










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.1 Joinville Jan./Mar. 2014
ORIGINAL RESEARCH ARTICLE
Analysis of blood pressure during tooth extraction
Alessandro Hyczy LisboaI; Chigueyuki JitumoriI; Evaldo Artur Hasselmann JúniorI; Rafael PesI; Gibson Luis PilattiII
I Department of Dentistry, Center of Higher Education of Campos Gerais – Ponta Grossa – PR – Brazil
II Department of Dentistry, State University of Ponta Grossa – Ponta Grossa – PR – Brazil
ABSTRACT
Introduction: Surgical procedures have a history of dental pain, apprehension and fear reported by patients. Because of these reasons, they trigger a series of modifications that lead to changes in blood pressure and stress occurrences. Objective: This study aimed to monitor changes in blood pressure pre-, trans-, and postoperatively and assess whether the differences would be significant. Material and methods: One hundred and ninety-four patients, both genders, aged between 14 and 65 who were undergoing surgery for tooth extraction were selected. They had their systolic and diastolic blood pressures measured at four different times: preoperative (M1), post-anesthesia (M2), post-extraction (M3) and at the end, after the suture (M4), with the aid of a digital tensiometer. Results: There were statistically significant differences between systolic blood pressure changes among all times, except between M1 and M4. Concerning the diastolic blood pressure measurement, there were statistical differences among all times except between M1xM4 and M2xM3. Conclusion: There were changes in blood pressure between different moments of extractions.
Keywords: blood pressure; anesthesiology; tooth extraction.
Introduction
Blood pressure (BP) is understood as that within arteries with communication to the walls. It can be calculated by multiplying the total peripheral resistance by the cardiac output and it can vary from a maximum value during systoles and a minimum value during diastoles 23. These measurements can undergo alterations because of systemic, behavioral, and physiological modifications when one faces stimuli caused by oral surgery, for example 8.
The current dental surgeries have a close relationship with blood pressure changes, since patients potentially correlate dental treatment with pain 4, resulting in fear 24, anxiety and stress, which is a body response to negative 27 and/or stress 19,22,26 stimuli many times imperceptible to the dentist. Consequently, one of the most evident effects in modifying the physiologic balance is the blood pressure change, resulting from the stress due to dental procedure 9. In Brazil, there has been found a prevalence of 15% of patients with dental anxiety 10, which can reach to 95% when tooth extraction is mentioned 11.
Heart diseases are a great risk for world population health 15 reaching from 22% to 41% of Brazilian population 2,6, and it has been an extremely prevalent condition particularly in patients who will be submitted to surgeries 25. The disease is currently explained by several genes interacting with many factors, among them, inheritance, obesity, and food 12,13. The dentists must pay attention to any symptom and they play an important role in diagnosing the disease 16. There exists also a relationship between bacterial endocarditis and oral surgery, which can results in heart alterations 30.
It is also possible to cite "white coat hypertension", a condition of blood pressure change only noted in clinical practice, where the patient is anxious and stressed waiting to be seen by either the dentist or the doctor, but it is within normal range during other daily situations 16.
Another relationship extremely important in dental clinics and mainly during oral surgeries is the use of anesthetic solutions associated with vasoconstrictor drugs because the following are the most used ones in dental practice 14: epinephrine, felypressin, phenylephrine and noradrenaline. These vasoconstrictor drugs have been associated with anesthetic salts and have directly acted on the system of blood vessels of the area anesthetized, resulting in the vasoconstriction as main effect, but exerting a side effect on blood pressure and/or heart rate 3, in addition to the pain and anxiety during anesthetic application 18.
According to Trento et al. 28 and Tucci et al. 29, these drugs inside the circulatory system can cause alterations. Adrenaline raises the systolic pressure and the heart rate, causing excitatory movements in the myocardium, palpitations and tachycardia, but these symptoms are transitory and not serious 29. On the other hand, phenylephrine and noradrenaline can significantly raise both systolic (SP) and diastolic (DP) pressure. Felypressin does not affect directly the myocardium, but it is a powerful vasoconstrictor of the heart, which can lead to angina attacks with myocardial ischemia in patients with some heart circulation deficiency 17. With the advent of vasoconstrictor drugs, it has been noted that most of the heart complications occur during or after the surgical procedure 21. Generally, these acts and symptoms cause blood pressure alterations. The dentist should control and pay special attention mainly in hypertensive and elderly patients and those with any heart alteration 1.
This study aimed to measure and analyze the result of systolic and diastolic blood pressure values at four moments of possible significant alterations during tooth extractions.
Material and methods
This study was submitted and approved by the Ethical Committee in Research of the Center of Higher Education of Campos Gerais (Cescage), under protocol no. 976/CEP. The study randomly selected 194 volunteers, both genders (91 male and 103 female), aged between 14 and 65 years-old, who were referred to tooth extraction in the Discipline of Oral Surgery of the School of Dentistry of the Center of Higher Education of Campos Gerais, Ponta Grossa, Paraná, Brazil.
All patients participating in the study were carefully evaluated by anamnesis, physical and radiographic examination, and when necessary by complementary laboratorial tests. Inclusion criteria comprised the referral for at least one tooth extraction and good general health to be submitted to the procedure. Patients who were not within the parameters to be submitted to tooth extraction; continuously using anticoagulant and/or antiplatelet drugs for the last six months; pregnant women; presenting pericoronitis, hepatic dysfunction, uncontrolled diabetes mellitus, and hypertension; and using substances capable of altering blood pressure were excluded from the study. All measurements were executed by a single examiner previously trained after the signing of a Free and Clarified Consent Form by all patients who were willing to participate in the study.
The measurements were carried out with the aid of a digital tensiometer (G-Tech Model GS100® – Genexel Medical Instruments, South Korea), previously calibrated, verified and approved by Inmetro. The systolic and diastolic blood pressure were measured (in mmHg), at four different moments: waiting room, ten minutes prior to the patient was sat on dental chair (M1), five minutes after the application of the first anesthetic tube (1.8 ml of 2% mepivacaine with epinephrine 1:100.000) (M2), after tooth extraction (M3) and after suture (M4).
After the analysis of the data, the following statistical tests were applied: Analysis of Variance for Repeated Measures Tukey-Kramer Multiple Comparisons, with level of significance of 5%.
Results
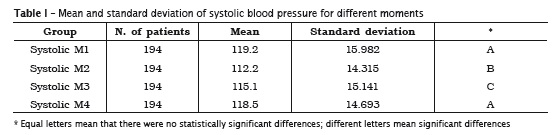
By evaluating the data of systolic measurements, the highest mean was at M1 followed by M4, M3 and M2. Comparing the systolic measurements between two different moments, only at M1xM4 there were no statistically significant differences (p > 0.05). At the other measurements, there were statistically significant differences between M1xM2 (p < 0.001), M1xM3 (p < 0.001), M2xM3 (p < 0.01), M2xM4 (p < 0.001) and M3xM4 (p < 0.001) (table I). The value of p < 0.0001 is considered as extremely significant.
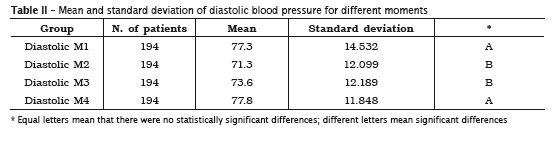
Concerning to the diastolic measurement, the highest mean was seen at M4, followed by M1, M3 and M2. Comparing these moments, at two comparisons there were no statistically significant differences: M1xM4 (p > 0.05) and M2xM3 (p > 0.05). At the other comparisons, there were statistically significant differences between M1xM2 (p < 0.001), M1xM3 (p < 0.001), M2xM4 (p < 0.001) and M3xM4 (p < 0.001) (table II).
Discussion
The knowledge of the patient's general health is of extreme importance for dentists, since systemic alterations can influence on dental treatment. Heart diseases play an important role in this context, mainly hypertension, which is the most common diseases in adults 8,15 and a growing condition in Brazil, affecting 30% of the population 2,6,10.
In this study, it could be observed that during a dental surgical procedure existed a significant alteration of blood pressure, because the peak of SP occurred at the first moment, that is, at the pre-operative time and before the anesthetic solution injection, characterizing the "white coat hypertension" 16, in addition to the anxiety generated by the effects of oral surgery can cause to patients, for example, pain, fear, and stress 4,11,19,22,24,26.
Salles et al. 20, by studying the influence of vasoconstrictor drugs on blood pressure, affirmed that there were not significant alterations after the application of 2% lidocaine with noradrenaline, 3% prilocaine with felypressin and 2% mepivacaine with epinephrine. According to Dantas et al. 7, who evaluated the effect of mepivacaine with epinephrine on blood pressure, only the diastolic pressure slightly increased about 1.5 mmHg, which is within the patterns of normal measurements: 120 for SP and 80 for DP. In this present study, the mean and standard deviation of both systolic and diastolic blood pressure measurements were within the patterns of physiologic normality. Santello et al. 21 affirmed that most of the cardiac risks for patients submitted to dental surgeries occur after the ending of the procedure. In this present study, the DP peak was just after the ending of the procedure.
Conclusion
Within the results of this study, it can be concluded:
• There were alterations in blood pressure between different moments of tooth extraction;
• The highest mean of systol ic pressure measurements was during the pre-operative moment;
• The highest mean of diastol ic pressure measurements was after the ending of the procedure;
• There were significant differences in systolic pressure measurements between M1xM2, M1xM3, M2xM3, M2xM4 and M3xM4, when compared between each other;
• There were significant differences in systolic pressure measurements between M1xM2, M1xM3, M2xM4 and M3xM4, when compared between each other.
References
1. Alencar CRB, Andrade FJP, Catão MHCV. Cirurgia oral em pacientes idosos: considerações clínicas, cirúrgicas e avaliações de riscos. RSBO. 2011 Apr-Jun;8(2):200-10. [ Links ]
2. Bronzo ALA. Procedimentos odontológicos em pacientes hipertensos com ou sem o uso de anestésico local prilocaína associada ou não ao vasoconstritor felipressina. Dissertação [Mestrado]–Faculdade de Medicina da Universidade de São Paulo, São Paulo; 2005.
3. Cáceres MTF, Ludovice ACPP, Brito FS, Darrieux FC, Neves RS, Scanavacca MI et al. Efeito de anestésicos locais com e sem vasoconstritor em pacientes com arritmias ventriculares. Arq Bras Cardiol 2008 Fev;91(3):142-7.
4. Cardoso CL, Lourei ro SR. Est resse e comportamento de colaboração em face do tratamento odontopediátrico. Psicologia em Estudo. 2008 Jan-Mar;13(1):133-41.
5. Cardoso CL, Loureiro SR, Nelson-Filho P. Pediatric dental treatment: manifestations of stress in patients, mothers and dental school students. Braz Oral Res. 2004 Mar;18(2):150-5.
6. Cavagioni LC, Pierin AMG. Hipertensão arterial em profissionais que atuam em serviços de atendimento pré-hospitalar. Texto Contexto Enferm. 2011 Jul-Sep;20(3):235-44.
7. Dantas MVM, Gabrielli MAC, Hochuli-Vieira E. Efeito da mepivacaína 2% com adrenalina 1-100.000 sobre a pressão sanguínea. Rev Odontol Unesp. 2008 Aug;37(3):223-7.
8. Ferraz EG, Carvalho CM, Jesuíno AA, Provedel L, Sarmento VA. Avaliação da variação da pressão arterial durante procedimento cirúrgico. Rev Odontol Unesp. 2007;36(3):223-9.
9. Ganhoto APA, Cabral AM, Vasquez EC, Ganhoto MRA, Lima EG. Monitorização ambulatorial da pressão arterial em indivíduos submetidos à cirurgia periodontal. Rev Bras Hipertens. 2006 Mar;13(2):97-103.
10. Kanegane K, Penha SS, Borsatti MA, Rocha RG. Ansiedade ao tratamento odontológico em atendimento de urgência. Rev Saúde Pública. 2003 Jul;37(6):786-92.
11. Lisboa AH, Kindl C, Pilatti GL. Nível de a n s i edade em p a c i e n t e s s u bme t ido s a procedimentos cirúrgicos odontológicos. Full Dent Sci. 2012;3(12):400-7.
12. Loffredo LCM, Telarolli Jr R, Basso MFM. Prevalência de hipertensão arterial sistêmica em estudantes da faculdade de Odontologia de Araraquara – Unesp. Rev Odontol Unesp. 2003 Jul-Dec;32(2):99-104.
13. Lolio CA. Epidemiologia da hipertensão arterial. Revista Saúde Pública. 1990 Apr;24(5):425-32.
14. Montan MF, Cogo K, Bergamaschi CC, Volpato MC, Andrade ED. Mortalidade relacionada ao uso de anestésicos locais em Odontologia. RGO. 2007 Apr-Jun;55(2):197-202.
15. Neves CAF, Couto GBL, Botelho KVG, Vasconcelos MMVB, Soares RPF, Cavalcanti JB et al. Avaliação da pressão arterial de crianças e adolescentes atendidos em clínica odontopediátrica. Odontologia Clín-Científ. 2007 Apr-Jun;6(2):163-7.
16. Oliveira AEM, Simone JL, Ribeiro RA. Pacientes hipertensos e a anestesia na Odontologia: devemos utilizar anestésicos locais associados ou não a vasoconstritores? HU Revista. 2010 Jan- Mar;36(1):69-75.
17. Paiva LCA, Cavalcanti AL. Anestésicos locais em Odontologia: revisão de literatura. Publ UEPG Ci Biol Saúde. 2005 Jun;11(2):35-42.
18. Possobon RF, Carrascoza KC, Moraes ABA, Costa Jr AL. O tratamento odontológico como gerador de ansiedade. Psicologia em Estudo. 2007 Sep-Dec;12(3):609-16.
19. Rocha R, Porto M, Morelli MYG, Maestá N, Waib PH, Burini RC. Efeito de estresse ambiental sobre a pressão arterial de trabalhadores. Rev Saúde Pública. 2002 May;36(5):568-75.
20. Salles CLF, Martinez AC, Pavan AJ, Daniel NA, Cuman RKN. Influência de vasoconstritores associados a anestésicos locais sobre a pressão arterial de ratos hipertensos e normotensos. Acta Scientiarum. 1999 Apr;21(2):395-401.
21. Santello JL. Atualização em hipertensão arterial: risco cirúrgico – hipertensão, fatores associados e prognósticos. J Bras Nefrol. 2001 Feb;23(1):60-3.
22. Santos FA, Santos LA, Melo DO, Alves Jr A. Estresse e estratégias de enfrentamento em pacientes que serão submetidos à cirurgia de colecistectomia. Interação em Psicologia. 2006 Jan-Jun;10(1):63-73.
23. Santos TS, Acevedo CR, Melo MCR, Dourado E. Abordagem atual sobre hipertensão arterial sistêmica no atendimento odontológico. Odontologia Clín-Científ. 2009 Apr-Jun;8(2):105-9.
24. Singh KA, Moraes ABA, Bovi Ambrosano GM. Medo, ansiedade e controle relacionados ao tratamento odontológico. Pesq Odont Bras. 2000 Apr-Jun;14(2):131-6.
25. Slullitel A. Hipertensão arterial e anestesia. RGO. 2007 Apr-Jun;55(2):197-202.
26. Tanno AP, Marcondes FK. Est resse, ciclo reprodutivo e sensibilidade cardíaca às catecolaminas. Rev Bras Ciên Farm. 2002 Jul-Sep;38(3):273-89.
27. Tomita LM, Costa Jr AL, Moraes ABA. Ansiedade materna manifestada durante o tratamento odontológico de seus filhos. Psico-USF. 2007 Jul-Dec;12(2):249-56.
28. Trento CL, Gaujac C, Santos F, Lima GDN. Complicações no uso de anestésicos locais – uma revisão. POS – Perspect Oral Sci. 2010 Aug;2(2):43-50.
29. Tucci CJ, Sposto MR, Mendes AJD. Influência da noradrenal ina cont ida nos anestésicos odontológicos sobre a pressão arterial de pacientes normotensos: estudo clínico. Rev Odontol Unesp. 1986 Mar;15(16):123-9.
30. Veronese EL, Silva FBR, Silva-Netto CR. Profilaxia e ocorrência de endocardite bacteriana por procedimentos odontológicos: uma revista da literatura. FOL – Faculdade de Odontologia de Lins / Unimep – Universidade Metodista de Piracicaba. 1999 Jan-Jun;11(2):45-51.
 Corresponding author:
Corresponding author:
Rafael Pes
Avenida Vedolino Neves, n. 400 – Centro
CEP 84530-000 – Teixeira Soares – PR – Brasil
E-mail: rafaeps2@hotmail.com
Received for publication: July 4, 2013
Accepted for publication: November 18, 2013
