










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.2 Joinville Abr./Jun. 2014
ORIGINAL RESEARCH ARTICLE
Bacterial infiltration comparison of two root canal filling techniques
Gislaine Pontarollo I; Raphael Hamerschmitt I; Beatriz Coelho I; Denise Piotto Leonardi I; Flávia Sens Fagundes Tomazinho I
I School of Dentistry, Positivo University – Curitiba – PR – Brazil
ABSTRACT
Introduction: Root canal system filling aims to the hermetic sealing of the space formerly occupied by the dental pulp. Objective: The aim of this study was to analyze the bacterial infiltration of Enterococcus faecalis in root canals filled through two techniques: single cone technique (group A) and thermoplasticized gutta-percha technique (group B). Material and methods: A total of 40 single-rooted human premolars were divided into two experimental groups (n = 15) and two control groups: positive (n = 5) and negative (n = 5). The root canals were prepared with ProTaper Universal system up to size F3 file and filled with the corresponding gutta-percha point. Teeth were mounted on a dual-chamber model, where the infiltration of E. faecalis was evaluated for a 30-day period by BHI turbidity indicating bacterial growth. Results: After the trial period all specimens in experimental and positive control groups showed turbidity of the culture medium. The average number of days until culture medium turbidity was 11.42 days for group A, 16.69 days for group B, and 5.5 days for positive control. By applying Anova test, there was no statistically significant difference between groups (p > 0.05). This allowed the observation that no difference between the obturation techniques in the infiltration of E. faecalis could be observed by the methodology used. Conclusion: It can be concluded that regardless of the obturation techniques, bacterial infiltration occurred.
Keywords: Endodontics; root canal obturation; dental leakage.
Introduction
Endodontic treatment success is linked to the maintenance of the sanitation obtained after root preparation. Root canal obturation must eliminate the empty spaces hindering recontamination 10.
The exposure of the filling material to oral cavity may be one of the causes of endodontic treatment failure. This can occur in different clinical situations, such as the loss of the temporary restoration, fracture of tooth crown, marginal leakage of the definitive restoration and secondary caries, enabling bacterial infiltration throughout the filling material 3.
Although gutta-percha has been not considered as the ideal material, it is the main solid material to fill the root canal system and displays its best performance when associated with the endodontic cement. Root canal filling must comprise a greater gutta-percha amount and the cement should fill root canal irregularities and be the linking between the solid material and the dentinal walls. However, the areas filled by cement are more vulnerable because of the cement solubility 7,18.
The filling technique may influence on bacterial leakage of root canals. Although most of the researches have accepted gutta-percha, the main discussion is about its utilization way. Techniques have been proposed aiming to decrease the operative time and the material consumption and, of course, improve the characteristics of root canal sealing. Thus, many different filling techniques using gutta-percha have appeared 22,25.
With the advancement of automatized preparation techniques of root canals, the gutta-percha points taper have matched that of nickel-titanium rotary systems used for root canal preparation, so that, at the moment of the canal filling, only one main gutta-percha point is used per canal, which makes unnecessary the use of accessory points and decrease the filling time 10.
In these cases, according to the manufacturers' instructions, after the use of shaping instruments, one should employ only the point matching the size of the last instrument used for the apical preparation of root canal, surrounded by cement, because this point have the standardized size exactly matching that of the shaping achieved by instrumentation 5,21.
Oval-shaped canals or canals presenting morphologies different from those of the current systems tend not to be totally filled by a single gutta-percha point. In these canals, the instruments are not capable of cleaning all root canal areas, resulting in a round-shaped preparation. Singlecone obturation will allow many spaces filled by cement, compromising the obturation sealing and enabling bacterial infiltration 6,24.
The sealing by resin cements directly influences on the obturation quality. These cements have exhibited good quality, optimum capacity of bonding to dentin and gutta-percha, low solubility, dimensional stability, radiopacity, low contraction, and good leakage resistance 12,17.
Considering that the ideal obturation would be the filling of root canal system with the greatest volume of solid material as possible 18, techniques of thermoplasticized gutta-percha have been advocated for root canal obturation because they can provide a more homogenous obturation with better adaptation to root canal walls, resulting in a smaller root leakage infiltration in comparison with lateral condensation technique 2,13.
The aim of this study was to determine which obturation technique is the most effective in preventing bacterial infiltration by E. faecalis: single-cone or thermoplasticized gutta-percha technique.
Material and methods
This study was approved by the Ethical Committee in Research of Positivo University under protocol no. 028/12.
Forty single-rooted human premolars with straight roots were obtained in the tooth bank of Positivo University and used in this study (Curitiba, Paraná, Brazil).
The 40 teeth were divided into four groups: two experimental groups, each one with 15 teeth; two control groups, positive and control group with five teeth each. The teeth of the experimental and positive control groups were prepared and filled, while those from negative control group remained sound.
The coronal portion of the teeth was cut with the aid of a diamond disc and the length of the roots was standardized at 13 mm.
The roots were instrumented by nickel-titanium rotary instruments (Protaper Universal, Dentsply Maillefer, Ballaigues, Switzerland), following the manufacturer's recommendations, with working length (WL) set at 12 mm. Prior to the use of the rotary system, root canal negotiation and instrumentation was accomplished with hand stainless steel size #10 and #15 K files at WL. Rotary instrumentation was performed with the aid of electrical motor (X-Smart, Dentsply Maillefer, Ballaigues, Switzerland) at speed of 300 RPM and torque of 1.6N, with the following file sequence: sizes S1 and S2 at WL; size SX up to the medium third; final preparation by sizes F1, F2 and F3 at WL. At every instrument change, root canal was irrigated with 2 ml of 2.5% sodium hypochlorite (DanaFarma Farmácia de Manipulação, Curitiba, Brazil).
After the complete preparation, root canal was filled with 17% EDTA (DanaFarma, Paraná, Brazil), for five minutes, aiming to remove the smear layer formed during root canal instrumentation. 17% EDTA was removed by 2.5% sodium hypochlorite. Next, root canals were dried with the aid of size F3 absorbent paper points (Dentsply Maillefer, Rio de Janeiro, Brazil) at working length.
The external portion of all roots were waterproofed with two layers of nail polishing at 3 mm shorter of the apex, except for the teeth of negative control groups that had all roots waterproofed.
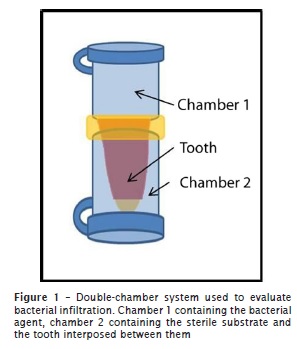
Eighty 1.5 ml Eppendorf tubes were used to achieve a system composed of three parts; an upper chamber, a lower chamber, and the tooth between them (figure 1). This set was sterilized in autoclave at temperature of 121ºC for 20 min.
The teeth of the experimental groups were randomly divided into two groups (n = 15) and then filled by two different techniques. Endodontic cement was AH Plus (Dentsply, Rio de Janeiro, Brazil). Group A (n = 15) – Protaper system single cone; group B (n = 15) –thermoplasticized Protaper system single cone. Positive control group (n = 5) was filled with size F3 single cone without cement and negative control group (n = 5) used sound teeth.
After root canal obturation, the samples were kept in incubator for 24 hours, at 100% humidity at 37°C, to allow the proper cement setting.
To evaluate the bacterial infiltration, E. faecalis (ATCC 19433) from the American Type Culture Collection was used. The microorganisms were cultivated in 5 ml of BHI broth. Test tubes containing BHI broth with the microorganisms already grown were adjusted with the aid of the same broth to the tube number 2 of McFarland Standards, at concentration of about 6x108 cells/ml. The upper chamber was filled with the bacterial solution and the lower chamber with sterilized BHI broth.
The specimens were incubated at 37°C, at proper respiratory conditions for 30 days. The culture medium was renewed at every 72 hours by removing all content of the upper chamber and replacing it by sterilized culture medium. Daily, for 30 days, all specimens were carefully agitated to verify the presence or absence of turbidity of the lower chamber, which would be and indicative of bacterial infiltration through the filling material. When the samples displayed turbidity, indicating bacterial infiltration, they were separated from the others.
Anova test was applied to verify whether there would be statistical differences between groups (p < 0.05).
Results
All specimens of positive control group showed culture medium turbidity at the first ten days. Conversely, negative control group did not show turbidity evidences at all experimental period. Four of 40 samples were excluded during all study, comprising three of group A and one of negative control group because of the failure of the device during the renewing of the culture medium.
The viability of the inoculum was proved after the experimental period (30 days). At the 30th experimental day, 12 upper chamber samples (four for each group) was randomly seeded on BHI plates, to prove the inoculum viability during the study. In all specimens showing turbidity, the microorganism found was identical to that initially inoculated. In all specimens displaying E. faecalis infiltration, the observation of the laminas revealed morphotinctorial features similar to those observed at the beginning of the study.
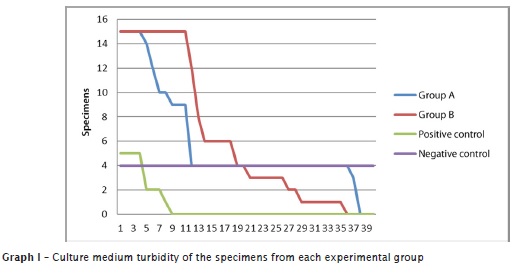
After the experimental period, all specimens of groups A, B and positive control group showed culture medium turbidity. The mean of days for culture medium turbidity was 11.42 days for group A, 16.69 days for group B and 5.5 days for positive control group.
Data of each group was compared through Anova test using SPSS software.
Anova test did not show statistically significant differences (p > 0.05) between groups, so that it can be affirmed that there were no differences between the filling techniques employed in relation to E. faecalis infiltration.
Graph 1 demonstrated the specimens infiltrated and the days elapsed.
Discussion
The endodontic treatment aims at the cleaning and shaping of root canal. After these steps, it is necessary to seal the root canal to keep the sanitation obtained during preparation. The sealing maintain the condition achieve by root canal preparation and is of great importance for endodontic treatment success.
Many in vitro methods have been used to evaluate the sealing capacity of root canal obturation by employing dyes, scanning electronic microscopy, techniques of infiltration of fluids, electrochemical methods, radioisotopes and bacterial infiltration 4,8,14,23.
Among these techniques, the model of bacterial infiltration is one of the most used due to the clinical relevance. This present employed E. faecalis because this microorganism has been associated with many dental infections and identified as the bacterial species more commonly found in root canals showing failures after endodontic treatment. It is a species very used in many studies on bacterial infiltration 3,8,9,16,24.
This present study was designed to evaluate in vitro the bacterial infiltration in root canals prepared with Protaper Universal system and filled by two different techniques (single cone and thermoplasticized single cone techniques). The teeth were carefully selected, standardizing the tooth group, number and curvature of canals, root and working lengths, aiming to decrease the number of variables.
The teeth used were the mandibular premolars because they have shown a varied morphology displaying either round- or oval-shaped canals. Because of these anatomical variations the proper cleaning, shaping and filling of root canals can be compromised and result in unsatisfactory long-term outcomes 6. Oval-shaped canals would have a greater amount of cement between gutta-percha point and root canal wall, making bacterial infiltration easier 6,24.
The double-chamber system (upper chamber + tooth + lower chamber) used in this present study was based on the model of the studies of De-Deus et al. 6, Brosco et al. 3, Ito et al. 10, Kangarlou et al. 11, Şimşek et al. 19, Alkahtani et al. 1 and Navarro-Escobar et al. 15, in which all had a chamber containing the bacterial agent and a chamber containing the sterile substrate with a tooth between them to simulate an environment contaminated in the upper chamber, the root with the root exposed to this environment, and the root apex exposed to a sterile culture medium in the lower chamber, and the only access was through the filled root canal.
The results of four studies confirmed the validity of the double-chamber system because both the experimental and positive control groups exhibited culture medium turbidity at different time periods, while the negative control group did not show turbidity during all experimental period.
This study employed ProTaper Universal nickel-titanium rotary system to prepare the root canal. In these cases, root canal filling according to the manufacturers' recommendations can be accomplished by using only the gutta-percha point matching the size of the last instrument used for the apical preparation because the size of the point is standardized in relation to the shaping left by the instrumentation 5,21.
The aforementioned description is which has been so-called single-cone technique which has allowed a faster and easier obturation because it used only one gutta-percha point. On the other hand, this technique cannot fill the morphological variations of oval-shaped root canals, which would not be completely filled by gutta-percha, requiring a greater cement amount, leading to root canal sealing failure 5.
To overcome the filling deficiency of single-cone technique, the thermoplasticization of the gutta-percha point can be obtained. This technique aims to improve gutta-percha adaptation to the morphological variations of root canal, thus achieving a sealing with greater gutta-percha and smaller cement amounts 20.
The results of this present study evaluating the root canal sealing capacity through two techniques demonstrated no statistical differences between them in relation to bacterial infiltration. This result corroborates that obtained by Damasceno et al. 5, Tasdemir et al. 21 and Ito et al. 10, which observed no statistically significant differences between different techniques of root canal filling regarding to bacterial infiltration.
In the study of Yücel et al. 24 and Monticelli et al. 13, a better sealing capacity was observed with thermoplasticized gutta-percha technique compared with single-cone technique. These outcome differences could have occurred because of the aforementioned authors employed System B and Thermafill in gutta-percha thermoplasticization, which may increase the adaptation to root canal walls.
Conclusion
Based on the methodology employed and on the results obtained, it can be concluded that both obturation techniques did not show significant differences between them in relation to the method of bacterial infiltration by E. faecalis.
References
1. Alkahtani A, Al-Subait A, Anil S. An in vitro comparative study of the adaptation and sealingability of two carrier-based root canal obturators. The Scientific World Journal. 2013;1-7. [ Links ]
2. Brosco VH, BernardinelIi N, Moraes IG. "In vitro" evaluation of the apical sealing of root canals obturated with different techniques. Journal Applied Oral Science. 2003;3(11):181-5.
3. Brosco VH, Bernardineli N, Torres SA, Consolaro A, Bramante CM, Moraes IG et al. Bacterial leakage in root canals obturated by different techniques. Part 1: microbiologic evaluation. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2008;1(105):48-53.
4. Cobankara FK, Asanir N, Belli S, Pashley DHA. Quantitative evaluation of apical leakage of four root-canal sealers. International Endodontic Journal. 2002;9(35):79-84.
5. Damasceno JHN, Silva PG, Queiroz ACFS, Vardasca de Oliveira PT, Pereira KFS. Estudo comparativo do selamento apical em canais radiculares obturados pelas técnicas cone único Protaper e termoplástica sistema TC. Revista Gaúcha de Odontologia. 2008;4(56):417-22.
6. De-Deus G, Murad C, Paciornik S, Reis CM, Coutinho-Filho T. The effect of the canal-filled area on the bacterial leakage of oval-shaped canals. International Endodontic Journal. 2008(41):183-90.
7. Dultra F, Barosso JM, Carrasco LD, Capelli A, Guerisoli DMZ, Pécora JD. Evaluation of apical microleakage of teeth sealed with four different root canals sealers. Journal Applied Oral Science. 2006;5(14):341-5.
8. Er K, Tasdemir T, Bayramoglu G, Herguner-Siso S. Comparison of the sealing of different dentin bonding adhesives in root-end cavities: a bacterial leakage study. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2008;9(106):76-82.
9. Fransen JN, He J, Glickman GN, Rios A, Shulman JD, Honeyman A. Comparative assessment of ActiV GP/glass ionomer sealer, Resilon/Epiphany, and gutta-percha/AH plus obturation: a bacterial leakage study. Journal of Endodontic. 2008;72(34):5-7.
10. Ito DL, Shimabuko DM, Aun CA, Brum TB. Avaliação da infiltração bacteriana em técnicas de obturação do canal radicular. Revista de Odontologia da Universidade Cidade São Paulo. 2010;3(22):198-215.
11. Kangarlou A, Dianat O, Esfahrood ZR, Asharaf H, Zandi B, Eslami G. Bacterial leakage of GuttaFlow-filled root canals compared with Resilon/Epiphany and Gutta-percha/AH26-filled root canals. Australian Endodontic Journal. 2012;1(38):10-3.
12. Martins AS, Ostroski MM, Silva Neto UX, Westphalen VPD, Frainiuk LF, Moraes IG. Avaliação in vitro da infiltração via coronária em função de diferentes cimentos endodônticos resinosos. Revista Odonto Ciência. 2006;52(21):179-84.
13. Monticelli F, Sadek FT, Schuster GS, Volkmann KR, Looney SW, Ferrari M et al. Efficacy of two contemporary single-cone filling techniques in preventing bacterial leakage. Journal of Endodontic. 2007;3(33):310-3.
14. Nagas E, Altundasar E, Serper A. The effect of master point taper on bond strength and apical sealing ability of different root canal sealers. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;1(107):e61-4.
15. Navarro-Escobar E, Baca P, González-Rodríguez MP, Arias-Moltz MT, Ruiz M, Ferrer-Luque M. Ex vivo microbial leakage after using different final irrigation regimens with chlorhexidine. Journal Applied Oral Science. 2013;1(21):74-9.
16. Paradella TC, Koga-Ito CY, Jorge AOC. Enterococcus faecalis: considerações clínicas e microbiológicas. Revista de Odontologia da UNESP. 2007;2(36):163-8.
17. Pinheiro CR, Guinesi AS, Camargo EJ, Pizzolitto AC, Bonetti-Filho I. Bacterial leakage evaluation of root canals filled with different endodontic sealers. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;6(108):56-60.
18. Shilder H. Filling root canals in three dimensions. Journal of Endodontic. 2006;4(32):281-90.
19. Şimşek N, Akpinar KE, Sümer Z. Evaluation of bacterial microleakage of root canals irrigated with different irrigation solutions and KTP laser system. Photomedicine and Laser Surgery. 2006;1(31):3-9.
20. Tanomaru-Filho M, Bosso R, Sant'anna-Júnior A, Berbert FLCV, Guerreiro-Tanomaru JM. Effectiveness of gutta-percha and Resilon in filling lateral root canals using thermomechanical technique. Revista de Odontologia da UNESP. 2013;1(42):37-41.
21. Tasdemir T, Er K, Yildri T, Buruk K, Çelik D, Cora S et al. Comparison of the sealing ability of three filling techniques in canals shaped with two different rotary systems: a bacterial leakage study. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;3(108):129-34.
22. Yilmaz Z, Deniz D, Ozcelik B, Sahnin C, Cimilli H, Cehreli ZC et al. Sealing efficiency of BeeFill 2 in 1 and System B/Obtura II versus single-cone and cold lateral compaction techniques. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;6(108):51-9.
23. Yilmaz Z, Tuncel B, Ozdemir HO, Serper A. Microleakage evaluation of roots filled with different obturation techniques and sealers. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;12(108):4-8.
24. Yücel AÇ, Çiftçi A. Effects of different root canal obturation techniques on bacterial penetration. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2006;4(102):88-92.
25. Williamson AE, Marker KL, Drake DR, Dawson DV, Walton RE. Resin-based versus gutta-percha-based root canal obturation: influence on bacterial leakage in an in vitro model system. Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontic. 2009;2(108):292-6.
 Corresponding author:
Corresponding author:
Flávia Sens Fagundes Tomazinho
Rua Curupaitis, n. 474 – Seminário
CEP 80310-180 – Curitiba – PR – Brasil
E-mail: flavia.tomazinho@gmail.com
Received for publication: November 12, 2013
Accepted for publication: December 12, 2013
