










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.10 no.4 Joinville Out./Dez. 2013
Case Report Article
Use of electronic apex locator in the impossibility of radiographic visualization of the root apex: report of two cases
Ricardo Machado I; Luiz Fernando Tomazinho I; Ângela Mayara Azedo Stel I; Emmanuel João Nogueira Leal Silva II; Luiz Pascoal Vansan III
I Ingá University – Rondonópolis – AC – Brazil
II Grande Rio University – Duque de Caxias – RJ – Brazil
III University of São Paulo – Ribeirão Preto – SP – Brazil
ABSTRACT
Introduction: Electronic apex locators have been widely used for foraminal identification and for working length determination. The establishment of a correct apical limit is essential for a good prognosis in cases of pulp vitality or pulp infection. Objective and Case reports: The aim of the study is to report two cases where the use of electronic apex locators was crucial due to the inability to visualize the root apex due to a post-surgical retaining plate (case 1) and during orthodontic treatment with a maxillary expander (case 2). Conclusion: In this light we could confirm the effectiveness of these devices for the determination of the working length when it is impossible to perform it by radiographic techniques.
Keywords: Endodontics; root apex; working length determination.
Introduction
The correct working length determination is crucial for the endodontic treatment success because it ensures that the cleaning and shaping process and filling material remains are restricted to the root canal space avoiding possible damage to the perirradicular tissues 1. Failures during this stage can result in sub or overinstrumentation increasing significantly treatment failure 8,20,23.
The use of different radiographic techniques is the most common method for working length determination 11,18. However, some limitations are considered relevant to the establishment of precise measurements. Radiographic examination provides a two-dimensional image of a three-dimensional structure. Furthermore, in some situations, the projection of anatomical structures or another structures, can avoid an adequate visualization of the radiographic apex. Due to these limitations, several methods have been developed for determine the correct working length, such as the electronic apex locators (EALs). Most studies have reported high success rates even in adverse situations such as the presence of blood or exudates, large apical foramen and resorptions 1-3,13,16,21,22.
The aim of this paper is to present two cases where the use of electronic apex locators was essential for working length determination because of the inability to visualize the root apex after a surgery with the use of metallic structures (case I) and during orthodontic treatment (case II).
Case reports
Case 1
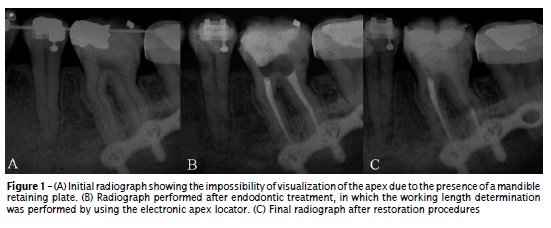
A 37 year-old female patient was referred to the office of one of the authors (RM) for emergency intervention in tooth #36. The patient complained of spontaneous pain during the night. Clinical examination revealed no periodontal involvement. Thermal and complementary tests have suggested a diagnosis of irreversible pulpitis. Radiographically, it was possible to observe a mandibular metallic retaining plate preventing a complete visualization of the roots (figure 1A).
After nerve block with Articaine 4% and epinephrine 1:100.000 (Articaine – DFL Indústria e Comércio Ltda., Rio de Janeiro/RJ, Brazil), placement of rubber dam and cleaning of the operative field with sodium hypochlorite 2.5% (Fórmula & Ação, São Paulo/SP, Brazil), the initial access was carried out with the aid of 1016HL, EndoZ and 3083 burs (KG Sorensen, Barueri/SP, Brazil). Then, the preparation of the cervical and middle thirds 24 was performed with SX, S1 and S2 instruments (Dentsply/Maillefer, Ballaigues, Switzerland). The working length was determined by using an electronic apex locator – Elements Diagnostic Apex Locator – (SybronEndo, Orange County, CA). For this purpose, a 0.02 taper size #15 K-File (Tulsa Dental Specialties, Tulsa, OK) was inserted into the canals until the reading of 0.5, then advanced slowly until the word apex flashed, and finally withdrawn until the reading of 0.5 showed again. The stopper was positioned at the coronal reference and the file removed. The length from the file tip to the stopper was measured with an endodontic hand ruler (Angelus, Londrina, Brazil). Posterior instrumentation of mesial canals was performed with size 04 Profile System (Dentsply/Maillefer, Ballaigues, Switzerland) until size 35 instrument . The distal canal was instrumented manually using a Crown-Down technique until size 50 K-File. Irrigation was performed with 2.5% sodium hypochlorite (Formula & Ação, São Paulo/SP, Brazil). After instrumentation, 17% EDTA was used for 3 minutes and the canals were dried after using 5 ml of saline solution. Endodontic filling was performed using lateral condensation and AH Plus sealer (Dentsply DeTrey, Konstanz, Germany) and the temporary restoration performed with Cimpat (Septodont, São Paulo/SP, Brazil) (figure 1B).
In the following visit, after nerve block with Articaine 4% and epinephrine 1:100,000, placement of rubber dam and cleaning of the operative field with 2.5% sodium hypochlorite, the temporary restoration was removed, followed by the partial removal of the filling in the distal canal with Gates Glidden drills (Dentsply Maillefer, Ballaigues, Switzerland), proof of the fiberglass post (Fiberpost – Angelus, Londrina/PR, Brazil), post cementation with resin cement Rely X (3M Brazil Ltda., Sumaré/SP, Brazil) and restoration with resin composite Z250 (3M Brazil Ltda., Sumaré/SP, Brazil) (figure 1C).
Case 2
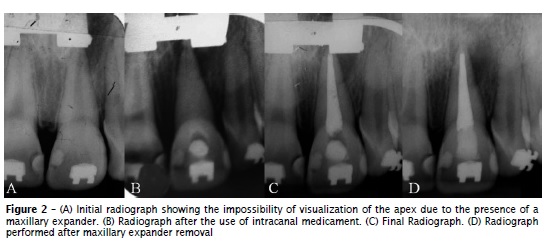
A 12 years old female patient was referred to the emergency clinic of the Specialization in Endodontics Course of Ingá University, Rondonópolis/AC, Brazil presenting spontaneous pain in the anterior upper left maxillary region. Clinical examination revealed the presence of a maxillary expander and swelling in the buccal side. Thermal and additional tests have suggested pulp necrosis of tooth #21. Radiographically, it was observed a periapical lesion and that part of the root apex was covered by the maxillary expander (figure 2A).
After infiltrative anesthesia with 2% mepivacaine and epinephrine 1:100,000 (Mepivacaine – DFL Indústria e Comércio Ltda., Rio de Janeiro/RJ, Brazil), placement of rubber dam and cleaning of the operative field with 2.5% sodium hypochlorite (Fórmula & Ação, São Paulo/SP, Brazil), initial access was performed with 1014HL and 3082 drills (KG Sorensen, Barueri/SP, Brazil). The neutralization of the septic content was carried out with a size 20 K file (SybronEndo, Lone Hill/CA, USA) associated with profuse irrigation with 2.5% sodium hypochlorite (Formula & Ação, São Paulo/SP, Brazil) . After preparation of the cervical and middle thirds 24 with Gates Glidden drills (Dentsply-Maillefer, Ballaigues, Switzerland), working length determination was performed with the use of an electronic apex locator (Ipex – NSK, Kanuma-City, Japan). For this purpose, a 0.02 taper size #20 K-File (Tulsa Dental Specialties, Tulsa, OK) was inserted into the canal until the reading of 0.5, then advanced slowly until the word apex flashed, and finally withdrawn until the reading of 0.5 again. The stopper was positioned at the coronal reference and the file removed. The length from the file tip to the stopper was measured with an endodontic hand ruler (Angelus, Londrina, Brazil). Instrumentation was performed with K-files following a Crow Down technique until size #80 file (SybronEndo, Lone Hill/CA, USA). Irrigation was performed at every instrument change with 2.5 ml of 2.5% sodium hypochlorite (Fórmula & Ação, São Paulo/SP, Brazil). Then, after the use of 17% EDTA (Fórmula & Ação, São Paulo/SP, Brazil), the canal was filled with a calcium hydroxide paste (Calen, SS White Dental Products Ltd. ., Rio de Janeiro/RJ, Brazil) and the pulp chamber was sealed temporarily with Cimpat (Septodont, São Paulo/SP, Brazil) (figure 2B). In the following visit, performed 30 days later, it was decided to continue using the medication due to the presence of exudate.
After more 20 days, following the completion of the previously described procedures, calcium hydroxide was removed by use of K-Files and profuse irrigation with 2.5% sodium hypochlorite (Fórmula & Ação, São Paulo/SP, Brazil). After using the chelating solution for 3 minutes (17% EDTA – Fórmula & Ação, São Paulo/SP, Brazil), the canal was dried and the filling was performed by lateral condensation and Sealer 26 (Dentsply, Petrópolis/RJ, Brazil). The coronal sealing was performed with Cimpat (Septodont, São Paulo/SP, Brazil) (figure 2C).
In the following visit, coronal sealing was removed with 1014 drills (KG Sorensen, Barueri / SP, Brazil) for performing the final restoration with composite resin Z250 (3M Brazil Ltda., Sumaré/SP, Brazil). After three months of the orthodontic treatment conclusion, a follow-up radiograph was performed showing the proper apical limit (figure 2D).
Discussion
Most part of randomized clinical trials conducted to evaluate rates of success and failure in endodontics demonstrated the influence of the working length determination on treatment outcomes 6,10,19.
Because of the limitations of the radiographic techniques used for the working length determination, the electronic apex locators have been widely used aiming to increase certainty and predictability. Since its inception in the 50s, these facilities have been upgraded and undergone major changes in its working principle and become more reliable and accurate, regardless of the clinical situation found 1-3,13,16,21,22.
Among the main advantages of the electronic working length determination, three points have been consistently cited in the literature: a) the reduction of radiation 7,14, b) the location of the main apical foramen that allows to perform an instrumentation quite near to the apical constriction 9,15 and c) the easier working length determination in the impossibility of a correct visualization of the roots 2.
In this paper, two clinical situations were presented showing the impossibility of adequate working length determination using radiographic techniques because of other treatments together with the endodontic therapy.
In case 1, during the interview, the patient reported having undergone a surgical procedure for Figure 2 – (A) Initial radiograph showing the impossibility of visualization of the apex due to the presence of a maxillary expander. (B) Radiograph after the use of intracanal medicament. (C) Final Radiograph. (D) Radiograph performed after maxillary expander removalcorrection of mandibular repositioning by occlusal compromises. The use of splints used in facial surgery has been widely reported in the literature aiming the restructuring the facial skeleton, particularly in cases of temporomandibular disorders and correction of mandibular damage resulting from trauma 5,12. In our case, even using different radiographic techniques with variations of vertical angle, it was not possible to have a correct visualization of the root apex. This factor was crucial to the use of electronic apex locator in order to perform a proper treatment.
In case 2 it was possible to visualize the maxillary expander for the orthodontic and occlusal rehabilitation of a young patient 4,17. As described above, this device does not allow the radiographic working length determination and the use of the foraminal apex locator was very important for a safer treatment. In this specific case, an incorrect working length determination could lead to the maintenance of infection and leakage of contaminated debris in case of sub or overinstrumented, respectively. Both could significantly compromise the prognosis of the treatment 8,20,23.
Conclusion
The cases showed in this paper indicated the effectiveness of electronic apex locators to determine the working length when the impossibility of carrying out the radiographic method.
References
1. Beltrame PCA, Triches TC, Sartori N, Bolan M. Electronic determination of root canal working length in primary molar teeth: an in vivo and ex vivo study. Int Endod J. 2011;44:402-6. [ Links ]
2. Cianconi L, Angotti V, Felici R, Conte G, Mancini M. Accuracy of three electronic apex locators compared with digital radiography: an ex vivo study. 6J Endod. 2010;36:2003-7.
3. Coutinho-Filho TS, Silva EJ, Magalhães KM, Krebs RL, Ferreira CM, Natividade CO. Avaliação in vitro da eficácia do localizador apical Joypex 5. Rev Odontol Bras Central. 2012;21:411-4.
4. Derton N, Gracco A, Procopio O. Surgical and orthodontic treatment of skeletal Class III featuring severe transversal and sagittal discrepancy. Int Orhtod. 2012;10:148-64.
5. Erkan M, Karaçay Ş, Atilla OA, Uzel G, Ülkür E, Yildirim E. Orthognathic surgery of a patient with oligodontia: alternative technique for intermaxillary fixation. J Craniofac Surg. 2012;23:407-10.
6 . Fleming CH, Litaker MS, Alley LW, Eleazer PD. Comparison of classic endodontic techniques versus contemporary techniques on endodontic treatment success. J Endod. 2010;36:414-8.
7. Fouad AF, Reid L. Effect of using electronic apex locators on selected endodontic treatment parameters. J Endod. 2000;26:364-7.
8. Glossary of endodontic terms. 7. ed. Chicago: American Association of Endodontists; 2003.
9. Grimberg F, Banegas G, Chiacchio L, Zmener O. In vivo determination of root canal length: a preliminary report using the Tri Auto ZX apex locating handpiece. Int Endod J. 2002;35:590-3.
10. Imura N, Pinheiro ET, Gomes BPFA, Zaia AA, Ferraz CCR, Souza-Filho FJ. The outcome of endodontic treatment: a retrospective study of 2000 cases performed by a specialist. J Endod. 2007;33:1278-82.
11. Ingle JI. Endodontic instruments and instrumentation. Dent Clin N Amer. 1957;805:22.
12. Ishihara Y, Kuroda S, Nishiyama A, Sasaki A, Takano-Yamamoto T, Yamashiro T. Functional improvements after orthodontic-surgical reconstruction in a patient with multiple maxillofacial fractures. Am J Orthod Dentofacial Orthop. 2012;142:534-45.
13. Janner SF, Jeger FB, Lussi A, Bornstein MM. Precision of endodontic working length measurements: a pilot investigation comparing cone-beam computed tomography scanning with standard measurement techniques. J Endod. 2011;37:1046-51.
14. Katz A, Tamse A, Kaufman AY. Tooth length determination: a review. Oral Surg Oral Med Oral Pathol. 1991;72:239-42.
15. Kobayashi C, Suda H. New electronic canal measuring device based on the ratio method. J Endod. 1994;20:111-4.
16. Miguita KB, Cunha RS, Davini F, Fontana CE, Bueno CES. Comparative analysis of two electronic apex locators in working length determination at endodontic therapy – an in vitro study. RSBO. 2011 Jan-Mar;8(1):25-9.
17. Miller P, Iyer M, Gold AR. Treatment resistant adolescent depression with upper airway resistance syndrome treated with rapid palatal expansion: a case report. J Med Case Rep. 2012;4:415.
18. Paiva JG, Antoniazzi JH. Endodontia: bases para prática clínica. 2. ed. São Paulo: Artes Médicas; 1984.
19. Pettiette MT, Delano EO, Trope M. Evaluation of success rate of endodontic treatment performed by students with stainless-steel k-files and nickel-titanium hand files. J Endod. 2001;27:124-7.
20. Ricucci D. Apical limit of root canal instrumentation and obturation, part 1. Literature review. Int Endod J. 1998;31:384-93.
21. Silva EJ, Herrera DR, Santos CC, Gomes BP, Zaia AA. Acuidade do Root ZX II utilizando limas de aço-inoxidável e de níquel-titânio. Dent Press Endod. 2011;1:41-4.
22. Soares NV, Silva EJ, Ferreira CM, Krebs RL, Coutinho-Filho TS. Clinical reproducibility of a low cost electronic apex locator. Braz J Oral Sci. 2012;11:112-5.
23. Stoll R, Betke K, Stachniss V. The influence of different factors on the success of root canal fillings – a ten-year retrospective study. J Endod. 2005;31:783-90.
24. Teixeira JMS, Barcellos MB, Pinho MAB, Barbosa CAM, Fidel RAS, Fidel SR. Effectiveness of an electronic apex locator used after preflaring of cervical and middle third. RSBO. 2012 Apr-Jun;9(2):158-62.
 Corresponding author:
Corresponding author:
Ricardo Machado
Rua Anibal Gaya, n. 898, Casa 14 – Centro
CEP 88375-000 – Navegantes – SC – Brasil
E-mail: ricardo.machado.endo@gmail.com
Received for publication: May 10, 2013
Accepted for publication: July 1, 2013
