










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.1 Joinville Jan./Mar. 2014
CASE REPORT ARTICLE
Maxillary squamous cell carcinoma: diagnosis and evolution of an inoperable case
Luana Beber YoshizumiI; Mariah Scotti AléricoI; José Miguel Amenábar CéspedesII; Cleto Mariosvaldo PiazzettaII; Cassius Carvalho Torres-PereiraII
I Department of Dentistry, Federal University of Paraná – Curitiba – PR – Brazil
II Department of Stomatology, Federal University of Paraná – Curitiba – PR – Brazil
ABSTRACT
Introduction: Squamous cell carcinoma (SCC) is a malignant neoplasia, originating from the oral lining epithelium, responsible for approximately 90-95% of malignancies in this location. Incidence and mortality rates for oral SCC may vary due to personal habits, socioeconomic characteristics, environmental factors and quality of health care. This study reports the aggressive evolution of SCC with a delayed diagnosis and the impossibility of immediate curative therapy. Case report: A 47-year-old brown male patient, smoker and drinker was referred by a primary health care center to the Stomatology Clinic at UFPR (Federal University of Paraná). The diagnosis of well-differentiated SCC was confirmed by histopathological examination. The patient was referred to a specialized service where an oncology team defined the case as inoperable due to lung function limitations and advanced tumor staging. The patient underwent lung physiotherapy sessions until reaching clinical conditions to undergo oncologic therapy which included radiotherapy and chemotherapy. Conclusion: The reported case highlights the importance of establishing an early diagnosis for SCC. There is a need of facilitating and speeding the access to both health care services and information that lead patients to seek professional assistance as soon as the first disease signs appear.
Keywords: mouth neoplasms; diagnosis; squamous cell carcinoma.
Introduction
Squamous cell carcinoma (SCC), sometimes referred to "spinocellular carcinoma" or "epidermoid carcinoma", accounts for 90% of the malign neoplasias occurring in the oral mucosa 2,6,7,9,15. It more frequently affects male individuals between the fourth and sixth decade of life, more commonly occurring at the tongue and mouth floor 2,7,12,15. Its etiology is multifactorial comprising environmental, social, and behavioral factors with smoking and drinking habits accounting for its main etiological agents 6,7,9,12,15.
The initial clinical aspect can vary among either leukoplakic, erythroplastic or leukoerythroplastic aspect. Its growth can be either exophytic or endophytic, leading to an aspect with stiffened base and areas of necrosis. In most advanced cases, in which the underlying bone was affected, the radiographic examination can show radiolucent areas without defined limits. The definitive diagnosis is obtained through histopathological examination which also determines the type and stage of the lesion 6,7.
Early diagnosis is fundamental to choose the treatment management, its onset, and consequently the prognosis and the patient's survival 2,13,15. The treatment choice – surgery, chemotherapy and/or radiotherapy – depends on the clinical staging and the degree of histopathological differentiation of the tumor 6. The best index of SCC prognosis is the moment of its diagnosis so that the advanced staging has been frequently associated with high mortality rates 13. The survival rate of patients with head and neck malign neoplasia is of 76% in early diagnosis cases, 41% in cases of metastasis in cervical lymph nodes and 9% in cases of metastasis in the neck area 2. Notwithstanding, the advancements in therapy and care patterns seem to play an important role in the moderate increasing of the survival rate 13.
Although early diagnosis can be performed by either the dentist during routine appointments or the patient through self-examination, most cases are late diagnosed 5,9,11,13,15.
The aim of this present study is two-fold: to report a clinical case of malign neoplasia affecting the maxilla, aggressive and inoperable, in a patient with prolonged history of exposition to the main risk factors; to discuss the treatment managements and its consequences in late diagnosing and advanced staging of the disease, considering the comorbidities identified in the comprehensive health state of the patient.
Case report
A 47-year-old male patient was referred to the Discipline of the Stomatology of the Federal University of Paraná by a primary care center with main complaint of a "swelling in the face". According to the patient, the swelling had appeared after the removal of a maxillary tooth. During anamnesis, the patient reported he consumed alcoholic beverage daily and smoked three packages per day since his 18 years old. He also reported to not practicing exercises and not having any systemic alterations.
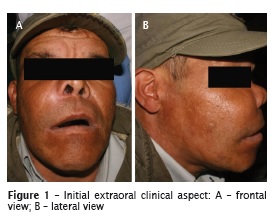
At extraoral clinical examination, it was observed a significant volume increasing at the right zygomatic area with signs of inflammation (figure 1A and B). At intraoral clinical examination, an irregular nodular mass was seen measuring 3 cm in its higher diameter, localized at the maxillary right side on the alveolar ridge, vestibule bottom and palate with a color among pinkish, reddish and whitish, firm to palpation and asymptomatic. The oral hygiene was poor with advanced periodontal destruction (figure 2). Panoramic, lateral, profile and posterior-anterior radiographs were obtained and revealed an extensive radiolucent area with vaguely defined limits located in the area of teeth #13 to #16 closer to the lesion (figure 3).


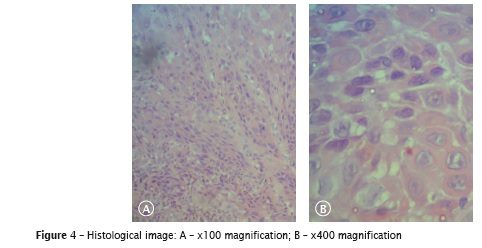
The diagnosis hypothesis was suggested as malign neoplasia of conjunctive tissue. At the same appointment, an incisional biopsy was carried out whose histopathological examination described welldifferentiated, invasive and ulcerated squamous cell carcinoma (figure 4A and B).
The patient was referred to the Oncology Service of the Erasto Gaertner Hospital, in the city of Curitiba, Paraná, Brazil. The hospital team considered the lesion as inoperable because of its dimensions, therefore opting by radiotherapy treatment as the first choice.
During stomatology revaluation, after three weeks, it was observed the increasing of the lesion (figure 5A and B), with poor oral hygiene, right nose suppuration, without painful symptomatology (figure 6). It was prescribed Amoxicillin 500 mg and 0.12% Chlorhexidine Digluconate to prevent secondary infection. The patient returned 6 weeks later showing visible weight loss increasing of the swelling worst oral hygiene with foul odor, displacement of the teeth near to the lesion, nasal suppuration and pain (figure 7). Notwithstanding, the surgery was still impossible. The aforementioned prescription was maintained until the surgery would be possible.



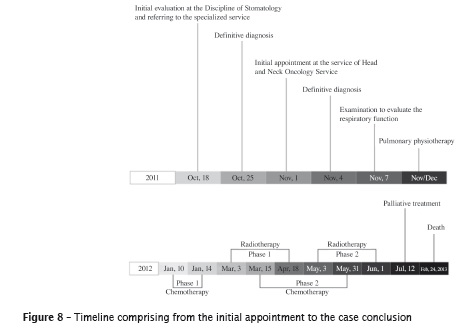
The patient was diagnosed with limited respiratory function and underwent 40 sessions of pulmonary physiotherapy. Only after that, the oncological treatment could be started.
At first, this comprised chemotherapy for four appointments, which had to be ended because the comprehensive health of the patient had worsened. Then, radiotherapy was chosen.
The radiotherapy appointments (n = 35) were daily executed together with chemotherapy (figure 8).
Parenteral nutrition was introduced during radiotherapy, once the patient had difficulty in chewing and swallowing.
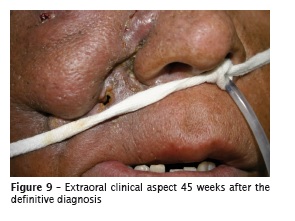
Palliative treatment was continued for pain, swelling and infect ion controlling (codeine, dexamethasone, benzoi lmet ronidazole and omeprazol). Also, the physiotherapy exercises were maintained to preserve the muscle and lung condition. After 45 weeks since the definitive diagnosing at the Erasto Gaertner Hospital, the tumor mass reduced at the right zygomatic area but the patient still exhibited nasal suppuration with skin fenestrations which had been treated with metronidazole ointment and cleaning with saline solution (figure 9). At intraoral examination, there was advancement of the maxillary involvement including the left side, with degree 3 mobility in the teeth #24 and #25. The area directly affected by radiotherapy presented extensive areas of tissue necrosis. The patient still showed poor hygiene with dental calculus, and hairy tongue (figure 10). The prescription of 0.12% chlorhexidine digluconate was maintained during all the stages of the treatment.

In February, 24, 2013 the patient passed away because of neoplastic cachexia.
Discussion
Similarly to other malign neoplasias, the earlier the diagnosis of squamous cell carcinoma, the better it prognosis 7,8. Notwithstanding, in this case report, the patient only sought for help when the disease was at an advanced stage. Such fact has been frequently described in the literature 2,7,9,12, and late diagnosis will result in more aggressive, expensive and disfiguring treatment, with poor quality of life and shorter survival rate 3,7.
The lack of attention of both the patient and the dentist accounts for the delay in obtaining the diagnosis 11. Because of the lack of symptomatology at the initial stages of the disease, the patients failed in seeking for treatment 9,11. The most frequent first symptoms are not shocking and can be easily attributed to simple causes by patients with little information 3. In this case report, the patient sought for treatment only when he had difficulty in swallowing and because of the pressure of his relatives due to his halitosis. Tucci et al. 15 still added as causes in treatment delay the fear of receiving the diagnosis even noting alterations in the mucosa. It has been also emphasized the situations in which the patients only seek for treatment because there is a deformity caused by the tumor growth 15.
The social-economical level, difficulties of access to health care, and lack of information may play a role in treatment delay 10. In this case report, the diagnosis delay is compatible with such situation because the patient had low education level and lived far from the primary health care center. Santos et al. 11 pointed out that this situation is the result of the lack of public policies aiming to the prevention and information regarding to oral cancer. According to Torres-Pereira et al. 14, oral cancer problem would be better managed if the health managers assumed it as a responsibility of each Brazilian city.
In this case report, the diagnosis delay occurred preponderantly because of the postponement in seeking for primary care and just after that because the patient failed in immediately attending to the referral for secondary attention, which took about two weeks.
Other relevant factor was the delay in the beginning of the oncologic treatment. Most of the specialized health services are located in the capitals of the Brazilian states, which implies in difficulty of access of patients living in the country and even metropolitan regions. According to the literature review of Santos et al. 11, many authors already reported that the time from the perception of symptoms and diagnosis until the treatment interferes in the evolution and prognosis of the disease and also in the quality of life of the patients. This present case report strengthens this perception suggested in some studies on the positive relationship between the difficulty of access and failure in the early cancer diagnosis. Still considering the delay in oncological treatment, the referral to public health care may be an aggravating factor, since many times the referral time is long and bureaucratic, interfering in the treatment and consequently in the prognosis and survival of the patient 1.
In this case reported, the need of pulmonary physiotherapy was an additional factor for the delay in oncological treatment onset. Moreover, all the comorbidities resulting from the long exposition to tobacco and alcohol caused important loss of the pulmonary capacity and physical fragility, consequently a preparation phase was required until the patient exhibited minimum conditions to treat oral malign neoplasia. Because of the tumor dimensions, the oncological team considered it as inoperable. According to Brener et al. 4, surgical treatment is the first choice in the treatment of oral malign neoplasia, varying with the size and staging of the disease. Radiotherapy has been chosen if there are no clinical conditions to submit the patient to surgery or if the patient does not accept the sequelae left by the treatment 4. The treatment timeline of this case report illustrates very well the difficulties faced during the decision making process of the treatment. The aesthetic and functional impact of an eventual surgical resection together with the physical fragility caused by the disease itself and the comorbidities hindered the adoption of a curative approach. At all stages, the disease management aimed to decrease the neoplasia volume and keep the patient in a condition of living together with his relatives.
Concerning to the prognosis, Seoane-Romero et al. 13 affirmed that variables such as age, comorbidities, immunological or nutrition state, tumor size and location, expression of oncogenes, proliferation markers, and DNA content have been evaluated as independent prognostic markers for oral cancer. However, the diagnosis stage is the most important marker for oral and oropharynx squamous cell carcinoma prognosis so that advanced stages have been frequently associated with high mortality rates. The case here reported corroborates the situation described by other authors 13.
Conclusion
This case reported highlights the importance of establishing an early SCC diagnosis. Therefore, an easier access to health services and more information on oral cancer prevention are required so that patients would seek for treatment at the first signs of the disease. Moreover, both the dentists and the health managers play an important role in decreasing the diagnosis delay by improving the referral system among the health-attention levels in Brazilian health services.
References
1. Abdo EM, Garrocho AA, Barbosa AA, Oliveira EL, Filho LF, Negri SLC et al. Time elapsed between the first symptoms, diagnosis and treatment of oral cancer patients in Belo Horizonte, Brazil. Med Oral Patol Oral Cir Bucal. 2007 Nov 1;12(7):469-73. [ Links ]
2. Akbulut N, Oztas B, Kursun S, Evirgen S. Delayed diagnosis of oral squamous cell carcinoma: a case series. J Med Case Rep. 2011 Jul;6(5):291.
3. Baykul T, Yilmaz HH, Aydin U, Aydin MA, Aksoy M, Yildirim D. Early diagnosis of oral cancer. J Int Med Res. 2010 Jun;38:737-49.
4. Brener S, Jeunon FA, Barbosa AA, Grandinetti HAM. Carcinoma de células escamosas bucal: uma revisão de literatura entre o perfil do paciente, estadiamento clínico e tratamento proposto. Rev Bras Cancerol. 2007;53(1):63-9.
5. Costa EGC, Migliorati CA. Câncer bucal: avaliação do tempo decorrente entre a detecção da lesão e o início do tratamento. Rev Bras Cancerol. 2001;47(3):283-9.
6. Daniel FI, Granato R, Grando LJ, Fabro SML. Carcinoma de células escamosas em rebordo alveolar inferior: diagnóstico e tratamento odontológico de suporte. J Bras Patol Med Lab. 2006 Aug;42(4):279-83.
7. Gaetti-Jardim EC, Pereira CCS, Guastaldi FPS, Shinohara EH, Garcia Jr IR, Gaetti-Jardim Jr E. Carcinoma de células escamosas de grandes dimensões. Rev Odont Araçatuba. 2010 Jul- Dec;31(2):9-13.
8. Gao W, Guo CB. Factors related to delay in diagnosis of oral squamous cell carcinoma. J Oral Maxillofac Surg. 2009 May;67(5):1015-20.
9. Gervásio OLAS, Dutra RA, Tartaglia SMA, Vasconcellos WA, Barbosa AA, Aguiar MCF. Oral squamous cell carcinoma: a retrospective study of 740 cases in a Brazilian population. Braz Dent J. 2001;12(1):57-61.
10. Gómez I, Seoane J, Varela-Centelles P, Diz P, Takkouche B. Is diagnostic delay related to advanced-stage oral cancer? A meta-analysis. Eur J Oral Sci. 2009 Oct;117(5):541-6.
11. Santos LCO, Batista OM, Cangussu MCT. Caracterização do diagnóstico tardio do câncer de boca no estado de Alagoas. Braz J Otorhinolaryngol. 2010;76(4):416-22.
12. Sassi LM, Oliveira BV, Pedruzzi PAG, Ramo GHA, Stramandinoli RT, Gugelmin G et al. Carcinoma espinocelular de boca em paciente jovem: relato de caso e avaliação dos fatores de risco. Rev Sul-Bras Odontol. 2010 Mar;7(1):105-9.
13. Seoane-Romero JM, Vázquez-Mahía I, Seoane J, Varela-Centelles P, Tomás I, López-Cedrún JL. Factors related to late stage diagnosis of oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal. 2012 Jan 1;17(1):35-40.
14. Torres-Pereira CC, Angelim-Dias A, Melo NC, Lemos Jr. CA, Oliveira EMF. Abordagem do câncer da boca: uma estratégia para os níveis primário e secundário de atenção em saúde. Cad Saúde Pública [online]. 2012 Mar;28:s30-s9 [cited 2012]. Avaiable from: URL:http://www.scielo.br/scielo. php?script=sci_arttext&pid=S0102-311X20120 01300005&lng=en&nrm=iso>.
15. Tucci R, Borges FT, Castro PHS, Aburad A, Carvalhosa AA. Avaliação de 14 casos de carcinoma epidermoide de boca com diagnóstico tardio. RSBO. 2010 Jun;7(2):231-8.
 Corresponding author:
Corresponding author:
Luana Beber Yoshizumi
Rua José Rietmeyer, n. 471, bloco 1, apto. 204 – Guabirotuba
CEP 81510-630 – Curitiba – PR – Brasil
E-mail: luana.yoshizumi@gmail.com
Received for publication: May 30, 2013
Accepted for publication: September 30, 2013
