










Serviços Personalizados
Artigo
 pdf em Inglês
pdf em Inglês Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailLinks relacionados
Compartilhar

 Permalink
PermalinkRSBO (Online)
versão On-line ISSN 1984-5685
RSBO (Online) vol.11 no.2 Joinville Abr./Jun. 2014
Case Report Article
Hypochlorite-induced severe cellulitis during endodontic treatment: case report
Bernardo Almeida Aguiar I; Fábio Almeida Gomes II; Cláudio Maniglia Ferreira II; Bruno Carvalho de Sousa III; Fábio Wildson Gurgel Costa IV
I Department of Endodontics, Center of Dental Specialties Odontológicas Ícaro de Souza Moreira – Sobral – CE – Brazil
II Department of Endodontics, Fortaleza University – Fortaleza – CE – Brazil
III Department of Endodontics, Federal University of Ceará – Campus Sobral – Sobral – CE – Brazil
IV Department of Oral Radiology and Stomatology, Federal University of Ceará – Campus Sobral – Sobral – Brazil
ABSTRACT
Introduction: Sodium hypochlorite is a solution used in endodontic treatment, and if an accidental apical extrusion occurs, serious complications may affect soft tissue. Objective: The aim of this article is to present a case of apical extrusion of sodium hypochlorite (NaOCl) during root canal system instrumentation. Case report: A 28-year-old woman sought a local dental service for root canal treatment of tooth #24. Conventional endodontic treatment was adopted, which consisted of the use of 2.5% NaOCl solution as irrigation solution applied with a 10-ml syringe and 22G hypodermic needle. At that time, the patient reported extreme pain and a burning sensation in the left maxillary region, followed by the formation of intense edema. A clinical diagnosis of hypochlorite-induced cellulitis was made. The patient was treated immediately with amoxicillin (500 mg, orally) at intervals of 8 h for 7 days and dexamethasone (4 mg, intramuscularly) at intervals of 24 h for 3 days. In the subsequent endodontic treatment, 2% chlorhexidine gel applied with a 5-ml syringe and 24G needle was used as irrigation for a better control of treatment and to prevent new accidents. The root canals were instrumented using adequate crown-down technique, which provides a conical shape, and filled by lateral condensation technique. The patient was symptom free at the 8-month clinical follow-up. Conclusion: Dentists should always carefully follow all stages of dental treatment planning without neglecting any of them, paying attention to the solutions used and their storage as well as performing a specific technique with maximum accuracy. If an accident occurs, the appropriate handling of the situation will enable the satisfactory completion of treatment.
Keywords: sodium hypochlorite; root canal treatment; complications; management.
Introduction
Sodium hypochlorite (NaOCl) is a commonly used irrigation solution in root instrumentation, showing the property of dissolving organic tissue 7,8. Accidental apical extrusion of NaOCl during endodontic canal preparation can cause serious soft tissue complications 2. These complications are probably a consequence of the alkaline and hypertonic nature of different NaOCl solutions that have cytotoxic effects, causing tissue damage especially at concentrations higher than 0.01% 15.
Several problems have been associated to NaOCl toxicity, including soft tissue and bone necrosis 14 ulceration 7, facial nerve disturbance 16, as well as inhibited neutrophil migration, hemolysis and damage to endothelial and fibroblast cells 2,4,9. Forty nine cases of NaOCl accidents were reviewed from the literature and added a case in which NaOCl was mistaken for anesthetic solution and infiltrated into the buccal mucosa during routine root canal treatment 13. We recently attended a healthy adult woman who developed important facial cellulitis during a conventional endodontic treatment. The purpose of this case is to present a serious problem that may occur during irrigation of root canal, discuss how to avoid it and present a protocol suitable for solving the problem of effective and safe manner.
Case report
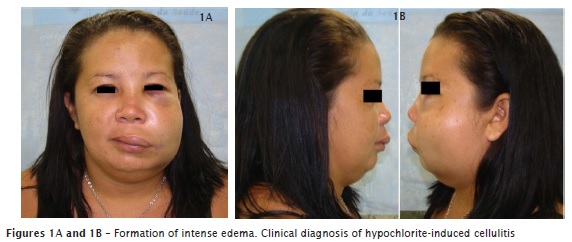
A 28-year-old woman sought a local dental service for root canal treatment of tooth #24. Diagnosis radiograph showed two canals in this tooth, no periapical lesion and clinical diagnosis was irreversible pulpitis. Conventional endodontic treatment was adopted, which consisted of the use of infiltrative anesthesia and endodontic access. Radiographic odontometry was performed using technique of changing the horizontal angle of incidence to avoid overlapping of root canals. Instrumentation was performed using step down technique with K-type files and file Gates Glidden drills. Solution of choice for irrigation of the root canal system was 2.5% sodium hypochlorite, with 10ml disposable hypodermic syringe and 22G disposable needle. 17% EDTA was applied for 3 minutes at the end of preparation, and its removal was performed with a solution of 2.5%sodium hypochlorite. Either the crash or obstruction of the needle in irrigation canals was not noticed. At that time, the patient reported extreme pain and a burning sensation in the left maxillary region, followed by the formation of intense edema. Thus, a clinical diagnosis of hypochlorite-induced cellulitis was made (figures 1A and 1B).
The patient received oral analgesic and was referred to a endodontist at the Acaraú Center for Dental Specialties (Brazil). Examination revealed the presence of extensive facial cellulitis, submandibular and infraorbital ecchymosis, and severe trismus. The patient was treated immediately with amoxicillin (500 mg, orally) at 8 h intervals for 7 days and dexamethasone (4 mg, intramuscularly) at 24 h intervals for 3 days. After one week, clinical evaluation revealed edema reduction. However, the painful symptoms were still present and restricted mouth opening prevented any treatment of the affected tooth. Finally, complete remission of the symptoms was observed after 21 days (figures 2A and 2B).

With the remission of signs and symptoms, endodontic treatment was resumed. It was observed that the instrumentation previously performed promoted excessive expansion of the apical foramen, and conformation and wide cylindrical root canals. This fact favors the flow of solution through the foramen. Chlorhexidine gel was applied with a 5-ml syringe and 24G needle was used as irrigant for a better control of treatment and to prevent new accidents. The root canals were instrumented using the more adequate crown-down technique, which provides a conical shape. Apical preparation was finished with size # 50 K type files, in both canals, 1 mm short of the apical foramen, determined through the use of an electronic apex locator (Root ZX II, J Morita, Japan). Finally, canals were filled by lateral condensation technique (figure 3). The patient was revalued after 8 months and remained asymptomatic.

Discussion
Careful mechanical instrumentation of the root canal system associated to a copious irrigation is a fundamental step during endodontic treatment 7. Effective irrigating solution is important to remove debris formed during instrumentation, to act as a lubricant for instruments, and to remove the smear layer produced after mechanical instrumentation 4,11,17.
In this present case, several factors have contributed to the accidental injection of NaOCl through the apical foramen. First, it was not used an electronic apex locator to assist the process of determining the apical limit of instrumentation. When only radiographic technique is used to perform this step, an apical limit can be determined incorrectly, because this technique does not identify the location of the apical foramen, but the position of the radiographic apex.
Second, inspection of the root canals showed excessive enlargement of the apical foramen, in which an endodontic K-file #40 was positioned without difficulty. This event favors the extravasation of irrigation solution. In addition, the canals presented a cylindrical instead of a conical shape, a fact favoring snug fit of the irrigation needle that in this present case had a large caliber (22G) that prevented reflux of the irrigation solution. Electronic odontometry showed that both the palatine and buccal canal had a length of 17 mm, a value considered to be short for the upper premolars. The failure to observe this short length also favored the accidental injection of the irrigation solution into the periapical tissues. The in vitro extrusion of 5.25% NaOCl solution through the apical foramina of mesial-buccal root canals of maxillary first molars was analyzed. According to authors, 5.25% NaOCl solution showed a great capacity to extrude beyond intact and small-sized apical foramina of mesial-buccal root canals of upper first molars, as apical extrusion occurred with and without previous use of patency files of different sizes 3. Other study showed positive correlation between the amount of extrusion into the apical tissues and endodontic technique-related factors (apical preparation size and the method of activation and delivery of NaOCl into the apical one-third 12.
The principal harm is to the cells because they are dependent on the specic uid environment in which they are found; NaOCl changes that environment, causing cellular necrosis and apoptosis. The damaged matrix can then become a nidus for infection. Trabecular bone was damaged by the toxic effects of NaOCl 10.
The antibiotic treatment has been used in this case to prevent an opportunistic infection in the periapical tissue necrosis, and thereby protect the patient from infection that could be installed and aggravate the already complicated case.
Careless use of NaOCl solutions has been associated with different complications during or after endodontic treatment, ranging from accidental injection into periapical tissues and maxillary sinuses, accidental injection instead of an anesthetic solution and seepage through lateral root perforations to allergic reactions 3. An interesting study among the professionals of the American Board of Endodontics 11 revealed some common findings related to these complications: prevalence of women, maxillary and posterior teeth have been more affected, clinical diagnosis of pulp necrosis with periradicular radiolucency in the associated tooth, complete resolution of patient symptomatology within a month, and no changes in the prognosis of the involved tooth.
The management of complications following NaOCl irrigation to periapical tissues has been well described in the literature 9,14,16. We agree with the next topics: 1) following an accident with NaOCl, the professional must be calm and should explain to the patient about what happened; 2) initially it is recommended the use of cold compresses that should be replaced by warm compresses after a 24 hour period; 3) according to severity of the case, antibiotics may be necessary; 4) the patient should be advised about the range in the healing process; 5) after remission of acute symptoms, endodontic treatment may be continued; 6) NaOCl solution should be replaced by a non-irritant irrigation solution 9.
Different substances have been used as alternative irrigation solutions, such as lower concentrations of NaOCl, chlorhexidine, and electrochemically active water 5. In this present case, we used chlorhexidine as irrigation solution to prevent new accidents. Knowledge about the length and integrity of the root canal system before irrigating procedure is essential to avoid complications 4.
Although the substance that caused local toxicity in the present case was different from that reported on another study 6 in which facial cellulitis was due to inadvertent injection of formalin instead of the local anesthetic, both cases demonstrate the possibility of dental treatment failures even when apparently conventional techniques are used.
Conclusion
Dentists should always carefully follow all stages of dental treatment planning without neglecting any of them, paying attention to the solutions used and their storage as well as performing a specific technique with maximum accuracy. And if even with all these precautions an accident happens, a protocol comprising appropriate intervention and patient following-up will allow the reversal of the unfavorable situation and satisfactory completion of therapy.
References
1. Basrani B, Haapasalo M. Update on endodontic irrigating solutions. Endod Topic. 2012;27:74-102. [ Links ]
2. Brown DC, Moore BK, Brown Jr CE, Newton CW. An in vitro study of apical extrusion of sodium hypochlorite during endodontic canal preparation. J Endod. 1995;21:587-91.
3. Camoes IC, Salles MR, Fernando MV, Freitas LF, Gomes CC. Relationship between the size of patency file and apical extrusion of sodium hypochlorite. Ind J Dent Res. 2009;20:426-30.
4. De Sermeño RF, da Silva LA, Herrera H, Herrera H, Silva RA, Leonardo MR. Tissue damage after sodium hypochlorite extrusion during root canal treatment. Oral Surg Oral Med Oral Pathol Oral Rad Endod. 2009;108:46-9.
5. Gernhardt CR, Eppendorf K, Kozlowski A, Brandt M. Toxicity of concentrated sodium hypochlorite used as an endodontic irrigant. Inter Endod J. 2004;37:272-80.
6. Gupta DS, Srivastava S, Tandon PN, Jurel S, Sharma S, Singh Jr S. Formalin-induced iatrogenic cellulitis: a rare case of dental negligence. J Oral Max Surg. 2011;69:525-7.
7. Gursoy UK, Bostanci V, Kosger HH. Palatal mucosa necrosis because of accidental sodium hypochlorite injection instead of anesthetic solution. Inter Endod J. 2006;39:157-61.
8. Haapasalo M, Shen Y, Qian W, Gao Y. Irrigation in endodontics. Dent Clin North Am. 2010;54: 291-312.
9. Hülsmann M, Hahn W. Complications during root canal irrigation – literature review and case reports. Inter Endod J. 2000;33:186-93.
10. Kerbl F, DeVilliers P, Litaker M, Eleazer P. Physical effects of sodium hypochlorite on bone: an ex vivo study. J Endod. 2012;38:357-9.
11. Kleier DJ, Averbach RE, Mehdipour O. The sodium hypochlorite accident: experience of diplomates of the American Board of Endodontics. J Endod. 2008;34:1346-50.
12. Mitchell RP, Baumgartner JC, Sedgley CM. Apical extrusion of sodium hypochlorite using different root canal irrigation systems. J Endod. 2011;37:1677-81.
13. Motta MV, Chaves-Mendonça MA, Stirton CG, Cardozo HF. Accidental injection with sodium hypochlorite: report of a case. Inter Endod J. 2009;42:175-82.
14. Pontes F, Pontes H, Adachi P, Rodini C, Almeida D, Pinto Jr D. Gingival and bone necrosis caused by accidental sodium hypochlorite injection instead of anaesthetic solution. Inter Endod J. 2008;41:267-70.
15. Serper A, Ozbek M, Calt S. Accidental sodium hypochlorite-induced skin injury during endodontic treatment. J of Endod. 2004;30:180-1.
16. Witton R, Henthorn K, Ethunandan M, Harmer S, Brennan PA. Neurological complications following extrusion of sodium hypochlorite solution during root canal treatment. Inter Endod J. 2005;38:843-8.
17. Young GR, Parashos P, Messer HH. The principles of techniques for cleaning root canals. Austr Dent J. 2007;52:S52-63.
 Corresponding author:
Corresponding author:
Bruno Carvalho de Sousa
Rua Andrade Furtado, n. 1.245 – ap. 602 – Cocó
CEP 60192-072 – Fortaleza – CE – Brasil
E-mail: brunendo@hotmail.com
Received for publication: March 27, 2013
Accepted for publication: September 10, 2013
