










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.2 Joinville Abr./Jun. 2014
ORIGINAL RESEARCH ARTICLE
Students' perceptions on diagnosis and treatment of occlusal surface of first molars
Beatriz Vieira de Paiva I; Fernanda Ladico Miura I; Silvana de Andrade Silvestre de Lima I; Danielly Cunha Araújo Ferreira II; Alessandra Maia de Castro III; Fabiana Sodré de Oliveira III
I School of Dentistry, Federal University of Uberlândia – Uberlândia – MG – Brazil
II School of Dentistry of Ribeirão Preto, University of São Paulo – Ribeirão Preto – SP – Brazil
III School of Dentistry, Federal University of Uberlândia – Uberlândia – MG – Brazil
ABSTRACT
Introduction: Accurate diagnosis of dental caries is a fundamental requirement in health care. Objective: The aim of this study was to evaluate the opinions of undergraduates concerning different conditions of the occlusal surface of permanent first molar. Material and methods: Two experienced and trained examiners, using visual and radiographic examinations, classified five occlusal surfaces of permanent first molars. The surfaces were photographed and presented to students with a questionnaire about classification of occlusal surfaces, methods used to aid caries diagnosis and type of treatment to be applied. The answers were classified as correct and incorrect and submitted to Chi-square test (p < 0.05). Results: The results showed a higher percentage of correct answers regarding to dentine caries (87.95%) and no caries (84.34%). For all surface conditions, the methods most commonly used to aid diagnose were professional prophylaxis, good lighting, drying and dental probe. Considering the treatment, a greater number of correct answers were obtained for the surface with dentine caries, with indication of conventional (65.06%) and/or preventive restoration (33.73%) and no caries without treatment need or sealant (53.01%). For students at 6th, 7th and 8th semesters, the percentage of correct answers for classification and treatment was 72.31%, 58.33% and 62.94%, respectively, without statistically significant differences (p < 0.05). Conclusion: It was concluded that the opinion of students differed regarding to the diagnosis and treatment mainly when the occlusal surface showed early stages of dental caries.
Keywords: dental caries; preventive dentistry; dental education.
Introduction
Despite the fact that the prevalence of dental caries has declined considerably, the reduction has not occurred uniformly for all dental surfaces. Occlusal surfaces are still the most likely sites for the development of lesions and occlusal caries account for most of the lesions in children aged 8-15 years 1,8.
The diagnosis of occlusal caries has always been difficult 3,5,6,19. Every practitioner is aware of the problems inherent in determining the presence or absence of an early lesion in these sites, which because of their morphology cannot be directly visualized 6.
There are many different methods for detecting occlusal caries 4. The ideal caries detection method should capture the whole continuum of the caries process, from the earliest to the cavitation stage 25.
The dental professional's approach to the treatment of caries has been evolving in recent years. Changes in caries epidemiology, advances in materials and technology have all contributed to the emergence of a more proactive, tailored, preventive and conservative treatment philosophy characterized by greater attention to the individual and his or her disease 2.
Due to the high susceptibility to caries of occlusal surfaces and the difficulties of diagnosis, many studies were conducted to evaluate different diagnostic methods 1,10,13,16,22,23 diagnosis variability and treatment decision for this surface 3,5,9,17,18.
Some studies were conducted among students 18, between students and teachers 5,23, between students and dentists 3, and among dental professionals 13,17. A wide variability in the diagnosis of occlusal caries and treatment decision for this surface has been found 5,17,18. Knowledge and experience of examiners influence on their ability to detect caries and affect inter-examiner reproducibility 23.
Accurate diagnosis of either the absence or presence of the disease is a fundamental requirement in health care 14 and the accurate diagnosis of the presence of disease is paramount for appropriate care 10. The diagnosis of non-overt occlusal decay is challenging and can be highly subjective, and its inherent uncertainties can lead to widely differing treatment decisions 14. Thus, the aim of this study was to evaluate the behavior of undergraduates regarding to different conditions of the occlusal surface of the permanent first molars. The specific aims included: (1) to investigate the ability of dental undergraduates to classify an occlusal surface and define a logical management for each clinical condition and (2) to identify the methods that students would use to aid the diagnosis of these surfaces.
Material and methods
Ethical aspects
This study was approved by the Ethics Committee (protocol no. 050/07) of the Federal University of Uberlândia, Minas Gerais, Brazil.
Sample selection
A convenience sample of undergraduates was chosen on the basis of availability for comparative study from the 6th, 7th and 8th semesters at the School of Dentistry of the Federal University of Uberlândia. The students were informed on the objectives of the study and signed the informed consent form. Eighty-three students participated in the study, 13 (15.66%), 36 (43.38%) and 34 (40.96%) enrolled at 6th, 7th and 8th semesters, respectively.
Study design
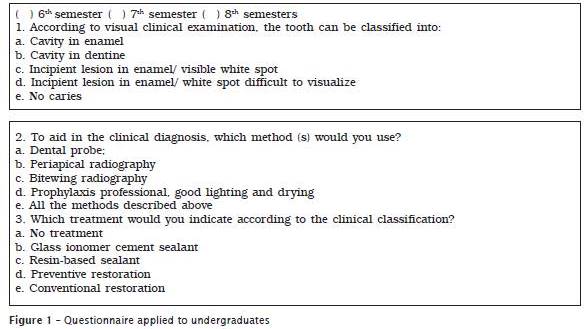
Five occlusal surfaces of permanent first molars of five patients underwent treatment at in the Clinic of Pediatric Dentistry were selected by two experienced and trained examiners using visual and radiographic examinations. The clinical examination was performed according to the visual examination criteria established by Ekstrand et al. 7 (Table I). Visual examination was carried out using only a dental operating light and air-drying for 5 seconds. No dental explorer was used during the examination. Prior to the visual clinical examinations, the occlusal surface was cleaned with bicarbonate jet and water (Profident – Dabi-Atlante). Each occlusal surface was scored as presented in Table I. The tooth selection included scores 0–4. This examination was performed by each examiner separately and final scores were obtained by discussion and consensus. The occlusal surfaces of the teeth were photographed and printed in order to produce examination sheets generating 10cm x 15cm images. These photographs were randomly numbered from 0 to 5. Photography 1 = Cavity in enamel, Photography 2 = Cavity in dentine, Photography 3 = Visible white spot, Photography 4 = White spot difficult to visualize, Photography 5 = No caries.
The teeth were radiographed under standardized conditions. The same two experienced and trained examiners analyzed the bitewing radiographs using the criteria established by Ekstrand et al. 9 (Table I). This examination was carried out by each examiner separately and final scores were obtained by discussion and consensus. Based on visual and radiographic examinations a logical management was established for each occlusal surface varying from no treatment to sealant, preventive restoration and conventional restoration.
The students were required to analyze the five photographs and to answer the questionnaire containing three questions about classification, methods used for aiding caries diagnosis and management for each one of the occlusal surfaces. The questionnaire was applied by two previously trained interviewers (Figure 1).
The students' answers were compared with the condition, the methods of diagnostic and proposed management given for each occlusal surface by two experienced and trained examiners and classified as correct and incorrect based on the literature.
Statistical analysis
Descriptive statistics were used to analyze the quantitative data. The percentages of correct answers among the students at 6th, 7th and 8th semesters were compared using chi-square test (p < 0.05).

Results
Table II presents the frequency and percentage distribution of answers from the students at each semester for the condition classification of the occlusal surface per each photograph.
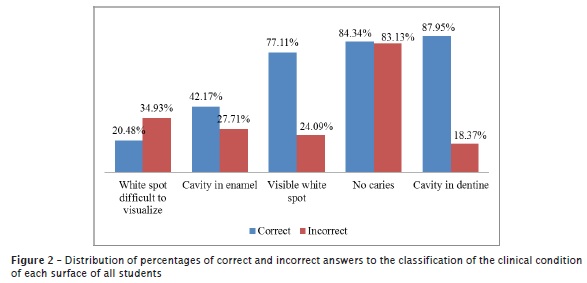
Concerning to photograph #1, in which caries in enamel was presented, the results showed that the percentage of correct answers for students at 6th, 7th and 8th semesters was respectively 38.46%, 36.11% and 50.00%.Within the sum of the responses of all students, the total number of correct responses was 42.7% (Table II and Figure 2).
The results from the occlusal surface having cavity in dentine (photograph #2) showed that the percentage of correct answers for students at 6th, 7th and 8th semesters was respectively 100.00%, 88.89% and 82.35%. Within the sum of the responses of all students, the total number of correct answers was 87.95% (Table II and Figure 2).
With regard to photograph #3, in which the occlusal surface had a visible white spot, the results showed that the percentage of correct answers for students at 6th, 7th and 8th semesters was respectively 84.62%, 72.22% and 79.41%. Within the sum of the responses of all students, the total number of correct answers was 77.11% (Table II and Figure 2).
The results of photograph #4 (occlusal surface with a white spot difficult to visualize) showed a percentage of correct answers for students at 6th, 7th and 8th semesters was respectively 38.46%, 11.11% and 23.53%. Within the sum of the responses of all students, the total number of correct answers was 20.48% (Table II and Figure 2).
The percentage of correct answers for students at 6th, 7th and 8th semesters was respectively 100.00%, 83.33% and 79.41% for photograph #5 (occlusal surface without caries). Within the sum of the responses of all students, the total number of correct answers was 87.95% (Table II and Figure 2).
Figure 2 displays the total number of correct and incorrect answers with respect to the condition classification of the occlusal surface considering the responses of all students.
Table III presents the distribution of frequencies and percentages of students' responses at each semester comprising the methods used to aid in the diagnosis of the occlusal surface condition for each photograph.
For all clinical photographs, the most cited response was professional prophylaxis, followed by good lighting and drying, except for photograph #2 (dentine caries) with a lower percentage (65.06%). With regard this latter photograph, the method of choice was the use of dental probing and periapical radiograph (59.04%), On the other hand, bitewing radiographs was chosen for all conditions of the occlusal surface at a lower frequency ranging from 2.41% to 25.30%. The combination of methods for diagnosis of the surfaces was indicated in a lower frequency ranging from 1.20% to 7.23% (Table III).
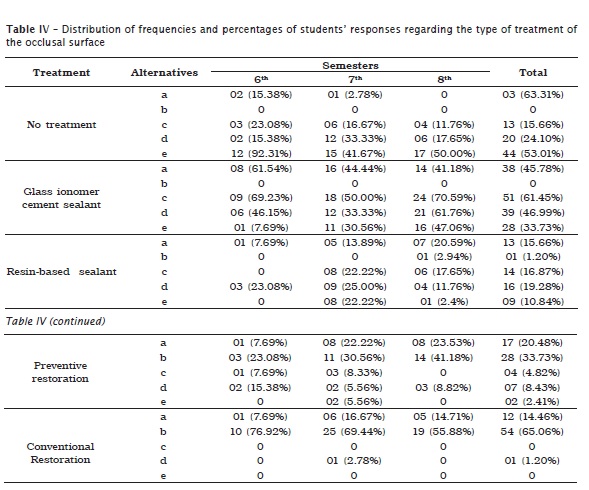
With regard to the treatment indication, 53.01% and 63.61% of the students answered that they do not treat both occlusal surface without caries and cavities in enamel, respectively. The glass ionomer cement sealant was indicated for all surfaces, except for those with dentine caries, but greater than the indication for the surface with visible white spot. Resin-based sealant was chosen for all occlusal surfaces, including those with dentine caries, but at a smaller proportion. The preventive restoration was indicated for all occlusal surfaces and conventional restoration surfaces for white spot difficult to visualize, cavity in enamel and dentine caries at a higher frequency (Table IV).
Table V shows the distribution of frequencies and percentages of students who answered correctly the classification and treatment of occlusal surface. All students who correctly classified the condition indicated the occlusal surface treatment correctly. Concerning to the students at 6th, 7th and 8th semesters, the percentage of correct answers for classification and treatment was 72.31%, 58.33% and 62.94%, respectively (Table V). Chi-square test (p < 0.05%) was applied and no statistically significant difference was found.
Figure 3 displays the distribution of the percentages of correct and incorrect answers of the students at each semester considering all the questions. According to the results, it was observed that students at 7th and 8th semesters showed a higher number of correct answers than those from the 6th semester. Chi-square test was applied (p < 0.05%) and no statistically significant increasing of correct answers among the percentages obtained by students at the three semesters was seen.




Discussion
Diagnosis is a fundamental step for making treatment decisions 4. As far as carious lesions are concerned, diagnosis implies deciding whether demineralization is present, the depth of the lesion and whether it is progressing rapidly or slowly or whether it is already arrested. Thus, diagnosis is more than lesion detection: it should also consider lesion activity 8,20.
In clinical practice, students are faced with many clinical situations in which they must diagnosis and decide which treatment is most appropriate. The occlusal surface of the first permanent molar is the site of greatest risk for the development of dental caries. This study was an attempt to investigate the ability of undergraduate students to classify occlusal surface and define a logical management for each clinical condition and to identify the methods that students have used to aid the diagnosis of these surfaces.
Most studies have been performed on extracted molars 1,3,16,18,22,23 or indicated for extraction 9 to be later evaluated by macroscopic and microscopic examination. This study used a questionnaire and clinical photographs in order to simulate a similar clinical situation methodology to that used by other authors 5,10.
Although the questionnaire did not contain data on the caries risk to the patient, the chosen photographs that had white spot lesions were classified as active 8.
The results agree with other authors who observed a wide variation in the diagnosis of the occlusal surface 5,17,18. In this study, there were a higher percentage of correct responses when the surface showed no cavity and caries in dentine. The intermediate stages in which the surface presented with white spots difficult to visualize and the presence of cavity in enamel, the amount of correct answers were lower and highly variable (Table III; Figure 2).
Although there are different methods for the evaluation of occlusal caries in clinical routines during graduation, new technologies are not available and the visual method is the most used. It is known that this method of diagnosis gives sensitivities to the order of 60.0% and a specificity of 85.0% 6. Nevertheless, the current diagnostic model of visual is qualitative, subject to operator interpretation, and consequently can produce varied diagnosis from dentists examining the same patient 19.
To conduct the clinical examination of caries it is necessary that the teeth are clean, dry and well lit. In this study, all photographs were taken by obeying these criteria. Thus, for all surfaces this alternative was considered correct for all clinical situations. The percentage of correct responses was high for all clinical situations ranging from 65.06% to 92.77% (Table IV). The detection of early signs of caries cannot be achieved unless the teeth are clean and dry 11.
The use of dental probing for occlusal caries detection causes enamel defects 12,24. This study did not evaluate how probing is being used whether appropriate or not. However, the results showed that probing was the second most appropriate method to aid in the diagnosis for all dental surfaces (Table III). In another study, the authors reported that the use of the probe is the main clinical diagnostic method used 10.
The difficulties in the accurate diagnosis of occlusal caries only by visual examination have been highlighted in the literature. Thus, bitewing radiographs should complement the diagnosis of clinical appearance. However, this is only valid whether cavities are found in dentine obviously. For the diagnosis of occlusal caries in enamel this method is inaccurate 15. The results showed a low percentage of responses for this method in the diagnosis of all conditions of occlusal surface, including the healthy surfaces (Table III). However, it was observed a higher percentage of answers for periapical radiographs as a diagnostic method. A smaller percentage of students answered that associated methods assist in diagnosis (Table III).
With regard to the type of treatment recommended for areas classified as healthy, a little over half of the students would not perform any treatment (53.01%), followed by glass ionomer cement (33.73%) or resin-based sealant (10.84%) of pits and fissures, or preventive restoration (2.41%). If the tooth belonged to a child at risk for dental caries, all the treatments mentioned, except performing preventive restoration were considered correct responses (Table IV).
Considering the surface that had white spots difficult to see, all treatments were considered and glass ionomer cement sealant was indicated (46.99%). On the other hand, for the surface with visible white spots, all treatments were cited, except for performing conventional restoration. In this clinical situation, sealing with glass ionomer cement was also the most appropriate treatment (61.45%). The use of glass ionomer cement sealant is justified by the fact that it has been recommended by the school of dentistry. All treatments were chosen for the occlusal surface with enamel caries, with the highest percentage (63.31%) for no treatment (Table IV). These results are in agreement with other study 5 in which the therapeutic method adopted in cases of clinical occlusal caries without cavitation, showed significant differences between the teacher and students.
A distinct stage in the caries process is the formation of the cavity. When a carious cavity is formed, it is much more difficult to control biofilm by oral hygiene procedures. Thus, the treatment of choice usually involves surgical intervention in the form of restorations 21. For the treatment options cited for cavity in dentine, performing conventional (65.06%) and conservative restoration (33.73%) (Table IV) were recommended.
The diagnosis of occlusal caries is highly subjective, with considerable variation in the ability and experience among clinicians to diagnose and treat occlusal caries appropriately 10. However, the correct diagnosis of the condition of the occlusal surface allows adequate treatment. In this present study, all students who correctly classified the condition of occlusal surface indicated the correct treatment (Table V).
It seems that students of 6th period had a greater number of correct answers than those from 7th and 8th periods. Meanwhile, there were no statistically significant differences among the students (Table V). Methodological differences make difficult to compare these results with those of other studies.
According to the results, considering all answers, it was observed that students at 7th and 8th semesters showed a higher number of correct answers compared to those at 6th semester (Figure 3). There was no statistically significant increasing in correct answers, among the percentages obtained by students at the three semesters.
It was concluded that the opinion of students differed regarding the diagnosis and treatment mainly as the occlusal surface showed early stages of dental caries. According to Coelho et al. 5 there is a real need to reduce the divergences and disagreements of therapeutic diagnosis to benefit the patient. The implementation of teaching/learning strategies based on constant training/calibration process is needed to minimize these variations and to contribute to professional's formation 18.
References
1. Angnes G, Angnes V, Grande RHM, Battistella M, Loguercio AD, Reis A. Occlusal caries diagnosis in permanent teeth: an in vitro study. Braz Oral Res. 2005 Oct-Dec;19(4):243-8. [ Links ]
2. Bader JD, Shugars DA. The evidence supporting alternative management strategies for early occlusal caries and suspected occlusal dentinal caries. J Evid Base Dent Pract. 2006 Mar;6(1):91-100.
3. Bobrowski R, Schneider M. Divergence between diagnostic healthy, biological sealing and occlusal caries in enamel or enamel and dentine, carried out by academics and dental professionals. Stomatos. 2001 Jan-Jun;17(32):43-54.
4. Braga MM, Mendes FM, Ekstrand KR. Detection activity assessment and diagnosis of dental caries lesion. Dent Clin N Am. 2010 Jul;54(10):479-93.
5. Coelho LT, Silveira ADS, Lima KC, Pinheiro IVA. Occlusal decay without cavitation: divergency on the therapeutic decision. Odontologia Clin Cient. 2007;6(1):39-43.
6. Dodds MWJ. Dillemas in caries diagnosis – applications to current practice and need for research. J Dent Educ. 1993 Jun;57(6):433-8.
7. Ekstrand KR, Ricketts DN, Kidd EA. Reproducibility and accuracy of three methods for assessment of demineralization depth of the occlusal surface: an in vitro examination. Caries Res. 1997;31(3):224-31.
8. Ekstrand KR, Ricketts DNJ, Kidd EAM. Occlusal caries: pathology, diagnosis and logical management. Dental Update. 2001 Oct;28(8):380-7.
9. Ekstrand KR, Ricketts DNJ, Kidd EAM, Qvist V, Schou S. Detection, diagnosing, monitoring and logical treatment of occlusal caries in relation to lesion activity and severity: an in vivo examination with histological validation. Caries Res. 1998;32(4):247-54.
10. Gordan VV, Riley III JL, Carvalho RM, Snyder J, Sanderson Jr JL, Anderson M et al. Methods used by dental practice-based research network (DPBRN) dentists to diagnose dental caries. Operative Dent. 2011 Jan-Feb;36(1):2-11.
11. Ismail AI. Visual and visuo-tactile detection of dental caries. J Dent Res. 2004;83(Spec Iss C):C56-66.
12. Künisch J, Dietz W, Stösser L, Hickel R, Heinrich-Weltzien R. Effects of dental probing on occlusal surfaces – a scanning electron microscopy evaluation. Caries Res. 2007;41(1):43-8.
13. Louvain MC, Miasato JM, Piassi E, Damasceno LM. Dentist's conduct concerning occlusal caries diagnosis. J Bras Odontopediatr Odontol Bebê. 2000 Jan-Feb;4:45-9.
14. McComb D, Tam LE. Diagnosis of occlusal caries: Part I. Conventional methods. J Can Dent Assoc. 2001 Sep;67(8):454-7.
15. Mejàre I, Kidd EAM. Radiography for diagnosis of decay. In: Fejerskov O, Kidd E. Dental caries: the disease and its clinical management. 2. ed. São Paulo: Santos; 2011. p. 69-88.
16. Mestriner SF, Vinha D, Mestriner Junior W. Comparison of different methods for the occlusal dentine caries diagnosis. J Appl Oral Sci. 2005 Mar;13(1):28-34.
17. Mialhe FL, Silva RP, Ambrosano GMB, Pereira AC, Ferreira AC. Occlusal caries detection and its treatment by public health services dentists. RFO. 2007 Sep-Dec;12(3):29-34.
18. Mialhe FL, Silva RP, Pereira AC, Ambrosano GMB, Alvez WF. Variability in detection of caries and treatment plans between students of dentistry. Rev Odontol Unesp. 2008;37(4):345-50.
19. Milicich G. Clinical applications of new advances in occlusal caries. New Zealand Dental J. 2000 Mar;96(423):23-6.
20. Nyvad B. Diagnosis versus detection of caries. Caries Res. 2004;38(3):192-8.
21. Nyvad B, Fejerskov O, Baelum V. Visual-tactile detection of dental caries. In: Fejerskov O, Kidd E. Dental caries: the disease and its clinical management. 2. ed. São Paulo: Santos; 2011. p. 49-68.
22. Pereira AC, Eggerston H, Martinez-Mier EA, Mialhe FL, Eckert GJ, Zero DT. Validity of caries detection on occlusal surfaces and treatment decisions based on results from multiple caries-detection methods. Eur J Oral Sci. 2009 Feb;117(1):51-7.
23. Souza-Zaroni WC, Ciccone JC, Souza-Gabriel AE, Ramos RP, Corona SAM, Palma-Dibb RG. Validity and reproducibility of different combinations of methods for occlusal caries detection: an in vitro comparison. Caries Res. 2006;40(3):194-201.
24. Yassin OM. In vitro studies of the effect of a dental explorer on the formation of an artificial carious lesion. J Dent Child. 1995 Mar-Apr;62(2):111-7.
25. Zandoná AF, Zero DT. Diagnostic tools for early caries detection. J Am Dent Assoc. 2006 Dec;137(12):1675-84. 2.
 Corresponding author:
Corresponding author:
Fabiana Sodré de Oliveira
Universidade Federal de Uberlândia
Avenida Pará, 1.720 – Bloco 2G – sala 2 – Campus Umuarama
CEP 38400-902 – Uberlândia – MG – Brasil
E-mail: fasoliv@yahoo.com.br
Received for publication: January 31, 2013
Accepted for publication: November 5, 2013
