in the buccal mucosa covered by sound tissue, well delimited, with a firm consistency and mobility to palpation. The patient signed a free and clarified consent form. An incisional biopsy under local anesthesia was chosen to define the lesion histopathologically. Firstly, an aspiration puncture was executed aiming to evaluate the lesion type: liquid or solid. No liquids were aspired, so that according to the lesion location and solid aspect the clinical diagnosis proposed was of lipoma (figure 2).
However, the histopathological examination concluded that lesion was a pleomorphic adenoma.
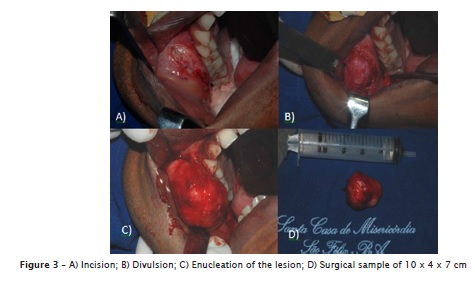
Then, the patient was admitted in the Service of Stomatology and Buccomaxillofacial Surgery of the Holly House Hospital of São Felix, Bahia, Brazil to be submitted to the lesion enucleation under general anesthesia (figure 3).
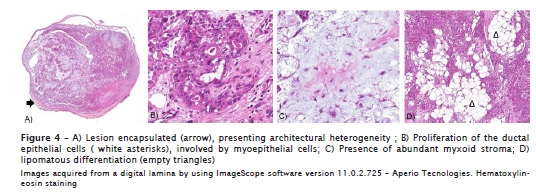
The sample was referred to the service of pathological anatomy of the Metropolitan Union of Education and Culture which confirmed the diagnosis of pleomorphic adenoma (figure 4).
After fifteen days, the post-operative period was uneventful and the sutures were removed, but there was still a little face asymmetry due to the residual swelling (figure 5).
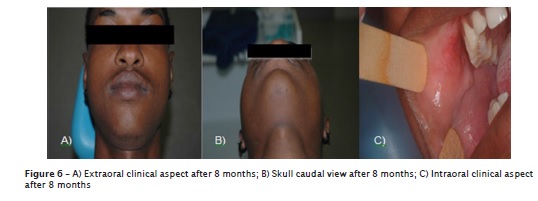
After 8 post-surgery months, the patient exhibited no signs of lesion relapse and good face symmetry (figure 6). The patient is still undergoing 1-year follow-up in the clinic of Specialization in Stomatology for at least 5 years.
Discussion
According to previous studies, PA occurs most frequently in the parotid gland, followed by submandibular glands and less frequently the minor salivary glands 8,11. The area main affected by PA of minor salivary glands is the hard and soft palate, corresponding from 42.2% to 55% of the cases, followed by the lips with 14% to 18.5% of the cases and oral mucosa in 15% of the cases 1,2,7,9. PA predominantly occurs in Caucasian females between the 4th and 6th decades of life aging from 43 to 46 years in average 1,2,4,7,9,13. This aspect differs from those of this present case report in which PA occurred in a melanoderm male patient at the third decade of life. During the intraoral physical examination, clinical aspects similar to those reported in the literature were observed, such as single submucosal tumor lesion of firm consistency and with mobility to palpation 2,5,6,10.
The histopathological examination confirmed the diagnosis of PA because of the abundant and heterogeneous presence of myoepithelial cells in tubular arrangement, glandular epithelium with ductiform structures, and with transformation of the stroma by exhibiting a myxoid and adipose tissue, which is in agreement with the aspects previous reported in the literature 2,9,12.
Because the buccal mucosa is not a very common site of PA appearance 3, and the patient was a young melanoderm male adult, facts that disagree with the literature 1,2,4,7,9,13, the first diagnosis option suggested in this present case report was of lipoma.
By reviewing the literature, the treatment recommended is the surgical excision by resection with a safe margin from 3 to 5 mm 5,6,10. Notwithstanding, in this case report, an enucleation was chosen because the lesion showed great dimensions, therefore avoiding some complications as scar retraction and salivary fistula. Thus, it is necessary to perform a careful following-up of at least five years because of the probability of relapse.
Conclusion
Because PA is a neoplasia with great diversity of cells in constant process of transformation, it demands a correct surgical procedure with safe margin to assure that the surgical site is free of tumoral cells.
It is worth emphasizing the important role of the dentist in executing the early diagnosis of the neoplasia to conduct more conservative treatments and obtain a better prognosis for the patient, always following-up the case for a period from five to ten years to ensure the non-recurrence of this neoplasia.
References
1. Bettio A, Salgado G, Azevedo-Alanis LR, Machado MAN, Grégio AMT, Lima AAS. Prevalência das lesões de glândulas salivares em laudos histopatológicos do Laboratório de Patologia Experimental da PUCPR. RSBO. 2009 Sep;6(3):231-6. [ Links ]
2. Boros FL, Júnior JB, Boros FL, Boros LH, Silva PA. Adenoma pleomórfico de glândula salivar menor do palato. Odontologia Clín-Científ. 2004 Jan-Apr;3(1):67-72. [ Links ]
3. Dalati T, Hussein MR. Juvenile pleomorphic adenoma of the cheek: a case report and review of the literature. Diagn Pathol [serial online] 2009 Sep;4(32):[5 screens] [cited 2012 Oct 19]. Available from: URL:http://www.diagnosticpathology.org/content/4/1/32. [ Links ]
4. Jorge J, Pires FR, Alves FA, Perez DE, Kowalski LP, Lopes MA et al. Juvenile intraoral pleomorphic adenoma: report of five cases and review of the literature. Int J Oral Maxillofac Surg. 2002 Jun;31(3):273-5. [ Links ]
5. Lacerda SA, Socolowski F, Rosa AL, Ferraz MP, Brentegani LG. Adenoma pleomórfico intra-ósseo no maxilar: relato de caso clínico. Rev Bras Estomatol. 2005;2(4):5-8. [ Links ]
6. Lawall MA, Simonato LE, Ribeiro ACP, Crivelini MM, Moraes NP. Adenoma pleomórfico: relato de caso clínico. Rev Odontol. 2007 Sep-Dec;19(3):336-40. [ Links ]
7. Loiola RS, Matos FR, Nonaka CFW, Lopes FF, Cruz MCFN. Perfil epidemiológico das neoplasias de glândulas salivares diagnosticadas em São Luís-MA. J Bras Patol Med Lab. 2009 Oct;45(5):413-20. [ Links ]
8. Rao PK, Shetty SR, Hegde D. Ectopic pleomorphic adenoma. N Am J Med Sci. 2012 Apr;4(4):190-2. [ Links ]
9. Ribeiro-Rotta RF, Cruz ML, Paiva RR, Mendonça EF, Spini TH, Mendonça AR. O papel da ressonância magnética no diagnóstico do adenoma pleomórfico: revisão da literatura e relato de casos. Rev Bras Otorrinolaringol. 2003 Sep-Oct;69(5):699-707. [ Links ]
10. Santiago LM, Torres BCA, Andrade MC, Silva UH, Santana AF, Santos EV. Adenoma pleomórfico em lábio superior. Odontologia Clín-Científ. 2005 Jan–Apr;4(1):63-70.
11. Sharma Y, Maria A, Chhabria A. Pleomorphic adenoma of the palate. Natl J Maxillofac Surg. 2011 Jul;2(2):169-71. [ Links ]
12. Teixeira JM, Cornélio SS, Grillo JPF, Pontes JRM, Ramos MEB, Israel MS. Adenoma pleomórfico en labio superior: relato de caso. Acta Odontol Venez. 2007 Sep;45(3):440-2. [ Links ]
13. Wang D, Li Y, He H, Liu L, Wu L, He Z. Intraoral minor salivary gland tumors in a Chinese population: a retrospective study on 737 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 Jul;104(1):94-100. [ Links ]
 Corresponding author:
Corresponding author:
Juliana Andrade Cardoso
Avenida Praia de Itamaracá, quadra B3, lote 24 – Vilas do Atlântico
CEP 42700-000 – Lauro de Freitas – BA – Brasil
E-mail: juliandradec@gmail.com
Received for publication: August 13, 2012
Accepted for publication: January 29, 2013
