










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.2 Joinville Abr./Jun. 2014
ORIGINAL RESEARCH ARTICLE
In vitro study of the morphology of internal lower second molars
Humberto Ramah Menezes de Matos I; Luanni Belmino Mastroianni I; Aldo Angelim Dias II
I Discipline of Endodontics, School of Dentistry, University of Fortaleza – Fortaleza – CE – Brazil
II School of Dentistry, University of Fortaleza – Fortaleza – CE – Brazil
ABSTRACT
Introduction: The mandibular molars are a group of teeth that have a complex internal morphology, and its fundamental knowledge is necessary. The second molar has two roots, one mesial and distal, but three canals are more commonly find: two in the mesial root and one in the distal root. Objective: To study through four criteria: radiographic, clinical, microscopic, and anatomy, the internal morphology of the mandibular second molars. Material and methods: This was a cross-sectional, in vitro, descriptive, observational study, in which 50 second molars were selected, having as exclusion criteria teeth destroyed by caries. Inclusion criteria comprised teeth with higid and semi-higid crowns Results: 299% of mandibular second molars had three canals. The round-shaped cross section was the most common throughout the cervical-apical extension of both mesial (59% ) and distal (47%) canals. However, other possible configurations and number of canals can be found in second molars, as the presence of four (12%) or five canals (3%). 36.7% of the mesial canals and 29.4% of distal canals were flattened in the mesial-distal direction and elongated in buccolingual direction; the variation of the "C-shaped" canal was found in 4% of cases. Conclusion: The most frequent configuration and number of canals of mandibular second molars were, respectively, the round-shaped cross section configuration in the entire length of the canal, and three canals. However the professional should be aware that this morphology may vary as shown in each research phase. Therefore, to achieve clinical success, the professional should have the knowledge of the internal morphology of these teeth and their possible variations.
Keywords: molar; Endodontics; pulp cavity.
Introduction
Endodontics has been through marked changes of concepts, such as the use of a single instrument for biomechanical preparation and innovative filling techniques. However, established aspects should not be left behind, such as the knowledge on the internal morphology of all teeth and possible variation that may be found; the negotiation of the root canal system with the adequate instruments; the biomechanical preparation that provides the maximum of canal disinfection; maintenance of apical foramen patency and its original position; a filling providing an adequate sealing of root canal systems.
The complexity in root canals, mainly in molars, is directly linked to recurrent infections. If the morphology of root canals is not known by the dentist and endodontist, treatment failure will be eminent, even using latest technology instruments, because root canals not properly negotiated and prepared may shelter infectious foci. Thus, the knowledge of internal morphology and its possible variation should be ample both for the dentists and the endodontists, during the execution of the endodontic intervention.
The mandibular second molar has two roots: a mesial and a distal one; but, it is more common to find three root canals: two in mesial root and one in distal root 15,18. A common variation in these teeth is "C shape" canal that is so named because of the root and canal cross section 5,7. Instead of exhibiting the entrances of different root canals, the pulp chamber floor presents a ribbon-shaped canal, with 180 degree arch, starting from the mesial-lingual line extending around of the buccal surface to the distal portion of the pulp chamber 10. Almeida-Gomes et al. 2 affirmed that the previous diagnosis and knowledge of "C-shape" canals are much valuable for the clinical success of the case. Jafarzadeh and Wu 10 affirmed that the diagnosis of this morphological variation can be of difficult conclusion through radiographic examination; however, clinical examination is more accurate in its diagnosis.
Malvar and Corbacho 14 studied the internal morphology of 81 second molars by diaphanization. The authors observed the number of roots, main canals, lateral canals, inter-canals and apical. The mesial root exhibited a prevalence of two different canals and the distal root the greater frequency of only one canal.
The interna l morpholog y doma in is a fundamental step during endodontic therapy, because the adequate preparation of the canal system would avoid the increasing of failure rates. Thus, the aim of this in vitro study was to assess the amount and possible configurations of the canals within mandibular second molars through radiographic, clinical, microscopic and morphological methods.
Material and methods
This present research is an in vitro, descriptive, observational study. All phases were carried out in laboratory with the use of freshly extracted teeth, that is, in vitro. Fifty mandibular second molars were selected after their removal due to therapeutic indication because of either aggressive periodontal disease with great loss of clinical insertion or orthodontic/prosthodontic reasons, whose detailed history is part of the patients' files. Inclusion criteria were teeth either sound or with carious lesion. Teeth were excluded because of lack of anatomical crown due to severe destruction, regardless of the reason causing such loss; and previous endodontic treatment. This study was submitted and approved by the Ethical Committee in Research of the University of Fortaleza (Coética/UNIFOR) under protocol no. #181.388/12.
After selection, all teeth were submitted to the methods of this present study (radiographic, clinical, microscopic and morphological).
Radiographic assessment
The teeth were fixed with wax to the periapical intraoral film (Kodak Insight, USA). Next, a radiographic shot was executed for 0.22 second. To enable the observation of all root canals, an angle of 20 degrees at horizontal plane towards mesial surface of the teeth was employed to mimic Clark's positioning technique, which corresponds a distortion at the horizontal angle of the x-ray beam incidence to prevent image superposition of root canals, improving their observation 8. This technique reproduces which would be possible to execute during the clinical treatment, thus enabling a better observation of the root canals.
The film development was carried out in dark chamber for two minutes within developing solution. Following, they were removed and immersed in water for 20 seconds; then the films were fixed for five minutes. The radiographs were immersed in running water for five minutes and left to dry. Only after this sequence, they were evaluated on negatoscope to evaluate the amount of canals of each tooth. The teeth in which the film was not properly exposed or in which the radiographic image not allowed a correct distortion were again exposed to correct the error and make possible an adequate assessment.
Clinical assessment
All procedures of access and exploration of the pulp chamber were executed by the same operator, previously trained during a pilot study with the same methodology employed in the study.
Firstly, pulp chamber access of the sound teeth was executed with the aid of n. 1013 diamond bur (KG Sorensen, Barueri, Brazil), coupled to high-speed handpiece (Kavo model 605c, Joinville, Brazil). The diamond point was changed at every 30 teeth, to assure its correct use. The initial penetration was performed on the center of the central sulcus of the occlusal surface with the drill parallel to the tooth long axis, obtaining a contour shape according to the tooth morphology 12. For the teeth presenting carious lesion contour shape was defined according to the extension of the carious tissue, which was removed with the aid of a round carbide drill (KG Sorensen, Barueri, Brazil) with size compatible with that of the cavity, changed at every 30 teeth, coupled to a micro motor and contra-angle at low speed (Kavo model 161 and model 2068, respectively).
After this procedure, the roof of the pulp chamber was removed and the surrounding walls became more divergent towards occlusal, with the aid of Endo Z drill at high speed (Dentsply Maillefer, Ballaigues, Switzerland), aiming at making easy the direct view, illumination and access of the pulp chamber.
After the conclusion of the access, a straight explorer was used to examine the pulp chamber floor to find all the entrances of the present root canals. Aiming at improving the observation of the found root canals, a file sequence was employed to enlarge the entrances of the canals, starting from sizes #8 and #10 (Dentsply-Maillefer, Ballaigues, Switzerland), followed by size #15 Kerr file (Dentsply-Maillefer, Ballaigues, Switzerland), #20 and #25 Flexofile files (Dentsply-Maillefer, Ballaigues, Switzerland), changed at every tooth groups. Sodium hypochlorite solution at 2.5% concentration (Biodinâmica, Ibiporã, Brazil) was employed during all negotiation phase of root canals.
Microscopic assessment
The visual magnification was executed through an optical microscope (DF Vasconcellos M900, Rio de Janeiro, RJ, Brazil), which improves the floor observation. All teeth were visualized with the aid of the microscope at x16 visual magnification so that the canals not identified could have been visualized and also to confirm more precisely the number of canals.
Microscopic assessment without anatomical crown
Aiming at a better identification of the canals, since atresic canals are difficult to be observed, in this study an anatomical cut of the crown was executed by the same operator.
The anatomical cuts of the crowns were executed at the anatomical neck with the aid of no. 2200 diamond point (KG, Sorensen Barueri, Brazil); this was changed at every tooth groups and coupled to high-speed handpiece (Kavo model 605c). After the cutting of all teeth, each tooth was stored into colorless plastic bags correctly numbered according to the tooth number. The observation and exploration with straight explorer was carried out under visual magnification (optical microscopy at x16 magnification), enabling the identification of root canals that possibly were not identified during clinical access. Root canals found during this step were negotiated by the aforementioned file sequence.
Results
Through the methodology employed, it was possible to observe regarding to the amount of root canals, a difference according to the assessment type executed, with variations in the number of canals found at each step (graph 1).
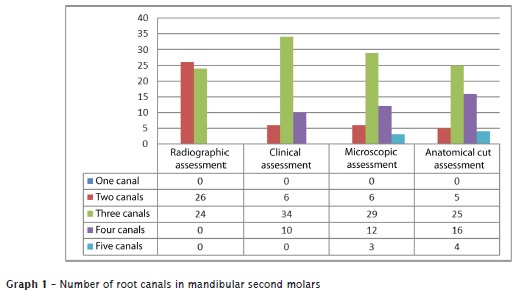
The prevalence of teeth with three canals was noted. Notwithstanding, through the microscopic and anatomical assessments, the amount of four canals increased, making possible to find cases with five canals.
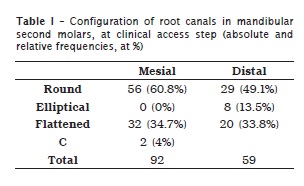
With regard to the configurations of root canals, the radiographic examination (step 1) did not allow to analyze the shape of canals, so that their morphology was established at the subsequent steps. The configuration with the greatest percentage was round-shape canals in both roots, defined during the clinical assessment step (table 1).
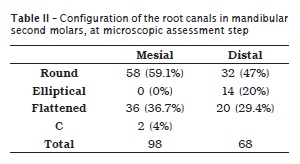
Only two cases of mandibular second were found with "C-shaped" configuration. At the third step of the study, in which visual magnification was used after pulp chamber access, it could be observe an increase in the relative frequencies due to the increase of the number of root canals found (table 2).
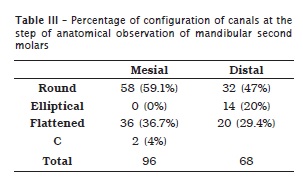
At the step of anatomical observation, some percentages were maintained, while others changed because of the possibility that not previously seen root canals were found after the removal of the anatomical crowns, which allowed a better illumination quality of the pulp chamber floor (table 3).
Discussion
In this present study, most frequently, the mandibular second molars exhibited round-shaped canals and three canals, respectively regarding to the configuration and number. The relevance of such configuration for endodontic practice is advantageous in relation to the shaping achieved by the instruments after biomechanical preparation, minimizing the percentage of instrument fracture due to torsion, because round-shaped configuration would avoid that the instrument's tip were apprehended in the walls due to the shape similar to that of the file13.
It was demonstrated that the conventional radiographic method limits the identification of canals even without image superposition and with angle standardization for all studied teeth. Current studies have affirmed that only the two-dimensional analysis of radiographs did not provide an accurate diagnosis of the internal morphology of the canals because of image superimposition, contrast and angulation limitations. Other factor limiting the identification of canals is the professional's expertise. Notwithstanding, even the most experienced professional could not identify changes in root canal system. Thus, the current researches have proposed a new auxiliary method to help in identifying atresic and calcified canals, and isthmus areas, which is computed tomography 4,11,17,19.
Carvalho and Zuolo 3 conducted an in vivo study to evaluate 93 mandibular first and 111 second molars regarding to the number of root canals. At the first appointment, pulp chamber exploration was performed with naked eye, finding 641 canals. At the second appointment, visual magnification through optical microscopy was used, and more 50 canals were found – accounting for an increase of 7.8%. The authors concluded that the use of the optical microscope help in identifying the canals not observed by conventional clinical examination.
Through the aid of visual magnification (optical microscope) after the clinical access and cut of the anatomical crown, it was observed an increasing of the number of canals identified, which is in agreement with previous authors. This demonstrates that the optical microscope help in the identification the canals not observed by conventional clinical examination.
Malvar and Corbacho 14 studied the internal morphology of 81 mandibular second molars through diaphanization. The authors observed the number of roots; main and recurrent canals, inter-canals, and apical deltas. They noted that in the mesial roots, there was a greater prevalence of two different canals extending from pulp chamber to the apex. For the distal root, one canal extending from pulp chamber to the apex was more frequently found. In this present study, most of the teeth showed three canals, two mesial and one distal. The presence of teeth with four and five canals after the last step of the study increased; however, it was lower than the amount of teeth with three canals.
Cooke and Cox 6 were the first authors to report a case of "C-shaped" mandibular second molar and affirmed that such variation occur in 8% of the cases. Studies on mandibular second molars have shown that the occurrence of "C-shaped" canals may range among populations: between 2.7% and 7.6% in Caucasians, 6% among Arabs, 14% among Lebanese and 31.5% among Chinese 1,9,16,20,21. The percentage of "C-shaped" canals in this present study was of 4%, which is lower than the percentage reported by Cooke and Cox.
The radiographic examinations, even with their limitations, should be used to aid in identifying morphological variations and in choosing resources and materials to be used during endodontic therapy. The access to pulp chamber should be performed allowing an adequate observation of the chamber floor aiming to identify the canals and their configurations. The negotiation of root canal systems should be executed through proper instruments, since it is one of the most important treatment stages and the morphology domain would make ease the subsequent operative steps.
Visual magnification provided by optical microscopy helps to identify atresic and calcified root canals and it can be an auxiliary tool of endodontic armamentarium. The result of the knowledge and domain of the internal morphology will be the increasing of endodontic treatment success rates.
Conclusion
It was possible to verify that, regarding to configuration, round-shaped cross section prevailed in mandibular second molars, probably because of the conical shape of the roots. The three-canal specimens were the most found; however, with the aid of visual magnification through optical microscope, the identification of teeth with both four and five canals increased during the observation of atresic root canal entrances. A prevalence of "C-shaped" canals was similar to that reported in literature, of approximately 4%.
References
1. Al Fouzan KS. C-shaped root canals in mandibular second molars in a Saudi Arabian population. J Endod. 2002;35(6):49999-504. [ Links ]
2. Almeida-Gomes F, Maniglia-Ferreira C, Lima Guimarães NLS, Alves dos Santos R, Vitoriano MM. "C shape canal": uma variação anatômica de interesse clínico. Rev Bras Pesq Saúde. 2010;12(2):57-60.
3. Carvalho MCC, Zuolo ML. Orifice locating with a microscope. J Endod. 2000;26(9):523-4.
4. Chandra SS, Rajasekaran M, Shankar P, Indira R. Endodontic management of a mandibular first molar with three distal canals confirmed with the aid of spiral computerized tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(4):77-81.
5. Cleghom BM, Cristie WH, Don CC. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod. 2006;32(9):813-21.
6. Cooke HG, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc. 1979;99(5):836-9.
7. Fan B, Cheung GS, Fan M, Gutmann JL, Fan W. C-shape canal system in mandibular second molars: part II – radiographic features. J Endod. 2004;30(12):904-8.
8. Freitas A, Rosa JE, Faria e Souza I. Radiologia odontológica. 6. ed. São Paulo: Artes Médicas; 2004.
9 . Haddad GY, Nehme WB, Ounsi HF. Diagnosis, classification, and frequency of C-shaped canals in mandibular second molars in the Lebanese population. J Endod. 1999;25(4):268-71.
10. Jafarzadeh H, Wu Y. The c-shaped root canal configuration. J Endod. 2007;33(5):517-23.
11. Lee S, Jang KH, Spangberg LS, Kim E, Jung IY, Lee CY et al. Three-dimensional visualization of a mandibular first molar with three distal roots using computer-aided rapid prototyping. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;11(5):383-8.
12. Lopes HP, Siqueira Jr JF. Endodontia: biologia e técnica. 3. ed. Rio de Janeiro: Guanabara-Koogan; 2010.
13. Maia Filho EM, Souza EM, Meneses EO, Rizzi CC. Effect of Gates Glidden, La Axxess, SX and ultrasound on the circularity and area of mesial canals of mandibular molars. RSBO. 2013;10(3):234-9.
14. Malvar MFG, Corbacho MM. Estudo da anatomia interna de segundos molares inferiores pela técnica da diafanização. J Bras Endo. 2002;3(11):337-41.
15. Navarro LF, Luzi A, Garcia AA, García AH. Third canal in the mesial root of permanent mandibular first molars: Review of literature and presentation of 3 clinical reports and 2 in vitro studies. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;12(8):605-9.
16. Sabala CL, Benenati FW, Neas BR. Bilateral root or root canal aberrations in a dental school patient population. J Endod. 1994;20(1):38-42.
17. Toubes KM, Côrtes MI, Valadares MA, Fonseca LC, Nunes E, Silveira FF. Comparative analysis of accessory mesial canal identification in mandibular first molars by using four different diagnostic methods. J Endod. 2012;38(4):436-41.
18. Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics. 2005;10(1):3-29.
19. Villas-Bôas MH, Bernardineli N, Cavenago BC, Marciano M, Del Carpio-Perochena A, de Moraes IG et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod. 2011;37(5):1682-6.
20. Weine FS. The C-shaped mandibular second molar: incidence and other considerations. J Endod. 199998;24(5):372-5.
21. Weine FS, Pasiewicz RA, Rice RT. Canal configuration of the mandibular second molar using a clinically oriented in vitro method. J Endod. 1988;14(5):207-13.7.
 Corresponding author:
Corresponding author:
Humberto Ramah Menezes de Matos
Rua Bill Cartaxo, n. 885 – casa 16 – Água Fria
CEP 60833-185 – Fortaleza – CE – Brasil
E-mail: beto_meneses@hotmail.com
Received for publication: July 22, 2013
Accepted for publication: December 16, 2013
