










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.1 Joinville Jan./Mar. 2014
CASE REPORT ARTICLE
Unusual transmigration of canines – report of two cases in a family
Sulabha A. NarsapurI; Sameer ChoudhariII; Shrishal TotadIII
I Department of Oral Medicine and Radiology, Al-Ameen Dental College and Hospital, Rajiv Gandhi University – Bijapur-586108 – Karnataka – India
II Department of Oral and Maxillofacial Surgery, Al-Ameen Dental College and Hospital, Rajiv Gandhi University – Bijapur- 586108 – Karnataka – India
III Department of Conservative Dentistry and Endodontics, Al-Ameen Dental College and Hospital, Rajiv Gandhi University – Bijapur-586108 – Karnataka – India
ABSTRACT
Introduction: Transmigration is pre-eruptive migration of tooth across the midline. The etiology of this rare anomaly is unknown. Transmigration is largely related to mandibular canines. Although maxillary canine transmigrations are found in the literature, they are still a rare entity. Objective: The aim of the present paper is to report two cases of unusual transmigrations of canines in two immediate members of a family and to report the first case of simultaneous transmigration of maxillary and mandibular canines in an Indian adolescent. Case report: A rare case of simultaneous transmigration of maxillary and mandibular canine in Indian adolescent along with bilateral transmigration of mandibular canines in her father is described here. Conclusion: Transmigration of canines in two immediate members of family needs to be further studied for familial occurrence of transmigration.
Keywords: familial occurrence; observation; simultaneous transmigration.
Introduction
Maxillary canine impaction is a well-known dental anomaly and the incidence is in the range of 0.8%-2.8%. Mandibular canine impaction is less frequent and the incidence was reported to be 20 times lower than that for maxillary canines. Migration of a tooth across the midline is an even rarer anomaly 3. This rare phenomenon of intra osseous tooth crossing the midline is known as dental transmigration and it occurs almost exclusively with mandibular canines with an incidence of 0.1% 6,10.
Maxillary canine transmigration is still a rarer phenomenon. The exact mechanism of transmigration is not clear 4,6. This anomaly is most often asymptomatic with no pain or over pathology, and usually cannot be detected during the routine clinical examination. Hence radiographs are essential for detection of such anomalies. Panoramic radiographs plays vital role in detection of transmigrations 9. In human beings canines are very important for the facial esthetics and mast icatory funct ion and their absence may compromise both. Hence the unerupted or transmigrated canines must be diagnosed early with timely treatment plan which help to preserve these canines implicating better esthetics and functions 6.
Our search in the international literature did not reveal any reports on simultaneous transmigration of maxillary and mandibular canines in a single patient. The present paper reports first case of simultaneous transmigration of right maxillary and left mandibular canines in adolescent and bilateral transmigration of mandibular canines in her father. To our best of knowledge simultaneous transmigration of maxillary and mandibular canines and familial occurrence of transmigration has not been reported in the literature yet.
Case report
A 13 old young Indian female was referred to the department of oral medicine and radiology for oral prophylaxis. No extra oral abnormality was detected. Intraoral examination revealed clinical absence of right permanent maxillary canine, left maxillary canine and left mandibular canine.
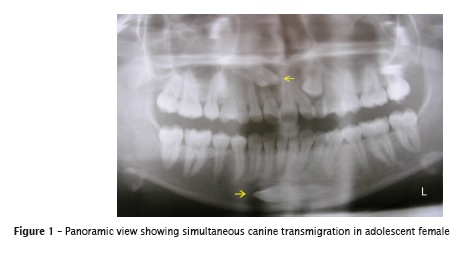
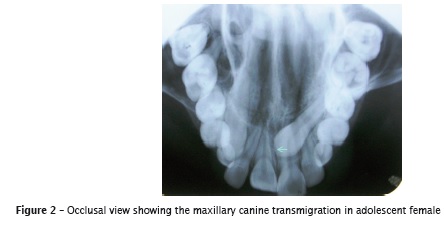
Panoramic view revealed retention of right, left maxillary and left mandibular primary canines along with the impaction of permanent maxillary right canine, maxillary left canine and mandibular left canine (figure 1). The right maxillary canine had transmigrated with its crown just crossing the midline (figure 2). The left mandibular canine was transmigrated and horizontally impacted near inferior border of mandible with its crown positioned below the root apices of right canine. The crowns of t ransmigrated canines were surrounded by enlarged follicular space. All the third molars were missing. Left first premolar was rotated by 90º. With these findings a diagnosis of simultaneous transmigration of maxillary and mandibular canine was made. Patient was informed of the condition and possible treatment plans. Since patient was not interested in any type of treatment, no treatment was given except from oral prophylaxis. Patient was informed about the consequences and radiographic monitoring was strongly recommended.
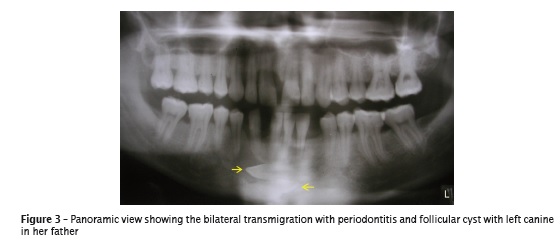
Examination of her immediate family members revealed that her father had missing lower canines bilaterally. Right lower lateral incisor was slightly extruded form its socket with slight mobility. Intra oral or extra oral swelling or tenderness was not noted in region of missing canines. Panoramic radiograph was taken which revealed bilateral transmigration of lower canines. There was irregular radiolucency around the left canine which was placed below the right lateral incisor and first premolar extending superiorly to the distal side of right lateral incisor (figure 3). Horizontal bone loss was seen till almost middle one third with lower anterior teeth with vertical bone defect along the distal aspect of the right lateral incisor and upper central incisor. With these findings a diagnosis of bilateral transmigration of mandibular canines with follicular cyst in association with left canine was made. Patient was informed about the consequences. Patient was not interested in any treatment type. None of other family members were affected. Unfortunately both the patients never returned for their follow up appointments and were lost to recall.
Discussion
Although migration of teeth is well documented, ectopia, pre-eruptive migration of tooth across the midline of jaw is termed as transmigration. The term transmigration was first used by Ando et al. in 1964 7. Tarsitano et al. defined transmigration as the phenomenon of an unerupted mandibular canine through midline. Joshi and Acluck suggested that the tendency of a canine to cross the midline suture is a more important consideration than the actual distance of migration after crossing the midline 4.
The etiology and exact mechanism are still not clear. Number of factors has been suggested. Abnormal displacement of the dental lamina in the embryonic life 6, abnormally strong eruptive force, conical shape of the canine which drives canine through dense symphysis, 4 agenesis of the adjacent teeth in particular the lateral incisor 11, presence of cyst around the crown of the canine facilitating the migration process 1, premature loss of deciduous teeth, retention of deciduous teeth, inadequate space, crowding, excessively large crowns, odontoma, fractures, cysts tumors, unfavorable alveolar length, genetics, and root stump obstacle would be sufficient to divert a tooth from its original path of eruption 4,5,8. In these present cases the primary canines were retained in young female patient, and in her father, follicular cyst was noted together with the left canine in order that the occurrence of transmigration in two immediate family members needs to be further studied for familial occurrence of transmigration.
Most of reports in the literature have described single cases 10. Transmigration of unerupted tooth is generally a unilateral phenomenon, although bilateral transmigrations have been reported 10. Transmigration is rarely found in maxillary arch. Aydin and Yilmaz reported the first case of maxillary canine transmigration in the literature in 2003 2. Kumar et al. reported maxillary canine transmigration of maxillary canine along with upper lateral incisor 6. Till date only 31 cases of maxillary canine have been reported in the literature with only two cases in Indian population 6 before this; however, simultaneous mandibular and maxillary canine transmigration has not been reported in the literature. Bilateral transmigration of mandibular canines along with periodontitis is also not reported.
The large cross-sectional area of the anterior mandible compared with the anterior maxilla may be the reason for higher frequency of mandibular transmigration. The maxilla transmigration of canines may be prevented by a shorter distance between the roots of the maxillary incisors and the floor of the nasal fossa as well as by the restriction of path of tooth movement by the roots of adjacent teeth, the maxillary sinus and midpalatal suture which act as a barrier 6.
Mupparapu described the five patterns for transmigrated mandibular canine 6,7. Type 1 – Canine is impacted mesioangularly across the midline, labial or lingual to the anterior teeth with crown portion of tooth crossing the midline. Type 2 – Canine is horizontally impacted near the inferior border of the mandible below the apices of the incisors. Type 3 – Canine has erupted either mesial or distal to opposite canine. Type 4 – Canine is horizontally impacted near the inferior border of the mandible below the apices of the premolar or molar on the opposite side. Type 5 – Canine is positioned vertically in the middle with long axis of the tooth crossing the midline. In the child patient, the mandibular canine transmigration was type 2 and transmigrated maxi llary canine in the child and bi lateral transmigration in her father could not be classified as there was no classification system proposed until now in the literature.
There have been several treatment options proposed for this anomaly 4. Surgical extraction appears to be the most favored, rather than heroic effort to bring the tooth back to its position. It is also indicated in the existence of pressure resorption towards the roots of adjacent teeth, periodontal problems, infections, cysts, prosthetic problems, neuralgic symptoms etc. Contralateral nerve should be anesthetized for extraction of transmigrated tooth as they maintain their nerve supply from original side.
If the mandibular incisors are in normal position and space for the transmigrated canine is sufficient, transplantation may be undertaken.
Orthodontic treatment can be done to bring back the labially impacted transmigrated canine to position. However, if the crown of such tooth migrates past the opposite incisor area or if the apex is seen to have migrated past the apex of adjacent lateral incisor it is impossible to bring back it into original place.
Some authors believe that symptom less non erupted teeth can be left in place.
In the present cases as both of our patients were not interested in any treatment, we opted to follow up the cases, but unfortunately the patients never came back for their appointments.
Conclusion
Transmigration is a rare event and simultaneous transmigration of maxillary and mandibular canines in a single patient is still rarer entity. Transmigration in two immediate members of family needs to be further studied for familial occurrence. Early radiographic examination of patient is important for treatment planning. Future studies and reports of more cases of canine transmigration would help to better understand their etiology, mechanism of migrat ion and improvement of classification criteria.
References
1. Al-Waheidi EM. Transmigration of unerupted mandibular canine with a literature review and a report of five cases. Quintessence Int. 1996 Jan;27(1):27-31. [ Links ]
2. Aydin U, Yilmaz HH. Transmigration of impacted canines. Dentomaxillofac Radiol. 2003 May;32(3):198-200.
3. Aydin U, Yilmaz HH, Yildirim D. Incidence of canine impaction and transmigration in patient population. Dentomaxillofac Radiol. 2004 May;33(3):164-9.
4. Camilleri S, Scerri E. Transmigration of mandibular canines – a review of the literature and report of five cases. Angle Orthod. 2003 Dec;73(6):753-62.
5. Joshi MR. Transmigrant mandibular canine: a record of 28 cases and retrospective review of the literature. Angle Orthod. 2001 Feb;71(1):12-22.
6. Kumar S, Urala AS, Kamath AT, Jayaswal P, Valiathan A. Unusual intraosseous transmigration of impacted tooth. Imaging Sci Dent. 2012 Mar;42(1):47-54.
7. Mupparapu M. Patterns of intraosseous t r ansmi g r a t ion and e c topi c mandibul a r canine: review of literature and report of nine additional cases. Dentomaxillofac Radiol. 2002 Nov;31(6):335-60.
8. Peck S. On the phenomenon of intraosseous migration of nonerupting teeth. Am J Orthod Dentofacial Orthop. 1998 May;113(5):515-7.
9. Shapira Y, Kuftinec M. Unusual intraosseous transmigration of a palatally impacted canine. Am J Or thod Dentofac ial Or thop. 2005 Mar;127(3):360-3.
10. Sumer A, Sumer M, Ozden B, Otan F. Transmigration of mandibular canines: a report of six cases and a review of the literature. J Contemp Dent Prat. 2007 Mar;8(3):104-10.
11. Vichi M, Franchi L. The transmigration of the permanent lower canine. Minerva Stomatol. 1991 Sep;40(9):579-89.
 Corresponding author:
Corresponding author:
Sulabha A. Narsapur
Department of Oral Medicine and Radiology, Al-Ameen Dental College and Hospital, Athani Road
Bijapur-586108 – Karnataka – India
E-mail: drsrident@gmail.com
Received for publication: August 12, 2013
Accepted for publication: October 14, 2013
